
Abstract
Merkel's cell carcinoma is a rare cutaneous tumor that can affect a wide variety of sites throughout the body. Commonly, it affects the skin alone and the management of limited disease can be confusing since the natural history of the disease involves distant metastasis. Traditional management has required wide local excision with negative margins of resection. We describe a case treated with local therapy alone and review the literature to suggest that complete microscopic excision may not be required if adjuvant radiotherapy is used.
Keywords
Case Report
A 74 year old Caucasian male presented with a change in a skin lesion of the dorsal aspect of the left forearm. A small non-descript lesion of approximately 1.0 cm had been present for at least 10 years which began to grow significantly over a six month period developing an erythematous and more nodular appearance. The patient was then referred for a surgical opinion and excisional biopsy. The original gross pathology described a firm, tan-appearing lesion measuring approximately 1.0 cm in greatest dimension. The original interpretation at an outside institution was that of metastatic anaplastic carcinoma. The pathologic slides and blocks were sent to the Allegheny General Hospital and reviewed. The tumor exhibited prominent peri-nuclear staining for cytokeratin 20, strongly positive for cytokeratin CAM 5.2, focally positive for neuron specific enolase, synaptophysin and MAP 2. The tumor cells were negative for chromogranin, leukocyte common antigen, and cytokeratin 7. The margins of resection were microscopically positive in multiple areas (R1 resection). The final diagnosis was neuroendocrine (Merkel cell) carcinoma. At follow-up clinical examination, no evidence of gross disease in the local site was identified. The incision measured 4.0 cm and was healing well. There was a moderate amount of induration in the peri-incisional area and minimal erythema in the post-operative bed. The patient was reluctant to undergo additional surgical excision due to the likelihood of tissue graft or flap requirement and the resultant possibilities of cosmetic and functional deficit in order to cover the projected large skin defect. The remainder of the physical exam was benign.
A metastatic workup consisting of a bone scan, CT scan of the chest and a PET scan revealed no evidence of metastatic disease. A brain MRI was normal. An abdominal CT scan demonstrated evidence of a right-sided renal mass which was suggestive of an angiomyolipoma. An ultrasound of the kidneys confirmed this finding. After further questioning, the patient admitted to a CT of the abdomen done 7 years prior. We retrieved this scan and found that the lesion was unchanged. Comprehensive metabolic analysis (CMP) and hemogram were unremarkable. His past history revealed hypertension, gastro-esophageal reflux, and benign prostatic hyperplasia. His medications included tamsulosin 0.4 mg, aspirin 81 mg, and esomeprazole 20 mg daily. His family history was unremarkable as was his review of systems, although he did admit to a 50 pack year smoking history which ceased 10 years prior to diagnosis.
The patient's case was discussed in a multi-disciplinary tumor board and the final decision was made for local irradiation only in view of the small, single focus of disease and complete gross excision. The local therapy consisted of shrinking field radiotherapy begun 4 weeks post-operatively. The tumor bed received 4600 cGy at 200 cGy per fraction including a 2.5 cm margin followed by a boost delivering an additional 1400 cGy at 200 cGy per fraction to the same site with a 1.5 cm margin. All treatment was delivered with a 6 MV linear accelerator using three-dimensional conformal techniques with a 1.0 tissue equivalent bolus overlying the incision to deliver full dose to the skin at this site. Acute treatment related sequelae included only grade II erythema of the skin (CTCAE v 4.0) 1 which resolved two weeks following the completion of radiotherapy. Follow up consisted of interim clinical history and complete physical examination and repeat bone scan, CT scan of the brain, thorax, and abdomen as well as a hemogram and CMP on an every three month basis for two years. PET scanning was repeated after the first follow-up visit and then at 3 month intervals for the same period of time. The patient is now 7 years post therapy and has had no evidence of recurrence. His only treatment related sequelae is slightly increased fibrosis in the tumor bed and permanent alopecia of the local site.
Discussion
Natural history
Merkel cell carcinoma (MCC) is a rare and often lethal cutaneous malignancy which was first described in 1972. 2 It is thought to be derived from Merkel cells of the skin, but it has also been proposed that the cell of origin may be a primitive pluripotent epidermal cell. 3 The University of Pittsburgh has shown that Merkel cell carcinomas frequently harbor a polyomavirus which has been aptly named Merkel cell polyomavirus. 4 The exact oncogenic role of the virus remains to be clearly elucidated.
