
Abstract
Hypertrophic osteoarthropathy (HOA) characterised by arthralgia, clubbing and periosteal proliferation of long bones, is rarely encountered in children and adolescents. Whereas in adults over 80% of cases are associated with malignancy, in children the majority of cases are due to non-neoplastic causes such as cystic fibrosis, bilary atresia and congenital heart disease. Up to 5% of adults with lung cancer demonstrate signs of HOA. However, lung cancer is extremely uncommon in children and young people. Here we report a case of lung adenocarcinoma in an 18 year old male associated with HOA present both at diagnosis and at subsequent disease progression.
Introduction
Hypertrophic osteoarthropathy (HOA) is a syndrome characterised by digital clubbing, polyarthritis and periosteal new bone formation of the long bones. 1 Lung cancer, a common cause of HOA in adults, is rarely encountered in children and adolescents. Whilst adenocarcinoma and squamous cell carcinoma are the most common histological subtypes seen in adults, bronchial carcinoid accounts for up to 80% of childhood lung cancers. 2 Here we report an unusual case of aggressive lung adenocarcinoma in an 18 year old male in which HOA was a disabling symptom.
Case Report
An 18 year old Caucasian male gave a six week history of progressive breathlessness and left sided chest pain. He had also noticed increasing pain and swelling of his finger joints. The patient reported no significant past medical history or family history and was not taking any regular medication. He had smoked up to five cigarettes a day for the previous two years and worked as a plumber, although there was no history of asbestos exposure. He attended his local emergency department and was diagnosed with pneumonia with an associated pleural effusion. Intravenous antibiotics were administered and a pleural tap was performed. Pleural fluid revealed a transudate with no malignant cells. Following drainage of the effusion his symptoms improved and he was discharged. He returned one week later with worsening dyspnoea, vomiting and widespread arthralgia, particularly affecting the upper limb. He was admitted for further investigations.
Serum haematology, renal, bone and liver profiles were normal. He had an elevated Creactive protein (150 mg/L, normal range <6 mg/L). Serum tumour markers including AFP, βHCG and CEA were within the normal range. An HIV test was negative. A chest x-ray demonstrated reaccumulation of the pleural fluid and a large pleural based mass involving the left hemi-thorax. CT scan confirmed a large left sided pleural mass with an associated pleural effusion and mediastinal shift. No other sites of disease were identified. Video-assisted thoracoscopic surgery (VATS) and a biopsy were performed. He was then transferred to our institution for further management.
On examination he had reduced air entry throughout the left lung with a chest drain in situ draining blood stained fluid. Marked swelling of the interphalangeal and metacarpophalangeal joints was noted. The patient demonstrated clubbing of the fingers. The remainder of the examination was unremarkable. Further staging investigations were then performed; a PET-CT (Figure 1) showed an extensive and irregular FDG avid mass within the left hemithorax extending from the apex towards the diaphragm, which appeared to be pleural based, extending towards the mediastinum and abutting the pericardium. A lytic lesion was also seen within the 10th thoracic vertebrae. A bone scan (Figure 2) did not reveal any discrete metastasis; however there was prominent uptake of tracer throughout the bone marrow with marked periosteal uptake of tracer, consistent with a diagnosis of hypertrophic osteoarthropathy (HOA). Review of the biopsy material demonstrated a poorly differentiated adenocarcinoma with numerous atypical mitosis. Immunohistochemistry revealed diffuse positivity for EMA, MNF116 and Ber-EP4. Staining was negative for TTF-1, calretinin, thrombomodulin, CK5/6, CD34, desmin, SMA, CD30, CD45, AFP and βHCG.
