
Abstract
Hidradenoma papilliferum is a known example of adnexal skin tumours with apocrine differentiation. It is a rare benign tumour which tends to arise from areas with rich concentration of aporine glands such as anogenital region, vulval, perineal, axillae, and periumbilical areas. In this report, the tumour was found in the upper outer quadrant of left breast, being one of the ectopic sites for this tumour. Contrary to most reports where male preponderance was popular for ectopic hidradenoma papilliferum, the patient in this report is a 71-year-old female. Considering the location of this tumour in this report, the likely histopathological differential diagnoses such as tubular apocrine adenoma, clear cell (apocrine) adenoma, lipoma, intraductal papilloma and papillary carcinoma of the breast should be considered for exclusion. This is the first reported case of a giant ectopic hidradenoma papilliferum of the breast in a Niger Delta region of Nigeria which also highlights the role of fine needle aspiration and cytology in the diagnosis of breast lesions.
Introduction
A hidradenoma papilliferum is otherwise known as papillary hidradenoma or papillary adenoma when located in the breast.1,2 Commonly, it is a slow-growing benign adnexal tumour with apocrine differentiation and has microscopic description similar to those of intraductal papilloma of the breast.1,3 This benign tumour is composed of a sharply circumscribed nodule of ectopic breast tissue usually found on the labia majora or the interlabial folds. 1 Hidradenoma papilliferum tends to originate in the apocrine glands, which are mainly concentrated in the anogenital region, vulval, perineal, axillae, and periumbilical areas.4–8 However, the ectopic localization of this tumour is rarely reported with the most common site being the head and neck region.8,9
Case Report
Clinical history
A case of a postmenopausal Para 4 (3 alive), 71-year old female who first presented in September 2010 with a 5-year history of a slowly growing, painful, palpable mass on the left breast. The patient's associated symptoms included bloody nipple discharge and waist pain. There was no history of trauma, alcohol use and smoking. Family history of breast cancer was negative. She had breast fed all her kids for an average of 2 years each. No history of associated fever, coughing or night sweating. Physical examination revealed a giant lump in the upper outer quadrant of the left breast measuring 20.0×16.0 cm. It was largely nodular and cystic in some areas, non-tender, and freely mobile. The overlying skin showed obvious cutaneous veins. Also, bloody nipple discharge was observed. There was no axillary lymphadenopathy.
A preoperative diagnosis of fibroadenoma of the left breast to exclude phylloides tumour or breast cancer was made by the surgeon
Investigation findings were: Negative Human Immunodeficiency virus (HIV) serology, normal urinalysis and chest x-ray, fasting blood glucose was 3.7 mmol/L (2.7 –5.8 mmol/L) and packed cell volume (PCV) was 36% (35–45%). Serum electrolytes, urea and creatinine as well as white blood count with differentials showed unremarkable findings. However, fine needle aspirate and cytology as well as mammogram were not done. Three months after presentation, local wide excision (lumpectomy) was done.
The operatory findings revealed a mixed cystic and solid nodular mass measuring 16.0×8.0 cm, encapsulated, extending from the nipple towards the axilla and partly adherent to the underlying pectoral muscles.
The lump was sent for histopathologic study.
The patient was discharged 3 days after the surgery to be seen at the outpatient surgical clinic.
Pathologic findings
Macroscopic examination of the breast tissue showed a huge encapsulated lobular lump with multi-locular cystic cut surfaces containing light greenish to light brownish mucoid gelatinous materials. It measured 10.0×7.5×6.5 cm and weighed 600 g (Figure 1).
Macroscopic description showed multi-locular cystic cut surfaces containing light greenish to light brownish mucoid gelatinous materials.
Microscopic examination of breast tissue showed a well encapsulated tumour composed of arborizing papillary glandular pattern. These proliferating papillary fronds are lined by pseudostratified bland looking epithelial cells and possessed loose fibrous connective fibrovascular stromal cores infiltrated by few lymphocytes, macrophages and plasma cells. The non-neoplastic breast tissue underneath the tumor showed focal fibroadenomatous changes. (Figure 2, 3 and 4). However, the connection to the epidermis of the skin could not be ascertained.
Photomicrograph of breast showed complex arborizing papillary glandular structure (haematoxylin and eosin × 10).
Photomicrograph of breast showed complex arborizing papillary glandular structure (haematoxylin and eosin HE × 40).
