
Abstract
We present a case of an intramedullary melanotic schwannoma (IMS) of the thoracic spinal cord. To our knowledge, this is the seventh reported case of an IMS of the central nervous system. Schwannomas are benign nerve sheath tumors of neural crest origin composed entirely of well differentiated Schwann cells that typically occur in peripheral nerves. Both the intramedullary location and the melanotic component of the reported lesion make it exceedingly rare. We will present our case, theories as to the origin of these tumors, clues in radiographic identification, and current clinical follow-up recommendations.
Case Report
Presentation and history
The patient is a 62-year-old female with a several year history of aching in both thighs. Three months prior to presentation she began having radicular pain in the thighs. The pain was worse when standing and walking. She denied significant back pain. She reported reduced strength in the legs and numbness in her legs to the dorsum of her feet, urinary urgency, and urinary incontinence.
Physical examination
Her examination demonstrated mild (4 out of 5) weakness of the iliopsoas and hamstrings bilaterally. Temperature and pain sensation was reduced below the T12 level. She had mild difficulty with tandem walking.
Initial diagnosis and radiography
Magnetic resonance imaging (MRI) of the thoracic spine revealed a 1.2×1.0×1.1 cm intramedullary mass posterior to the T11 vertebral body within the spinal canal (Figures 1–3). There was spinal cord expansion and edema above and below the mass evidenced by T2 hyperintensity. The lesion was T1 hyperintense and T2 hypointense.
A) Sagittal T1 magnetic resonance imaging without gadolinium contrast; B) Sagittal T2 magnetic resonance imaging.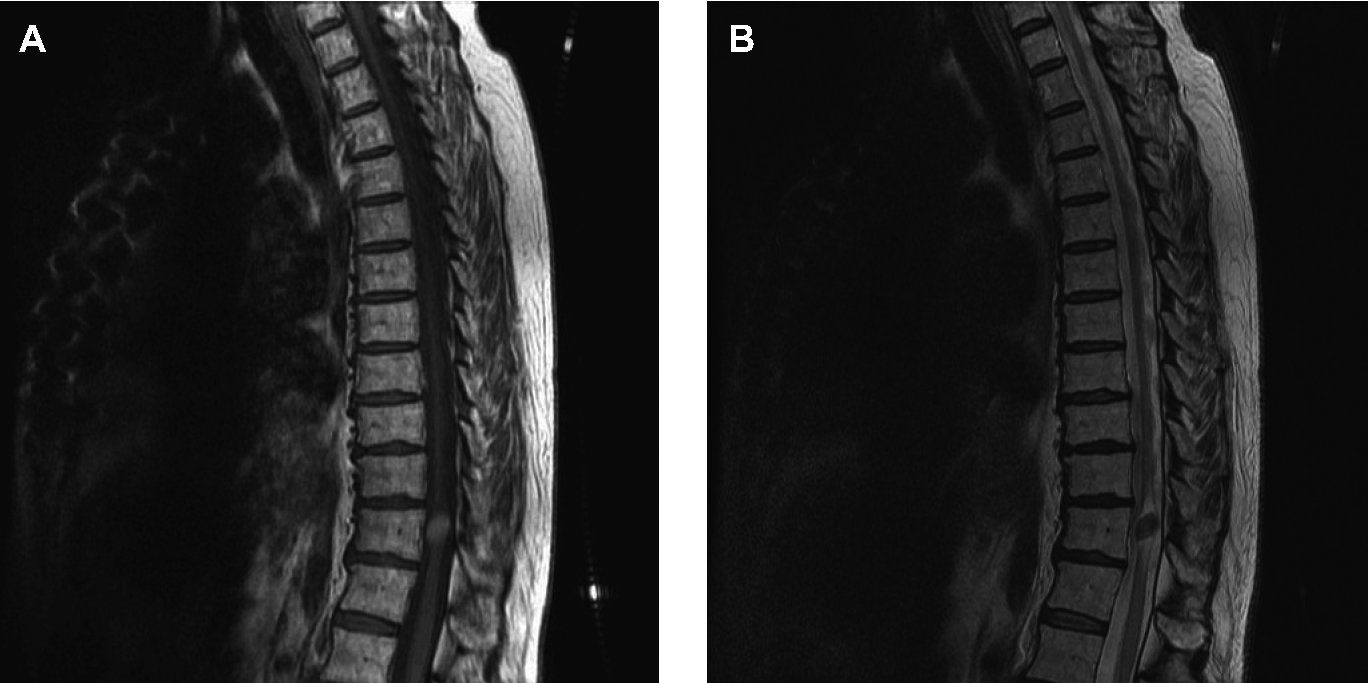
Axial T2 magnetic resonance imaging fast spin echo at A) T11 (cephalad); B) T11 (middle); C) T11 (caudal).
