
Abstract
In February 2020, Italy has been the first country in Europe fighting against COVID-19. In March 2020, Italian government declared national lockdown. Until May 4th, people stayed in home confinement and only the so-called essential works and activities were continued. Like in other countries, both for the disease severity and for the risk of death, the higher the age of people the higher the risk. In the first months of 2020, Italy saw a very high number of deaths related to COVID-19, with a huge age effect. There is an agreement on the view that there had been also an excess of mortality and on the role of mortality as a correct way to reflect the dynamics of the virus's spread. In this paper we briefly discuss the trends of mortality during the first 4 months of 2020 according to the data by the Italian National Institute of Statistics.
Introduction
Since the last days of 2019, China has fight with a new coronavirus called SARS-CoV-2 and the related disease called COVID-19. Starting from China, in first months of 2020 the outbreak took Europe and then USA and other countries of the world and now it is spreading all over the world. As of March 11, 2020, World Health Organization declared pandemic status. Today, after more than 13 months, the pandemic is still going on, with more than 150 millions of infected people and 3 millions of deaths all over the World.
Significance for public health
Data on mortality and on excess of mortality during pandemic are critical to be investigated as there is an agreement on their role in the understanding of the dynamic of pandemic. The paper shows differences in Italy: while some regions showed an excess of mortality, other regions did not show differences. The paper discusses possible reasons for the excess of mortality (high pressure on Italian public health system during the acute phase of pandemic could have had the indirect effect of increase other causes of death, like the ones related to other disorders or diseases for which individuals had difficulty to access to care during the more critical phases of pandemic. From an intervention perspective, it proposes some practical suggestions for planning and implementing specific interventions during current and future steps of the COVID-19 Pandemic, aiming to prevent excess of deaths.
Italy is one the oldest country in Europe and in the World and it has been the first country in Europe that start fighting against COVID-19.1,2 Like in other countries, the higher the age of people the higher the risk of contagion, the risk of severity of the disease and the risk of death.3-11 The month of March represented the first step of the Italian's experience with the outbreak, with a progressive diffusion of the contagion and with government progressive introduction of the mitigation measures. As of March 2020, Italian government declared national lockdown. Until May 4th, 2020, people stayed in home confinement, schools were closed, face to face lesson were stopped and only the so-called essential works and activities were continued. Despite the introduction of measures to mitigate the infection and spread of the virus, Italy was particularly affected in this first phase, both for the number of people who contracted the virus and for the number of deaths.
In this paper we aim to describe some effects of the pandemic and the spread of contagion, with a focus on COVID-19-related deaths. There is an agreement on the role of mortality as a correct way to reflect the dynamics of the virus's spread. 2 Moreover, according to Bartoszek and colleagues, 2 there is a need to put attention not only on a country level, but also on a region-level because the country-level does not say much about the dynamic of the disease and of the contagion that could have taken place at regional level. We choose to focus our attention on the first four months of 2020 that represent the so-called first wave of pandemic in Italy. In these months, Italy saw a very high number of deaths related to the COVID-19 infection and there is an agreement on the view that there has been an excess of mortality, mainly in the north regions of Italy and some papers described a clear difference between regions, with a clear picture of two or three areas with different mortality and morbidity. Aiming to offer a contribute on this field, the present study examined the trends of mortality during the first 4 months of 2020 in Italy according to the official data released by Italian National Institute of Statistics (ISTAT www.istat.it), and it compared them with findings from a previous interval of 5 years. Moreover, the study examined the effect of age in the trend of mortality, with a focus on oldest old.
Design and methods
We analyzed daily data on total mortality in the first four months of 2020 in Italy published by ISTAT (Italian National Institute of Statistics). We compare data of the first four months of 2020 with data on the same months in 2015, 2016, 2017, 2018, 2019. We considered data in each region of Italy: we summed daily data and calculated total mortality in the period 1st January – 30th April 2020. We calculated total mortality in the same period in the years 2015-2019. Then we calculated daily average death for each region, for each month and for each year.
Results
Tables 1–4 and Figures 1–4 show total mortality in Italy in each region in each month in 2020 with a comparison to the total mortality in Italy in each month of the previous 5 years. Each table and in each figure describe data on a group of 5 Italian regions.

Total mortality for month in the first 5 regions (Valle d'Aosta, Piedmont, Liguria, Lombardy and Trentino Alto Adige).
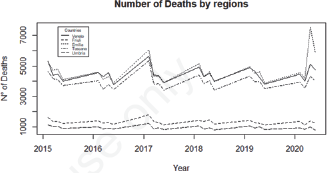
Total mortality for month in 5 regions Veneto, Friuli- Venezia Giulia, Emilia Romagna, Tuscany, Umbria.
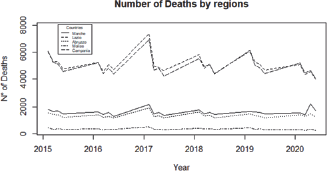
Total mortality for month in 5 regions (5 regions-Marche, Lazio, Abruzzo, Molise, Campania).

Total mortality for month in 5 regions (5 regions-Apulia, Basilicata, Calabria, Sicily, Sardinia).
Total mortality for month in the first 5 regions - Valle d'Aosta, Piedmont, Liguria, Lombardy and Trentino Alto Adige.

Total Mortality for month in the 5 regions - Veneto, Friuli-Venezia Giulia, Emilia Romagna, Tuscany, Umbria.

Total mortality for month in the first 5 regions - Marche, Lazio, Abruzzo, Molise, Campania.