Photomicrograph of breast showed the lumen of the papillary glandular structure lined by two layers of columnar and cuboidal cell with focal decapitation and fibrovascular core infiltrated by inflammatory cells (haematoxylin and eosin × 100).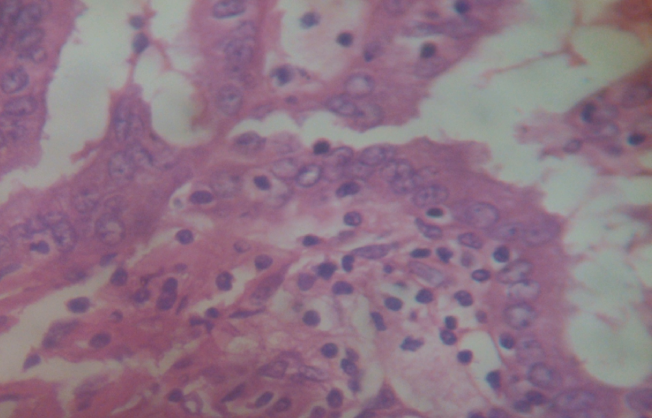
The histologic diagnosis was consistent with a giant hidradenoma papilliferum of the left breast.
Discussion
Hidradenoma papilliferum is a rare benign adnexal skin tumour in the African compare to Caucasians.4–7,10 This may be attributed to the presence of relatively increased amount of apocrine glands in the Caucasians.6–8 In addition, the tumour has its origin from the apocrine glands richly found in the anogenital region, vulval, perineal, axillae, and periumbilical areas.4–8
Left breast was found to be the anatomical site for ectopic hidradenoma papilliferum in this series. Previously reported common sites for ectopic hidradenoma papilliferum include the head and neck region, extremities, upper eyelid, external ear, nose, and chest wall.9–15 Of all these sites, head and neck region is the most favoured site for ectopic hidradenoma papilliferum.8,9 The histogenesis of this tumour in ectopic sites could be linked to the corresponding areas rich in heterotrophic and modified apocrine glands. 8
The age range for those patients with ectopic hidradenoma papilliferum varies. Our patient was an 71-years old which lies within the age range of 8 to 78 years recorded by Fernández-Aceñero
Although, our patient is an old woman, most studies report a male preponderance for the ectopic lesion.8,10,11,14,15 However, independently of being typical or ectopic, the tumour occurs mostly in white women, but in contrast to the anogenital lesions, in which nearly one-half of the patients with the ectopic form are men. 8 In contrast to most studies, Loane et al in Cork, Ireland recorded one case of perianal hidradenoma papilliferum in a man. 7
The patient in our study presented with 5-years history of slowly growing, painful, palpable left breast mass and bloody nipple discharge. This findings are not too different from a study conducted by Fernández-Aceñero et al in Madrid, Spain who reported similar patterns of clinical presentation for both anogenital and non-anogenital (ectopic) hidradenoma papilliferum.9,10 Neither pruritus nor ulceration was present in our study, which is in contrast to other studies.5,10
Focal inflammatory infiltrates rich in plasma cells, lymphocytes and occasional macrophages seen in our study, were similarly reported by studies conducted by Fernández-Aceñero
Depending on the location of these tumours, the likely histopathological differential diagnoses to be considered include tubular apocrine adenoma, clear cell (apocrine) adenoma, lipoma and intraductal papilloma and intraductal carcinoma of the breast with papillary pattern.1,3,10 The treatment of choice in our study was local excision which conforms to the most literature.1,4–15 Although a few studies have reported recurrence following incomplete excision of the primary tumour. 10 Recurrence of this lesion could not be ascertained in our study, as more time is needed for this.
Some authors have described malignant transformation in anogenital hidradenoma papilliferum such as intraductal carcinoma resembling apocrine carcinoma and invasive adenosquamous carcinoma but this is usually not seen in the ectopic presentation.8,17–19 They claimed that HPV plays a crucial role in inducing malignancy, but the association still needs to be verified. 19 Fine needle aspiration and cytology (FNAC) is an important diagnostic tool of breast lesions which is well accepted and established method to determine the nature of breast lump with high degree of accuracy.20–23 Its advantages include simple, cost effective and less traumatic as well as highly sensitive and specific method for assessment of breast lumps. 20 Tiwari in Nepal, Indian reported sensitivity and specificity of breast FNAC in diagnosis of malignancy to be 83% and 100% respectively. 20 Thus, fine needle aspiration and cytology (FNAC) is advised prior to biopsy in palpable breast lumps with provisional diagnosis of either benign or malignant lesions.
Conclusions
Overall, ectopic hidradenoma papilliferum including those located in the breast is rare and this report in a woman contrasts findings in most studies.
Footnotes
Acknowledgments:
The authors appreciate the support received from the management and staff of University of Uyo Teaching Hospital, Uyo, Akwa-Ibom State, Nigeria, in ensuring the success of this manuscript.