A) Sagittal T1 magnetic resonance imaging with gadolinium contrast; B) axial T1 magnetic resonance imaging with gadolinium contrast at T11.
Operative course
The patient underwent T10-T11 laminectomies. The dura was thinned posteriorly where the lesion presented intradurally. Dark pigmentation was visible through the dura. The dura was opened in the midline exposing an intramedullary lesion reminiscent of a cavernous malformation (Figure 4). The lesion was carefully resected from the surrounding cord and sent whole for pathological analysis (Figure 5).
Intra-operative photograph.
Gross specimen.
Pathology
Hematoxylin and eosin staining was performed and demonstrated a heavily pigmented spindle cell neoplasm suggestive of a melanotic schwannoma (Figure 6). Tumor cells stained with antibodies to melan-A (Figure 7). MIB-1 labeling index was very low, although difficult to interpret due to the dark pigmentation of the tissue (not shown). A collagen IV stain was positive and a reticulin stain revealed a dense reticular pericellular network (not shown) suggesting the presence of a pericellular basement membrane as typical of well differentiated Schwann cells. Electron microscopy, in addition to intracellular late stage melanosomes, demonstrated the presence of a continuous pericellular basal lamina confirming the schwannian nature of the cells (Figure 8). Thus, the diagnosis of intramedullary melanotic schwannoma (IMS) was made.
Hematoxylin and eosin stain.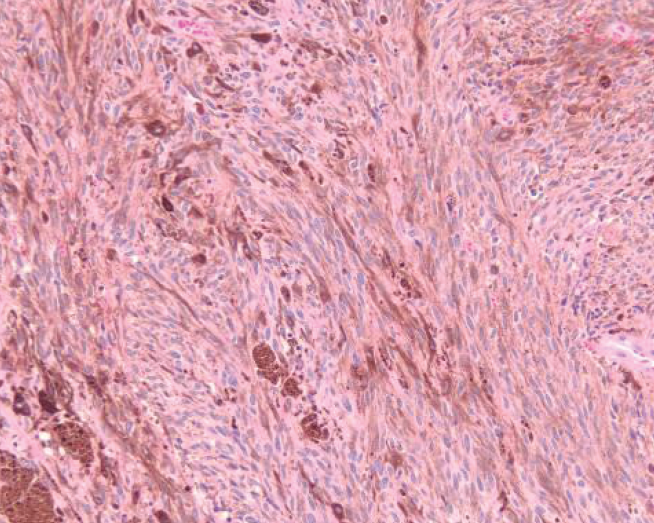
Melan-A stain.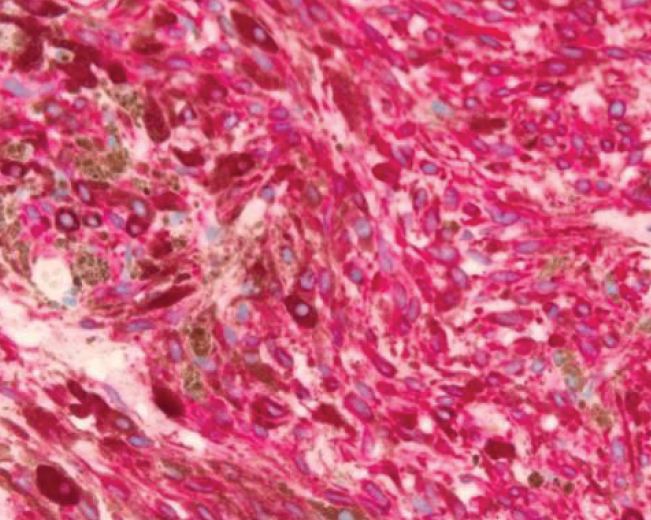
Spindled cells, numerous late-stage melanosomes, predominantly stage IV); surrounded by a characteristic single continuous basal lamina.
Post-operative course
Immediately postoperatively, the patient had weakness in the proximal left leg. She had diminished sensation to light touch and temperature in the right leg. Her strength and sensation in the lower extremities improved over the following days and the patient was subsequently transferred to inpatient rehabilitation. A post-operative MRI performed three months after surgery revealed no evidence for residual or recurrent tumor (Figures 9A and 9B). Since a gross total resection was confirmed radiographically, we did not recommend any adjuvant treatment. We recommended close clinical and radiographic observation with semi-annual MRI's.
A) Sagittal T1 magnetic resonance imaging without gadolinium contrast (postoperative); B) sagittal T2 magnetic resonance imaging (post-operative).