The incidence in the United States is 0.23 per 100,000 in Caucasians, occurring most commonly in the elderly, with a three-fold increased incidence since 1986. 5 MCC is much less prevalent in the black population, 6 and is significantly higher in immuno-suppressed populations. The relative risks when compared to the general population for patients with HIV or those who have received organ transplantation are 13.4 and 5, respectively.7,8
MCC typically presents as a firm, pinkish-red nodular or plaque-like exophytic mass. The most common locations are in sun-exposed skin of the head, neck or extremities. 9 Wide local excision is the mainstay of treatment, 10 although radiotherapy has often been used as adjuvant or definitive treatment.11–15 As with melanoma, depth of invasion is a prognostic feature. 16 A recent meta-analysis also showed the prognostic importance of sentinel lymph node biopsy (SLNB). In 122 patients, MCC recurred within 3 years in 60% of patients with a positive SLNB versus 20% having negative nodes. 17 MCC is locally aggressive, demonstrating local recurrence rates between 25 and 100% following surgical excision and the mortality rate of MCC is between 30 and 60%. 9 In a series of 251 patients from one institution, patients with stage IV disease had a median survival time of 6.8 months. 18
Pathologic features
MCC appears as a dense population of small, round blue cells on hematoxylan and eosin stain. The nuclei are large relative to the cytoplasm and they may have finely granular and evenly distributed chromatin (salt and pepper like) (Figure A). Mitotic figures and apoptotic cells are common. 18 The cells form dermal nests, trabeculae or sheets. Mitotic activity is usually brisk and single cell necrosis is frequent (Figure B). Immunohistochemistry (IHC) is helpful to distinguish it from other small cell types of malignancy such as small cell lung carcinoma, lymphoma and melanoma. Neuron-specific enolase, chromogranin, synaptophysin and cytokeratin are frequently positive in MCC. S-100 and thyroid transcription factor-1 are negative in MCC, which help distinguish it from small cell-lung carcinoma. Cytokeratin 20 is a fairly specific and sensitive marker for MCC, with a characteristic paranuclear dot-like positivity (Figure C).
(A) A predominately dermal small blue cell tumor, with slate gray low power appearance. (hematoxylineosin, original magnification ×100). (B) The cells form dermal nests, trabeculae or sheets composed of uniform oval cells with uniform nuclei with pale vesicular of finely granular (salt and pepper-like) nuclei and scant amphophilic cytoplasm Mitotic activity is usually brisk and single cell necrosis is frequent. (hematoxylin-eosin, original magnification ×400). (C) The small round cells show membranous and paranuclear dotlike staining with cytokeratin 20 immunoperoxidase staining, original magnification × 200).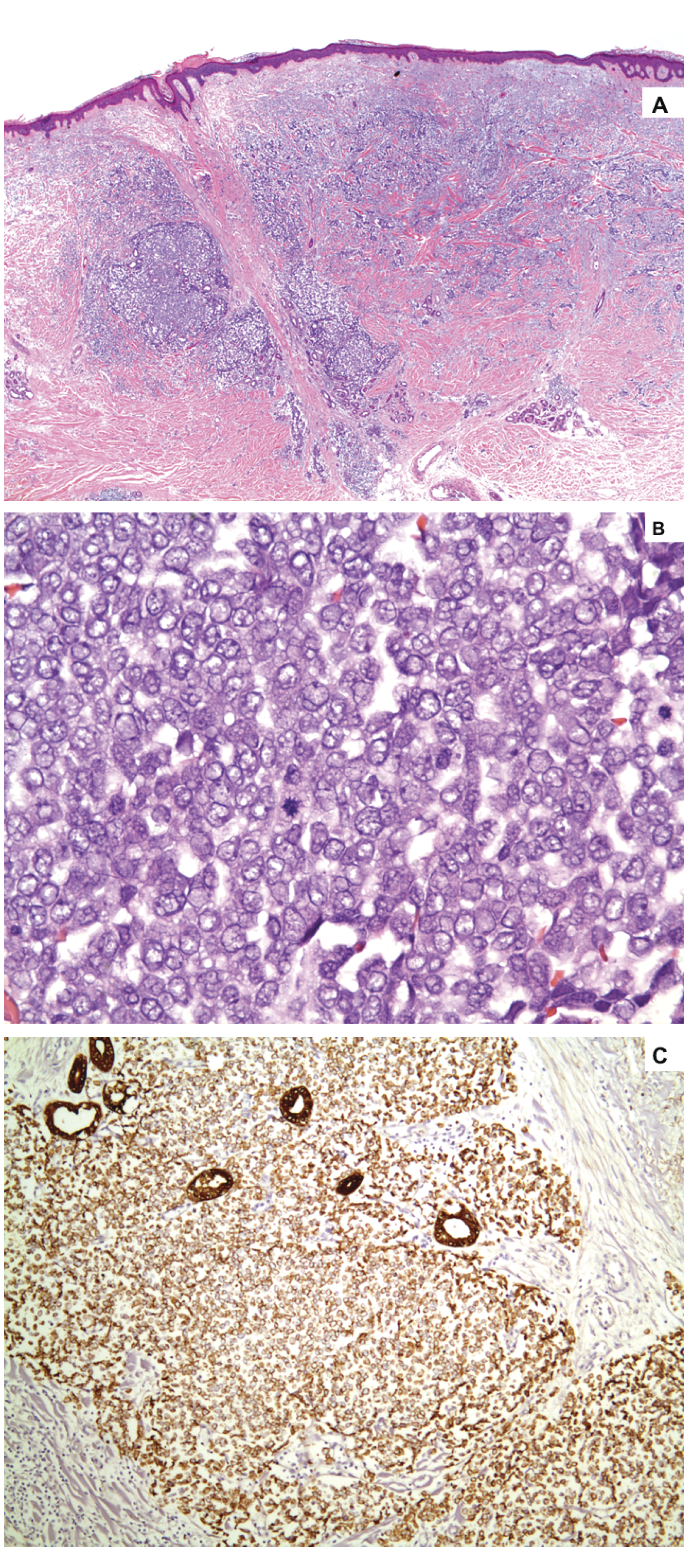
Traditional management
