
Abstract
Mixed acinar-endocrine carcinomas (MAEC) are rare tumors of the pancreas. We present the case of a patient with periampullary tumor that presented with painless jaundice and after investigation was found to have MAEC. He underwent pancreaticoduo-dunectomy with tumor free margins and negative lymph nodes. The patient presented with local recurrence and liver metastasis after 1 year and is on chemotherapy with stable lesions 30 months after the diagnosis.
Introduction
Pancreatic tumors are rare and constitute less than 1% of all neoplasms. Adenocarcinomas represent more than 75% of pancreatic cancer, neuroendocrine carcinomas are 7% and acinar cell carcinomas (ACC) are 1%. 1 Mixed endocrine-exocrine tumors of the pancreas are also very rare. The World Health Organization (WHO) classified these tumors as either mixed ductal-endocrine carcinomas that are part of the ductal carcinomas, and should have more than 30 % endocrine component, or mixed acinar-endocrine carcinomas (MAEC) that are part of the ACC and should have at least 30% endocrine component. 2 Another classification for mixed tumors from the Atlas of Tumor pathology (fourth series) dictates that each component has to compose at least 25% of the total cells. 3 We present a case of a 52 years old male patient who presented with MAEC with a review of the literature.
Case Report
A 52 year-old male patient presented to our institution with epigastric pain, fatigue and jaundice. Computed tomography (CT) scan revealed a dilated commom bile duct (CBD). Endoscopic retrograde cholangiopancreatography revealed a mass in the vicinity of the ampulla of Vater obstructing the lumen. Fine needle aspiration (FNA) revealed a neuroendocrine tumor. Past medical history was positive for atrial fibrillation and the patient was a 45 pack-year smoker.
His laboratory studies were as follow: total bilirubin 8.8 mg/dL (normal range 0–1.2), 7 mg/dL direct bilirubin (normal range 0–0.3), SGOT 56 IU/L (normal range 0–50), SGPT 75 IU/L (normal range 0–65), γ-GT 220 IU/L (normal range 10–50), lipase level 119 U/L (normal range 13–60) and alkaline phosphatase 332 IU/L (normal range 35–120).
A standard pancreaticoduodunectomy was performed and pathology revealed an ampullary tumor measuring 1.5×1.2×1 cm compressing but not obstructing the opening. Microscopic examination of the mass showed that the tumor was composed of two cell types: 75% of cells with endocrine differentiation (islet cells) and the other 25% with exocrine features (acinar). The endocrine component had