(A and B) Axial and coronal reconstructions of contrast-enhanced computed tomography (CT) scan of the chest demonstrating a heterogeneously enhancing mass extending from the left hilum (thin arrow) to the left chest wall (thick arrow). (C and D) Axial and coronal reconstructions of the fused PET-CT scan showing the left thoracic mass to be highly avid.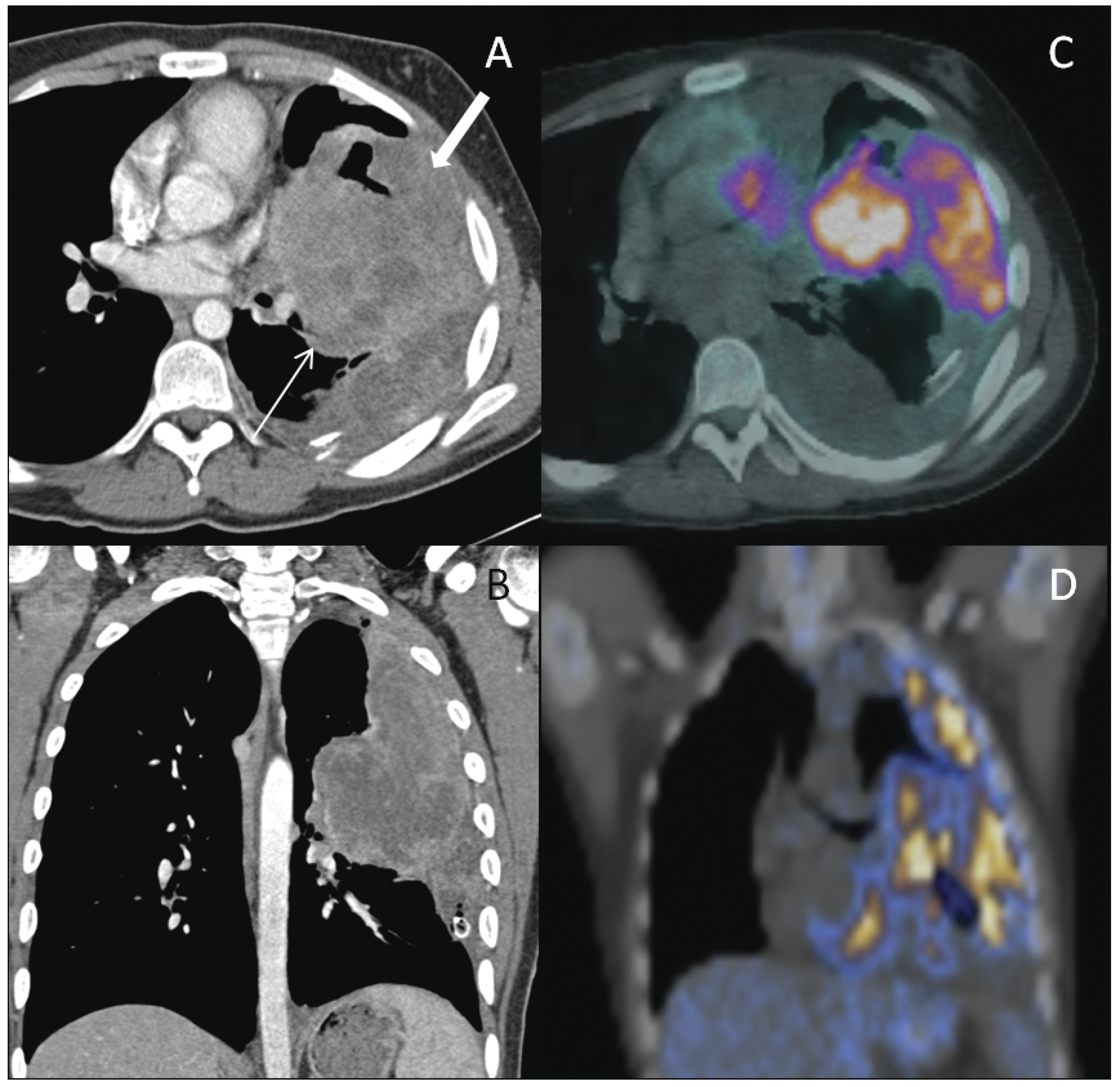
Bone scan coned in the view of the left arm demonstrating the increased periosteal uptake around the distal radius and ulna (thick arrows) and also in the humerus (thin arrow).
