
Abstract
A 75-year old man was detected with a pediculate tumor in the upper esophagus. A biopsy determined that it was an adenocarcinoma. A subtotal esophagectomy with dissection of three-fields of lymph nodes was selected. The pathological study revealed it to be an esophageal adenocarcinoma arising from ectopic gastric mucosa of the fundus of the stomach. His post-operative course was uneventful and without sign of recurrence for 3.5 years.
Introduction
Esophageal adenocarcinomas arising from ectopic gastric mucosa (EAEGM) have been reported in only 26 cases worldwide, therefore therapy for this condition is still inconsistent. The available therapeutic strategies for surgical treatment, chemotherapy and/or radiation will be discussed from experience with the present case, and in reference to past reported cases. This is the first report to discuss the clinical features and treatment for EAEGM.
Case Report
A 75-year old man underwent a medical examination without any complications. Since an upper gastrointestinal X-ray showed a simple shaped tumor, 20 mm in size (Figure 1a), detailed studies were selected. On laboratory blood examination, no abnormal data were found except for slight anemia and a high value of squamous cell carcinoma-related antigen, 1.3 ng/mL (normal range; <1.5 ng/mL). An upper gastrointestinal endoscopy detected a pediculate tumor, 25 mm in size, with easy bleeding in the upper thoracic esophagus (invasive level; muscularis propria) (cT2) (Figure 1b), and pathological findings from a biopsied specimen revealed a moderately differentiated tubular adenocarcinoma. With chest and abdominal computed tomography (CT), a primary pediculate tumor, 30×20 mm in size, with regional lymphnode swelling (N1) was noted without any metastasis or direct invasion to other organs (M0). According to the UICC 6th edition staging system, the tumor was indicated as cStage IIB, and a subtotal esophagectomy with lymph-node clearing was performed in April, 2006. On removal, a type I tumor, 35×22 mm in size, was observed on the esophagus, and it stained negative with lugol solution (Figure 2). In addition, the esophageal mucosa surrounding the tumor was also negative for lugol solution, suggesting that the tumor arose from the ectopic mucosa. The pathological study demonstrated the presence of a tubular papillary and solid type EAEGM (pStage: I, invasion level: mucosa, lymphatic duct invasion: not detected, vessel invasion: not detected) (Figure 3), and lymph node metastasis was not noted. The patient is currently in good health without any problems.
Upper gastrointestinal X-ray and endoscopic examination. Barium esophagogram (a) (arrow) and upper gastrointestinal endoscopy (b) showed a pediculate tumor, 20 mm in size, which was detected in the upper thoracic esophagus.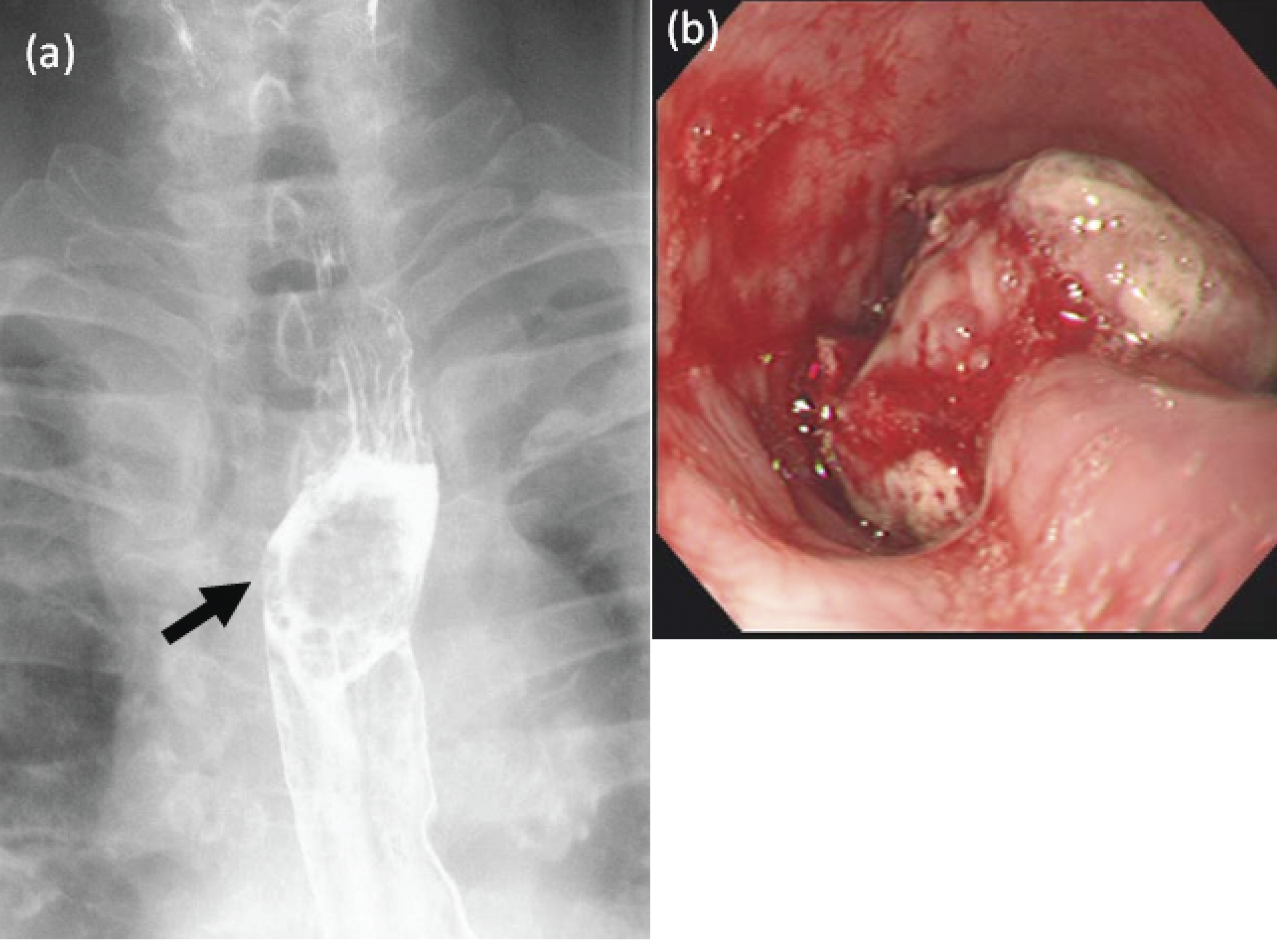
Removed specimen of subtotal esophagectomy. The type I tumor, 35 × 22 mm in size, was detected in the specimen (arrow head). The tumor was round shaped and was negative for lugol solution staining, with the negative staining extending 5 cm distant from the oral margin (arrows).