relatively well differentiated areas as well as moderately differentiated areas with brisk mitotic activity (up to 5 per single HPF). The exocrine component consisted of well differentiated cells arranged in acini (Figure 1). The tumor originated in the ampulla and eroded the duodenal mucosa but didn't infiltrate the ampullary lumen. The surgical margins were free of tumor. Immunohistochemistry was diffusely positive for chromogranin and the acinar portion was focally positive. All lymph nodes were negative for metastasis.
Histological sections of the resected mass. (1) Low magnification showing tumor extending into duodenal mucosa. (H&E, 20×). (2) Higher magnification showing the acinar exocrine component of the tumor (left) and endocrine component (right). (H&E, 100×). (3) The exocrine component consists of well differentiated cells arranged in acini. (H&E, 400×). (4) Portion of the endocrine component showing nests of tumor cells with chromogranin A positivity (400×).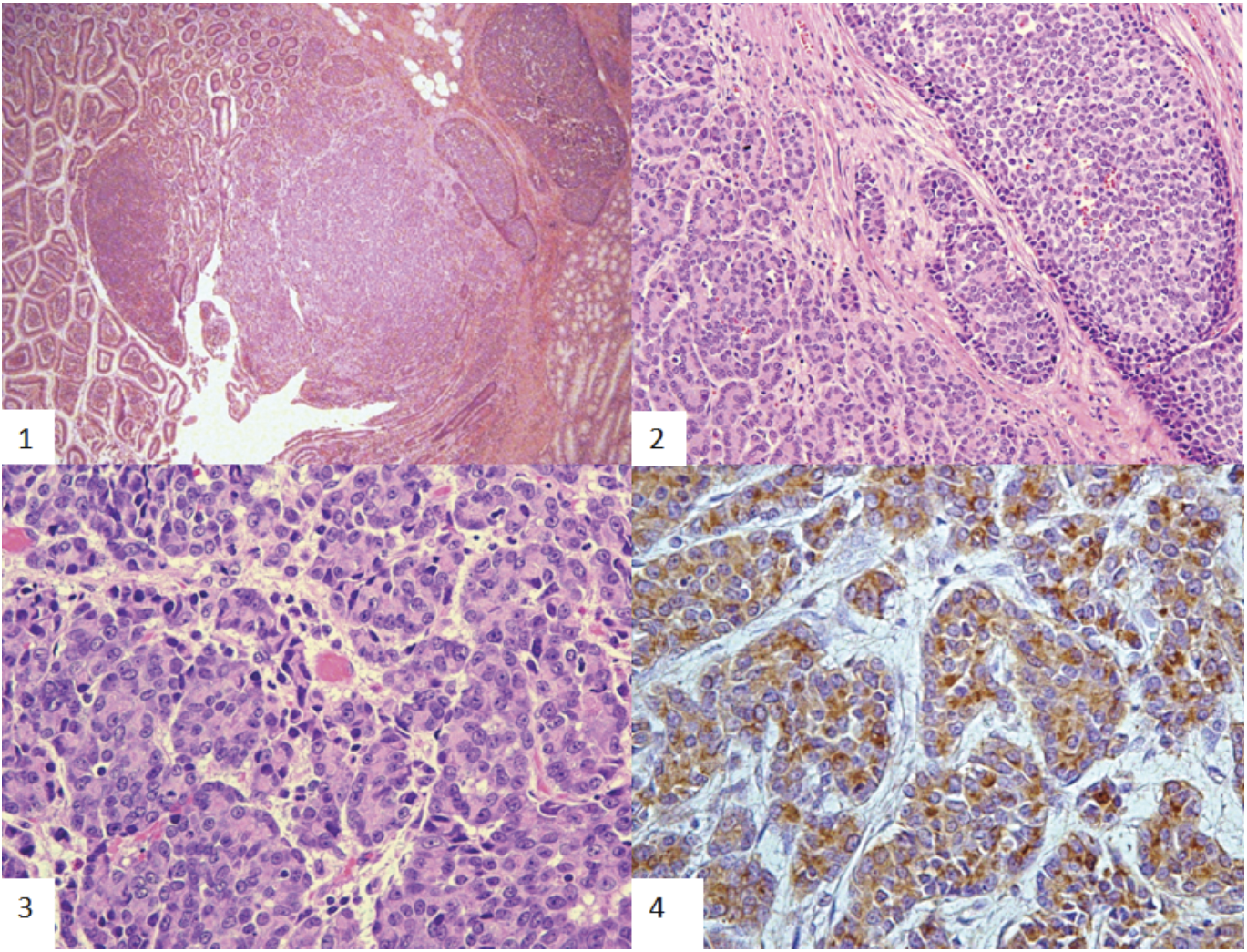
Follow up CT scans at 4 months post surgery did not show evidence of tumor recurrence.
One year after, he presented to the emergency room with severe epigastric pain radiating to the back. CT scan showed local recurrence in addition to liver metastasis and paraaortic soft tissue mass. FNA of both masses confirmed a high grade tumor similar to the original tumor resected. The masses were positive for chromagranin and synoptphysin.
The patient was started on cisplatin (50 mg/m2) and Camtothecin (180 mg/m2). This treatment was planned to be given every two weeks. Before the forth cycle, serotonin level and chromagranin A level were 392 ng/mL (normal 151–186) and 2380 (normal <100) respectively. CT scan performed after chemotherapy and showed a reduction in the liver lesions. Another 4 cycles were given and a repeat CT scan revealed a decrease in the size of the liver lesions. The new serotonin level was 205 and the chromagranin A level was 391. After the 7th cycle, CT scan showed a mild increase in the liver nodules. A different chemotherapy protocol was initiated and consisted of 2 cycles of 1250 mg/m2 of Gemcitabine followed after 1 hour by 50 mg/m2 of cisplatin. The patient is now on same protocol but oxalipatin (100 mg/m2) instead of cisplatin because of adverse drug reaction.
Recent CT scan of abdomen and pelvis showed progressive hepatic disease with stable extrahepatic pancreatic – bed lesion. PET CT scan with Gallium (68) didn't reveal any activity in both hepatic and extrahepatic lesions (Figure 2).