Total mortality for month in the first 5 regions - Apulia, Basilicata, Calabria, Sicily, Sardinia).

As the month of March had the higher level of mortality in Italy in the first four months of the year 2020, we chose to focus our attention on this month. We calculated the daily mean of mortality in each region in March 2020, and the daily mean of mortality in each region in an interval of five years (2015-2019). Then we compared the number of deaths in March 2020 with the mean of the mortality in March in the previous five years.
Tables 5 and 6 compared the daily number of deaths in March 2020 with the mean of the daily number or deaths in March in the previous five years (2015-2019). We show data for each region, and we propose statistical comparison. In Table 5 we also ordered Italian regions by the number of inhabitants and population density. Table 6 shows that for some regions there is a clear difference in the number of deaths in the month of March of the previous 5 years and in the month of March 2020. Specifically, Lombardy, Piedmont, Emilia Romagna had the higher increase of deaths in March 2020, compared to the average trend in the previous five years in the same month; also, Veneto, Liguria, Trentino Alto Adige, Valle d'Aosta, Marche showed a increase of deaths in March 2020, compared to the average trend in the previous five years in the same month, but of minor entity. Lazio and Sicily showed a reduction of deaths in March 2020, compared to the average trend in the previous five years in the same month.
Comparison between March 2020 and the mean of March 2015-2019.

t-test on the comparison between March 2020 and the mean of March 2015-2019.

Discussion and Conclusions
This study has three aims. First, it aimed to describe data on mortality in Italian regions in the first 4 months of 2020 and to compare them with the trend in the previous 5 years (2015-2019). The number of total deaths for month and the daily average in each region showed an excess of mortality in some regions in the first 4 months of 2020. The excess of mortality is region dependent.2,12 As expected, we found that in the first months of 2020 there has been a significative increase of mortality in some North regions but with a different gradient (Lombardy, Piedmont, Liguria, Valle d'Aosta, Veneto, Emilia Romagna). In these regions, the month of March 2020 had the higher level of mortality, both on a daily base and on a monthly base. Moreover, there has been a different trend in other regions, with no increase of mortality or even with a slight reduction (see for example Lazio, Sicily). Second, with reference to the causes of excess of mortality, the number of total deaths in regions with the higher frequency of death is higher than the total official number of COVID-19 related deaths (as declared by official data of the Italian Minister of Health) (for example, about 28.000 total COVID-19-related deaths in Italy in the months of March and April of 2020). 13 Further research is needed to better understand these data.
Third, it aimed to discuss age differences in the trend of mortality during the first month of 2020, with a focus on oldest old. According to Italian National Institute of Statistics, the total increase in mortality is explained at 76.3% by people over the age of 80, 20% by people aged 65 to 79. Furthermore, the excess mortality observed is higher in the higher ages and it is more pronounced in men than in women (Report_ISS_Istat_2020_5_marzo.pdf). Other papers demonstrated again an age-effect, where the excess of mortality affects more the older ages.14,15 Again, further research is needed on this topic to better understand these data. By now, we can only propose some general hints of analysis: 1. the excess of mortality could be the effect of the high pressure that the outbreak put on Italian Health system 2. a part of the excess mortality would still be linked to the contagion from COVID19 but in people who died in their homes for which the presence of the virus was not detected. Both hypotheses are consistent with what emerged in that period. Again, with reference to the first hypothesis, the high burden due to COVID-19 pandemic on the Italian health system could have had the indirect effect of increase other causes of deaths (like the ones related to other disorders or diseases for which individuals had difficulty to access to care during the more critical phases of pandemic). In summary, in agreement with Wolf and colleagues (2020), 16 we could assume that excess deaths attributed to causes other than COVID-19 could reflect deaths from unrecognized or undocumented infection or deaths among uninfected individuals resulting from other effect produced by the pandemic, like the huge pressure on health system.17,18
This phenomenon could have had a higher effect on some countries, and in Italy in the North regions that are the first that have fight against pandemic (even if they had also the stronger health system). The same phenomenon could have had a higher effect on some group of oldest old, that from this perspective seems the more vulnerable group, mainly when they live in rest homes, nursing homes and similar facilities, like long-term care facilities,19,20 because, unfortunately, in the first phase of the outbreak, these institutions acted as a sort of incubator of infection. Some data demonstrated that for people living in Long-Term Care Facilities the risk of death increased about 4 times during the more critical phases of pandemic when compared to the previous years in some regions of Italy. 20
Moreover, further research is also needed to better understand different effects on other regions, in the center and in the South of Italy, where there had been a peculiar pattern of deaths.
We strongly believe that further research is needed in the field, even with a higher attention to the other phases of pandemic, like the current one. In this paper we choose to address the first months of 2020 because we consider these months as a clear model of the acute effect of pandemic and of the outbreak emergency, while the analysis of the other phases and of the current one, could give us some information about the effects of the pandemic on a longer time. Some lessons are learned about the acute phase of the pandemic: from an intervention perspective, these data could be useful to Government, scientific societies, stakeholders and health policy makers for planning and implementing specific interventions during the current and future steps of the COVID-19 Pandemic, taking into account a region-level approach (and even a provincelevel approach).12,21 Moreover, the same data are useful with the aims to define specific measures to prevent infection (like pharmacological ones, non-pharmacological ones and vaccines) and to prevent other general negative effect on Health system and on individual lives.1,12,16-18,22-24
Footnotes
The authors declare no potential conflict of interest.