Pathological findings. Tubular, papillary and solid adenocarcinoma were localized within the tumor (a and b). In the epithelium around the tumor, mucosa similar to fundic gland mucosa extended from the tumor (a and c). H & E stain, (a) ×40, (b and c) ×100 magnification.
Discussion
Primary esophageal adenocarcinomas that match the following diagnostic criteria represent 0.76% of all the cases of carcinoma of the esophagus or cardia; i) a tumor localized in the esophagus from the cricoid cartilage to the cardiac orifice; ii) a tumor arising from the esophageal glands; iii) a tumor that has tissues of the glands, and where there are lesions of the carcinoma discharging mucus on the inside of the tumor; iv) existence of normal squamous epithelium in the anal side of the tumor, or a tumor that exists in an area apart from the cardiac orifice; v) no primary cancerous lesions in the other organs.1,2 Because the incidence of ectopic gastric mucosa has been detected in only 4.0% of males and 2.9% of females, 3 carcinogenesis at this site is observed quite rarely, with 26 cases reported worldwide as shown in Table 1.4–25 The age of these patients ranged from 37 to 85 years, and the tumor size was between 1.9 and 7.0 cm (mean; 3.9 cm). The nature of invasion into surrounding tissues was found to be to the submucosal level in 9 cases, muscular invasion in 4 cases and advanced invasion in 9 cases, with 3 cases unknown. If the degree of layer invasion and tumor size are compared, the average tumor size was 3.4 cm in submucosal invasion, 4.3 cm in advanced invasion and 4.5 cm in muscular invasion, suggesting that the tumor size (width of growth) might be associated with the degree of layer invasion (invasive level of tumor). However, the prognosis was not exactly indicated by tumor size, because in patients with big tumors, such as 5 cm or 6.5 cm, there may be no signs of recurrence, whereas tumors as small as 2 or 3 cm could lead to recurrence. Focusing on the nature of the layer invasion to estimate the most favorable therapeutic strategy in submucosal invasion cases, esophagectomy was an appropriate radical treatment, but not partial resection, because local resection alone was found to lead to local recurrence. In muscular invasion cases, one of 2 cases of esophagectomy without additional therapy led to recurrence, and a case treated with radiotherapy (RT) and chemoradiotherapy (CRT) showed a relatively good prognosis. In advanced cases, with the exception of one unknown case without detailed data, esophagectomy without additional therapy led to a poor prognosis for 3 cases in 4, and one case remains alive but is still under short-term observation. In contrast, one esophagectomy case combined with RT showed a good outcome. In addition, esophagectomy combined with radiation or chemo-radiation therapy might result in a favorable outcome, suggesting that additional treatment beyond the initial operation is critical. In the present case, since there was no tumor invasion into the muscular layer, no adjuvant treatment was required and no signs of recurrence have been observed.
Twenty-six cases of esophageal adenocarcinoma arising from the ectopic gastric mucosa.

Adenoca, adenocarcinoma; rec, recurrence; meta, metastasis.
The rate of lymph node metastases was found to be relatively high in the esophagus, with around 30% of cases showing submucosal invasion, compared to 19% in the stomach. 26 Additionally, distant metastasis has been noted frequently due to the anatomical characteristic of the esophagus developing a strong lymphatic network, 27 indicating the importance of aggressive lymph node resection. In fact, complete surgical resection represents a first-line treatment for esophageal adenocarcinomas, such as Barrett's esophageal adenocarcinoma. 28 In addition, in East Asia, the combined drug TS-1 (tegafur/gimeracil/oteracil potassium), an oral 5-FU drug, is widely accepted as a chemotherapeutic agent due to its high response rate; 47% in single use and over 70% when used in combination with other chemotherapeutic agents.29,30 In contrast, because TS-1 is not commonly used in North America and Europe, a combination chemotherapy based on infused 5-FU is widely selected as a standard; infused 5-FU and cisplatin or the addition of a third drug (anthracyclines; epirubicin).31,32 The response rate has been reported as 49–56% against locally advanced gastric cancer.33,34 In conclusion, radical surgical treatment with adjuvant chemotherapy should be considered for advanced EAEGM.