Ten months post-operatively the patient had resolution of her neurogenic bladder symptoms and was voiding spontaneously. She was able to walk at least a half block with a walker. Her neurologic exam revealed diffuse mild corticospinal weakness in the lower extremities bilaterally with spasticity in the right lower extremity. She had bilateral plantar extensor responses. The patient had sensory deficits in the lower extremities resulting in sensory ataxia.
Discussion
Schwannomas are benign nerve sheath tumors, which display advanced Schwann cell differentiation and are the most common type of peripheral nerve tumor in adults, prevalent in those 30–50 years old without gender predilection. 1 Most extracranial schwannomas are sporadic rather than associated with neurofibromatosis type 2. They are often slow growing masses that can occur anywhere distal to the oligodendroglial-Schwann cell myelination junction. 1 The intramedullary location, as in this case, is rare for schwannomas.
The melanotic appearance of the reported intramedullary schwannoma is also a rare entity involving cytoplasmic deposition of melanin from functional melanosomes. Theories explaining the melanin producing properties of these cells include neoplastic differentiation of neural crest cells into Schwann cells with melanogenetic properties and melanocytic transformation of previously normal Schwann cells. 2 These tumors typically occur in the spinal nerves and ganglia. The presence of psammoma bodies is typical of the psammomatous variant of melanotic schwannoma, a tumor which most frequently occurs in the autonomic nerves and viscera, including the intestinal tract and heart. Approximately 50% of patient with psammomatous melanotic schwannomas are affected by the Carney complex, an autosomal dominant disorder with coexisting morbidities such as cardiac myxomas. 3 Carney complex involves skin pigmentary abnormalities, myxomas, endocrine tumors or overactivity, and schwannomas. The psammomatous melanotic schwannoma occurs in an estimated 10% of affected individuals affected by the Carney complex. 4
IMS is a very rare entity. This is only the 7th reported case to our knowledge describing this tumor (Table 1).2,5–9 Various explanations for this tumor's unusual location in the central nervous system have been put forth (Table 2).6,8,10–13
Summary of reported cases.

Presumed etiologies of intramedullary melanotic schwannoma.

MRI is the preferred method of evaluating lesions of the spine cord. Melanotic lesions will appear hyperintense on T1weighted images and hypointense on T2 weighted images due to paramagnetic free radicals in melanin. 14 In contrast, non-melanotic tumors are hypointense on T1 weighted images and hyperintense on T2 weighted images and chronic hematomas are hyperintense on both T1 and T2 weighted images which help to differentiate the melanotic from non-melanotic lesions. However, there can be some difficulty in differentiating subacute hematomas from melanotic lesions since they share similar characteristics on MRI. 15 This is what most likely led to the initial radiographic diagnosis of cavernous malformation in our case.
MRI characteristics of intramedullary schwannomas are fairly inconsistent. Administration of gadolinium can cause nodular enhancement of schwannomas when cystic components are present, but is mainly useful in differentiating intramedullary schwannomas from spinal cord edema.12,16 A confident diagnosis of intramedullary schwannoma can be made preoperatively when there is continuity of the intramedullary lesion with a contrast enhancing thickened spinal root. 12
Complete surgical excision of intramedullary schwannomas is considered curative, effective, and safe. Schwannomas are normally benign encapsulated tumors. In contrast, approximately 10% of melanotic schwannomas have been reported to pursue an aggressive clinical course with local recurrence and metastases including seeding of the subarachnoid space.2,14 The presence of multiple lesions however is not synonymous with seeding since multiple independent schwannomas may occur. Whenever possible, complete resection and careful follow-up should be practiced with any melanotic schwannoma regardless of location. Radiotherapy following subtotal resection of an intramedullary melanotic schwannoma is recommended due to the tumor's potential for recurrence and metastasis. 17 In our experience, melanotic lesions of the spinal cord may behave in an unpredictable fashion. While we do not believe radiotherapy is necessary when a gross total resection is possible and postoperative MRI confirms this, we recommend close MRI follow-up. It is our usual practice to image spinal cord tumors annually following surgical resection; we shorten this interval to six months, at least initially, for melanotic tumors of the spinal cord.
Conclusions
MRI is the preferred method for evaluating lesions of the spine cord. Melanotic lesions will appear T1 hyperintense and T2 hypointense due to paramagnetic free radicals in melanin. In contrast, non-melanotic tumors are T1 hypointense and T2 hyperintense. There can be some difficulty in differentiating early subacute hematomas from melanotic lesions and this may lead to an initial radiographic diagnosis of cavernous malformation. IMS are rare and their behavior is unpredictable. Gross total resection is the goal in neurosurgical treatment since recurrence and malignancy are possibilities.