
Abstract
Myopericytoma (MPC) of the oral cavity is extremely rare. Herein reported is a case of MPC of low grade malignancy in the oral cavity. A 61-year-old man noticed a tumor of the cheek mucosa, and admitted to our hospital. Oral examination revealed a reddish elevated tumor of the cheek mucosa. Tumorectomy with wide margins was performed. The clinical diagnosis was pyogenic granuloma. Grossly, the tumor was reddish, and measured 1×1×1 cm. Microscopically, oval to spindle tumor cells with hyperchromatic vesicular nuclei and many vasculatures were seen. The tumor cells were contiguous and mixed with endothelial cells in many blood vessels, thus resembling pericytes. Mitotic figures were scattered. The surgical margins were negative for tumor cells. Immunohistochemically, the tumor cells were positive for vimentin, α-smooth muscle actin and p53. The Ki67 labeling was 40%. The tumor cells were negative for cytokeratins (AE1/3 and CAM5.2), CD31, CD34, S100 protein, HMB45, CD10, vimentin, desmin, and factor VIII-related antigen. The endothelium of the vessels were positive for vimentin, CD31, CD34 and factor VIII-related antigen, but negative for α-smooth muscle actin, p53, cytokeratins (AE1/3 and CAM5.2), S100 protein, HMB45, CD10, vimentin, and desmin. The Ki67 labeling was 5%. Because the pericytoid tumor cells showed α-smooth muscle actin and negative for endothelial markers, MPC was diagnosed. In addition, because there was some atypia and mitotic figures were scatters and also because the tumor cells were positive for p53 and Ki67 labeling was high, a pathological diagnosis of MPC with low grade malignancy was made. No recurrence was observed, and the patient is now free from tumor 6 months after the operation.
Introduction
Myopericytoma (MPC) is defined a benign tumor that is composed of oval to spindle shaped myoid appearing cells with a striking tendency concentric perivascular growth. 1 It is believed that the lesional cells show apparent differentiation towards myoid cells or myopericytes. However, malignant counterpart of MPC, i.e. malignant MPC, has been reported. 2 MPC of the oral cavity is extremely rare; only several cases have been reported in the literature.3–6 In addition, malignant MPC has not been reported in the oral cavity. Herein reported is a case of MPC of low grade malignancy in the oral cavity.
Case Report
A 61-year-old man complained of a tumor of the right cheek mucosa, and consulted to our hospital. Oral examination revealed a reddish elevated tumor of the right cheek mucosa. The clinical diagnosis was pyogenic granuloma. Tumorectomy with wide margins was performed. Grossly, the tumor was reddish, and measured 1×1×1 cm (Figure 1A). Microscopically, oval to spindle tumor cells with hyperchromatic vesicular nuclei and many vasculatures were seen (Figure 1B and 1C). The tumor cells were contiguous and mixed with endothelial cells in many blood vessels, thus resembling pericytes (Figure 1B and 1C). Mitotic figures were scattered (Figure 1C). No angiomatous, leiomyomatous, fibromatous areas were recognized. The surgical margins were negative for tumor cells.
Histolopathology of the tumor. A) Very low power view shows vascular tumor measuring 1×1×1 cm, Haematoxylin & Eosin, x10; B) low power view of the tumor shows pericytomatous pattern, Haematoxylin & Eosin, x 100; C) high power view of the tumor shows ooal to spindle tumor cells with hyperchromatic nuclei located around the vessels. Mitotic figures are scattered (arrows). Haematoxylin & Eosin, x200.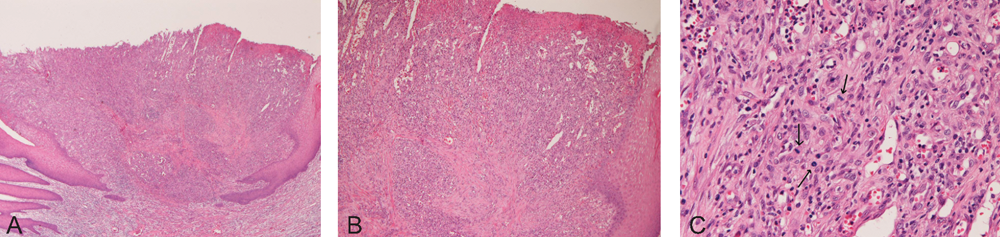
An immunohistochemical study was performed with the use of Dako's EnVision method, as previously described.7,8 Immunohistochemically, the tumor cells were positive for vimentin, α-smooth muscle actin (Figure 2A) and p53 (Figure 2B). The Ki67 labeling was 40% (Figure 2C). The tumor cells were negative for cytokeratins (AE1/3 and CAM5.2), CD31, CD34 (Figure 2D), S100 protein, desmin, HMB45, CD10, vimentin, and factor VIII-related antigen. The endothelium of the vessels were positive for vimentin, CD31, CD34 (Figure 2D) and factor VIII-related antigen, but negative for α-smooth muscle actin, p53, cytokeratins (AE1/3 and CAM5.2), S100 protein, HMB45, CD10, vimentin, and desmin. The Ki67 labeling was 5%. Because the pericytoid tumor cells showed α-smooth muscle actin and were negative for endothelial markers, MPC was diagnosed. In addition, because the tumor cells had atypia and mitotic figures and immunohistochemically were positive for p53 and Ki67 labeling was high, a pathological diagnosis of MPC with low grade malignancy was made. No recurrence was observed, and the patient is now free from tumor 6 months after the operation.
The tumor cells are positive for α-smooth muscle actin (A), p53 (B), and Ki67 (labeling=40%), but negative for CD34 (C). The blood vessels’ endothelial cells are positive for CD35 (D). Immunostaining, x200.
Discussion
The present tumor was parivascular cell tumor, and the tumor cells were positive for α-smooth muscle actin.
Thus, the tumor is compatible with MPC, though concentric tumor cell arrangement was not obvious. MPC belongs to a spectrum of disease entity; perivascular myoid cell neoplasm. 9 This entity includes perivascular tumors such as Glomus tumor, MPC, myofibroma, infantile hemangioendothelioma. Similar related tumors are solitary fibrous tumor, angioleiomyoma, and hemangiopericytoma.
The present tumor is not Glomus tumor, because the tumor cells were not epithelioid. The present tumor is different from myofibroma because fibromatous areas were not seen. The present tumor is different from infantile hemangioendothelioma because of the age and histology. The current tumor is different from solitary fibrous tumor because of the histology and lack of CD34. The current tumor is different from angioleiomyoma because of the lack of leiomyomatous element. The present tumor is different from perivascular epithelioid cell neoplasm, such as Pecoma, because of the histology and negative HMB45. Thus the present tumor appears to be MPC.
In the present case, there was cellular atypia of the tumor cells, and mitotic figures were scattered. In addition, p53 was positive and Ki67 showed high (40%) labeling. These findings suggest that the present tumor is low grade malignancy. Therefore, the present tumor seems MPC of low grade malignancy.
Most cases of MPC behave in a benign fashion, but local recurrence and rarely metastases may occur in atypical and malignant MPC. 10 In the current case, the follow-up period is only 6 months. Because the current MPC appears to be low grade malignancy, strict follow-up is need.
In conclusion, the author presented an extremely rare case of MPC of low grade malignancy in the oral cheek mucosa.