
Abstract
Background
A community-based intervention was implemented to improve maternal, child, and adolescent health practices, promote financial literacy and enhance livelihood opportunities for young people in marginalized communities. A hypothesis related to our intervention was that peer-led education sessions on health and nutrition in conjunction with community mobilization would change communities’ perceptions towards maternal and child health.
Design and methods
This three-year intervention was done in the two districts of Rajasthan, India, namely Nagaur and Pali. The paper explored the changes in perceptions and practices that resulted from this intervention among women and adolescents. We performed a retrospective, qualitative effect evaluation of the project. Focus group discussions with married women (15-49 years) and adolescents (10-19 years), and in-depth interviews with frontline workers and village health committees were done. The qualitative data were translated, coded, and analyzed thematically using an inductive approach.
Results
Overall, 4853 women and 8158 adolescents were engaged in the intervention. The study seemed to have brought a change in some of the practices like postnatal care uptake, breastfeeding, and uptake of antenatal care among women, and enhanced awareness about sexual and reproductive health and harms of substance abuse among adolescents was noted. Around 23% and 67% of the young people from Nagaur and Pali, respectively, were linked with jobs in computer training centres, tailoring centres, and beauty parlours.
Conclusions
The intervention was perceived successful in improving many health and nutrition practices and livelihood opportunities among project beneficiaries, calling for a comprehensive and multi-dimensional intervention to target social determinants of health.
Significance for public health
This paper adds evidence on a community-based intervention using peer-led approach to improve maternal, child, and adolescent health and nutrition. This study provides valuable qualitative research to evaluate a community intervention in India. Our article highlights the key maternal and child health issues that can be addressed easily and the issues that are more challenging to achieve. Furthermore, the study sheds light on the need and importance of fostering financial security through empowering youth with skills and financial literacy and help them secure a livelihood.
Introduction
India is ranked 115 out of 162 countries in the global ranking based on the achievements of Sustainable Development Goals (SDG) with an index score of 61.1. The country has major challenges remaining in the transformations to achieve SDG-3 of good health and well-being.1 Despite India's ground breaking success in reducing maternal mortality by 77% in 26 years, the change has not been equitable and remarkable across all geographies and communities.2,3 States with the highest burden of maternal mortality, such as Uttar Pradesh and Rajasthan, have the worst overall performance in health development.3 Besides, women from marginalized communities (population belonging to socially backward classes, or those living below the poverty line) have the worst maternal health outcomes. For example, the rate of skilled birth attendance differs by 31 percentage points between the richest and poorest women and by 15 percentage points between women from non-marginalized and marginalized communities.4 Poor women from rural and remote areas and marginalized communities have limited access to maternal health care services, including antenatal care, skilled birth attendance, and postnatal care due to various socio-cultural and geographical barriers.5 Hence, there is a need to improve access to and utilization of maternal and child health care services for women, particularly from marginalized communities.
Increasingly, community-based interventions have been recognized as an important component of comprehensively-designed maternal health programs.6 However, recent systematic reviews have demonstrated that community-based interventions dependent on the health education of women alone may not be successful in improving the utilization of maternal and child health care services. Instead, health education programs integrated with multiple interventions greatly improved maternal health outcomes.7,8 Hence, community-based strategies must deliver a variety of services. There is emerging evidence on the impact of fostering financial security and social inclusion in reducing inequities for access to maternal health care.9,10 Ensuring livelihood can bring financial security and access to financial services to vulnerable people. However, there are limited livelihood opportunities for young people in India due to a lack of skills, education, and a huge competition.11 Gender inequality and rural-urban differences in access to job opportunities further add to the growing problem of unemployment and livelihood struggles for the marginalized populations. 12
Research on such evidence-based integrated health and livelihood development interventions informed the conceptual model of our intervention (Figure 1).13,14 The conceptual model informed that peer-led education sessions with beneficiaries would help in bringing behaviour change in the society together with mobilization of the communities.15 Concurrently, encouraging and empowering youth with skills would enhance their chances of employment. Youth information centres have been accepted as a medium to enhance knowledge and inculcate skills in youth .15,16 A hypothesis related to this model is that peer-led education sessions on health, hygiene, and nutrition in conjunction with community mobilization would change the perceptions in the families and communities towards maternal and child health. Besides, youth would feel empowered and skilled to pursue jobs in the local market. Employment will help to improve financial security that will address the limitations to access health services.

Conceptual model. The figure illustrates the conceptual model of the intervention that describes what were the problems or rationale behind the intervention and its strategies and what interventions were proposed to achieve the outcome. The three major intervention strategies were peer-led sessions, community mobilization, and youth livelihood training. The plus signs indicate that the three different strategies were worked upon together to achieve the outcomes.