Computed tomography scan of the abdomen showing the recurrent lesions. (1) The liver lesions that were detected on computed tomography scan. (2) The recurrent mass in the left paraaortic region. (3) Latest image of the liver lesions that show regression in size after the treatment in comparison to 1st image. (4) Regression of the mass in the primary site of the neoplasm.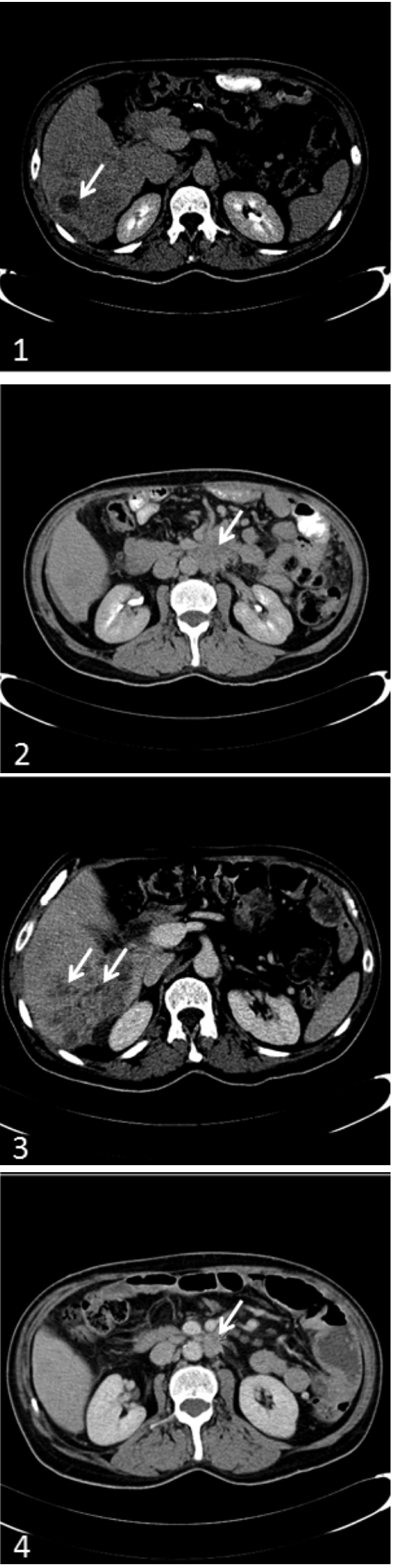
Discussion
Pancreatic tumors can originate from acinar, ductal or endocrine cell types. 1 However it has been reported that pancreatic neoplasms can exhibit more than one line of cellular differentiation. 2 Mixed exocrine-endocrine neoplasms of the pancreas are rare tumors, characterized by the association of an exocrine-ductal or acinar component and a significant endocrine component that comprise at least one-third to one-half of the total tumor tissue (Tables 1 and 2).1,4
Immunohistochemistry staining in reported cases of mixed acinar-endocrine carcinomas of the pancreas.

CGA, chromogranin A; CEA, Carcinoembryonic antigen; NSE, neuron-specific enolase; MUC1, Mucin 1, cell surface associated.
Reported cases of mixed acinar-endocrine carcinomas of the pancreas in the literature.

PPPD, pylorus preserving pancreaticoduodunectomy, NA, not available
Cubilla et al reported in his large series the incidence of MAEC to be 0.2%. 5 MAEC can present in 3 different combinations: a tumor with separate acinar and endocrine regions identifiable by light microscopy (Collision tumor), a mixture of endocrine and acinar cells (intermingled tumor) and a tumor with uniform cell population by light microscopy but with amphicirne features immunohistochemically.1,6 The histogenesis of MAEC is still controversial; the co-existence of exocrine and endocrine elements in these tumors can be attributed to their common embryologic origin (Tables 1 and 2).7,8 Although the biologic aggressiveness of MAEC is still uncertain because of the small number of cases, Klimstra et al. suggested that the behavior of MAEC may be similar to that of acinar cell carcinoma. 6
It is not known whether mixed acinar-endocrine carcinomas are simply an acinar cell carcinoma with an increased number of endocrine cells or is developmentally distinct from acinar cell carcinoma. Koboayashi et al. reviewed 21 cases of mixed exocrine-endocrine carcinoma (Table 1 and 2). 9 The tumor can develop in any part of the pancreas, but they were relatively common in pancreatic head. Metastasis was observed in 6 cases with a mean survival time of 20.6 months. He concluded that MEAC have a similar behavior of malignancy to that of acinar cell carcinoma. Our patient relapsed 18 months after the surgery and the main site of relapse was locoregional with liver metastasis. He responded partially to chemotherapy and he is still alive 30 months after diagnosis. To the best of our knowledge, no specific chemotherapeutic agents targeting MEAC were discussed in literature. The chemotherapy regimen given to our patient was based on the AUB tumor board decision, which was in turn extrapolated from the treatment of Acinar cell carcinoma and endocrine carcinoma of the pancreas since they share similar components.
Hange A et al., reported recently 96% sensitivity for (68) Ga-DOTA-TATE PET compared to 56% for (18) F-DOPA PET for detection of metastasis in neuroendocrine tumor, but no data were reported in mixed acinar-endocrine tumor. 10 Our patient did not show any activity either in the liver or at the site of locoregional disease recurrence with (68) Gallium DOTTA-TATE PET CT scan which may reflect the absence of somatostatin receptors in such tumors. Since our case has no secretory activity with negative (68) Ga PET CT Scan, 18F-DOPA PET CT Scan will not be of help.
In conclusion, MEAC is a very rare condition with relatively poor prognosis. Due to the small number of cases reported, there are still many controversies regarding the treatment of choice for those tumors. Therefore, surgery should continue to be the gold standard of their treatment, since it has been the one to demonstrate satisfactory long-term survival results (Table 1 and 2). 11