A diagnosis of poorly differentiated adenocarcinoma of the lung with associated HOA was made. The patient commenced treatment with cisplatin (80 mg/m2 day 1) and gemcitabine (1250 mg/m2 day 1 and 8) every 21 days. After one cycle of chemotherapy he noticed resolution of his joint aches and swelling and was able to discontinue all analgesics. A CT scan performed after three cycles of chemotherapy demonstrated a partial response. Unfortunately after the fourth cycle of chemotherapy the patient noticed a return of his joint pain and swelling and worsening left sided pleuritic chest pain. Imaging confirmed disease progression. The disease continued to progress despite sequential treatment with erlotonib, docetaxel, carboplatin/paclitaxel (introduced after an allergic reaction to docetaxel) and cisplatin/vinorelbine and he died from his disease 7 months after his original diagnosis.
Discussion
Primary lung carcinoma in childhood and adolescence is exceedingly rare and comprises only 0.2% of all childhood malignancies, 3 with an incidence of approximately one case per 2 million under 19 years old. 4 Metastases from non pulmonary tumours outnumber primary lung cancers in children and adolescents by 5 to 1. 5 Histological subtypes vary between adult and paediatric populations. Bronchial carcinoid tumours represent 50–80% of all pulmonary neoplasms diagnosed in children and adolescents2,4,6,7 and small cell and squamous cell lung cancers, common in adults are rare. 2 Historically, retrospective population based studies have demonstrated lower overall survival in younger patients with lung cancer although more recent data suggests that when stage is controlled for, overall and progression free survival is similar. 8 However, survival is markedly influenced by histology. In a large case series examining 160 patients less than 20 years old diagnosed with lung cancer, adenocarcinoma and squamous cell carcinomas were associated with the poorest survival with a median survival of 14 months, in contrast, those with endocrine neoplasms had a 92% 10 year survival. 4
An additional unusual feature of this case was the clinical and radiological features suggestive of HOA. HOA is well documented in adults but rarely encountered in children. The clinical features include clubbing of the fingers and toes, arthritis and a painful ossifying periostitis of the tubular bones. 1 HOA may be primary (hereditary or idiopathic) or secondary. Most cases encountered in children and young adults are secondary and associated with chronic suppurative lung processes (e.g. cystic fibrosis), congenital heart disease and biliary atresia. The association with malignancy is relatively common in adults and the prevalence of HOA in lung cancer has recently been reported in 4.5% of patients9,10 with over 80% of all secondary HOA in adults due to malignancy.11,12 Malignancy-associated HOA in children and young adults is not well documented but there are a number of case reports describing the association with carcinoma of the nasopharynx, osteosarcoma, rhabdomyosarcoma Hodgkin's lymphoma, thymic carcinoma and pleural mesothelioma.13,14 We did not identify any reported cases of HOA associated with lung carcinoma in children or young adults in the literature. The exact pathogenesis of HOA is not well understood. It has been suggested that processes which disrupt the pulmonary circulation prevent the normal fragmentation of platelets within the capillary bed. This allows the megakaryocytes or large platelet clumps to enter the systemic circulation where they can travel to the extremities and release platelet derived growth factor (PDGF) which leads to vascular proliferation, oedema and new bone formation. 15 Vascular endothelial growth factor (VEGF) is also thought to contribute to the development of HOA. It is over expressed in hypoxia and malignancy 16 and like PDGF can induce vascular hyperplasia, new bone formation and oedema. 17 The management and prognosis of HOA is dependent on the underlying disease process. In malignant HOA symptoms often resolve with the removal of the tumour or treatment with chemotherapy as in this case.14,18 Conventional analgesics, particularly non-steroidal anti-inflammatories are often used and intravenous bisphosphonates have been shown to improve symptoms. 19 A re-emergence of symptoms often heralds disease relapse and may precede symptoms from the primary tumour.14,20
Conclusions
Both primary lung cancer and HOA associated with malignancy are rare in children and young people and symptoms may often go unrecognised. Due to the small number of primary lung tumours in paediatric and adolescent patients, delays at diagnosis are common and patients often present with advanced stage disease as in this case.
Footnotes
Acknowledgement:
this work was undertaken at UCLH/UCL who received a proportion of funding from the Department of Health's NIHR Biomedical Research Centres funding scheme.