Traditional management has been surgical resection as the mainstay of local therapy. However; standardized adjuvant therapy is less well defined. In the largest reported study to date, the Trans-Tasman Radiation Oncology Group reported their phase II findings in 2003.(19) The standardized treatment consisted of Carboplatinum (day 1) and Etoposide (days 1–3) with concurrent radiotherapy (5000 cGy at 200 cGy/fx with wide margins) followed by two additional cycles of chemotherapy. Of the 53 patients enrolled in the study 76% were alive at 3 years and 65% had no evidence of relapse. Unfortunately grade III neutropenia occurred in 57% of patients and 23% of patients developed grade III skin toxicity. The NCCN has incorporated this treatment strategy as one recommended option for therapy. 20 In general, the recommendations call for wide surgical excision. 10 One group reported on the use of Moh's micrographic surgery in highly selected small MCC without adjuvant therapy and reported a 96% local control rate and 5 year overall survival rates approaching 80%. 21 Three patients had in-transit metastases while only one patient developed a marginal recurrence which was successfully salvaged with re-excision and local irradiation.
Radiotherapy as monotherapy
Radiotherapy has become a mainstay of local treatment with most reported series demonstrating significant increases in local control with the addition of radiotherapy following surgical resection.22–27 Although a single study showed no improvement in local control, a small sample size has limited the conclusion. 18
Conflicting data have been reported regarding the use of primary radiotherapy absent surgical resection. In a series by Meeuwissen et al., 28 7 of 80 total patients were treated by radiotherapy after incomplete gross surgical resection (R2 disease). Six of these patients recurred with primary radiotherapy alone using doses of 4500–6000 cGy. However; Mortier et al. 29 have reported on a series of 9 patients treated with primary radiotherapy (median dose 6000 cGy; range 5000– 7800 cGy) with no local recurrences despite primary tumor sizes ranging from 1.0–8.0 cm.
Waiting time has been implicated in progression of disease. Tsang et al have reported a near doubling of local recurrences (25 vs. 40%) when mean waiting times between surgery and radiotherapy increased from a mean of 19 vs. 30 days respectively. 30
Novel therapies
The use of imiquimod (an immune modulator that activates TLR7 cells on the skin surface) cream plus radiotherapy (5040 cGy in 28 fractions) has been used anecdotally 31 as has hyperthermia with radiotherapy 32 with limited success. Both groups demonstrated local control, however adjuvant radiotherapy was delivered in both cases and the margins of resection were histologically negative.
Conclusions
Conventional local treatment of MCC has traditionally involved wide local excision with a goal to achieve negative surgical margins followed by radiation therapy. Depending upon location, such surgical management can result in significant disfigurement requiring reconstructive flap or graft surgeries. Additionally, the increased time interval between repeat surgical and adjuvant management may worsen outcomes. The data we have presented here demonstrate options for management that may not require such extensive surgical approaches or microscopically negative margins and still result in satisfactory outcomes. The case we have presented is an example where radiotherapy following surgery for a small tumor resulted in local disease control with acceptable morbidity despite microscopic marginal positivity. We urge consideration of such alternatives in cases where patients do not desire additional potential disfiguring surgery.