Description of the community-based intervention
Objectives of the intervention
The specific objectives of the project were: i) to bring change in maternal, child, and adolescent health practices in the communities through a life course approach; ii) to create an enabling environment for enhancing accessibility and utilization of health services among women and adolescents; and iii) to promote financial literacy and linkages for improving livelihood opportunities among marginalized communities. The key strategies of the intervention included the health education of women and adolescents through structured sessions, modular training of young people on financial literacy and livelihood promotion, and one-to-one interactions with stakeholders for influencing the access to maternal and child health services.
Intervention settings
The project was implemented in two districts of Rajasthan, namely Nagaur and Pali. Rajasthan, a state in Western India, has a population of 60 million, a child sex ratio of 888, a female literacy rate of 52%, and a maternal mortality ratio of 182 per 1,00,000 live births.17,18 All the 32 districts of Rajasthan were ranked based on the gender-related development index, a composite index of health, education, and income indicators.19 The districts were further grouped into three categories: the highest one-third, middle one-third, and the lowest one-third groups. Two districts (Nagaur and Pali) were randomly selected from the lowest one-third group. One block was selected randomly from each of the two districts. The intervention was done in 28 and 29 villages in Nagaur and Pali, respectively. Both districts had poor maternal and child health indicators (Supplementary Table 1).
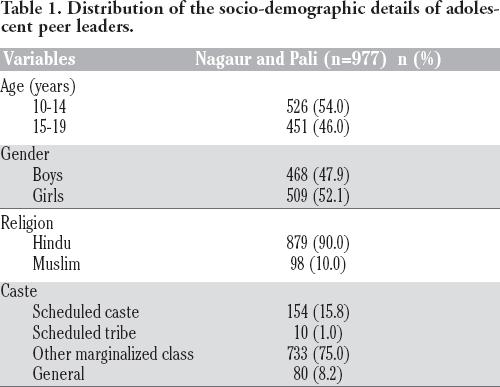
Distribution of the socio-demographic details of adolescent peer leaders.
Furthermore, the intervention population (married women in the reproductive age group (15-49 years) and unmarried adolescents) was selected to receive the intervention after community mapping and line-listing. We had a mixed team of 20 men and women, which included a public health specialist (n=1), district coordinators (n=2), outreach staff (n=16), and monitoring and evaluation officer (n=1). District coordinators and outreach workers belonged to the intervention area and were well versed in the local language and cultural practices. The roles of each of these implementing actors are given in Figure 2.

Roles of the implementation actors of the project. The figure depicts the key roles of the different implementation staff of the project. Four key implementation staff included public health specialist, district coordinators, outreach workers and monitoring and evaluation officer. The arrows indicate the flow of information among the implementation staff. VHSNC, Village Health Sanitation and Nutrition Committee; MIS, Management Information System.
Intervention activities
The outreach staff identified women and adolescents in the communities, and separate groups of 20-25 women and adolescents were formed. Further, separate groups were formed for adolescent girls and boys. In every group, one leader was selected, who was named as a peer leader. The outreach staff conducted 6- day training of the peer leaders in the villages on maternal, child, and adolescent health. These peer leaders had the responsibility to educate other women or adolescents on the health and nutrition issues in the villages. There were 540 peer leaders from the women's group. The socio-demographic details of the adolescent peer leaders are provided in Table 1. Peer leaders were provided small cash-based incentives to manage sessions, call participants for attending sessions, and use transport to reach the dropouts at their houses.
The health education program for women had 10-structured sessions distributed over ten months. The titles of the ten sessions were: pre-pregnancy care, safe motherhood, intra- and post-partum care, and prevention of parent to child transmission of HIV, prevention of malaria during pregnancy, newborn care, breastfeeding, and immunization, care during the post-neonatal period, and prevention of undernutrition among children. Similarly, six-structured sessions were conducted with adolescents. The names of these sixsessions were: understanding adolescence, understanding gender and sex, adolescent's rights, contraceptives, stress and emotions management, and prevention of anaemia. The sessions with the women were conducted in the villages at a suitable place (health centre, Anganwadi centre, or community hall). Anganwadi centres are the child development centres in the villages where women, adolescent girls, and children are provided supplementary nutrition, health education, and nutrition-related services.20 Each session lasted for 1.5-2 hours, beginning with the rounds of introduction, followed by the main content of the session, questions and answers, and lastly, a short story to convey the message of the session.
Besides, youth information centres were created in the villages. The youth information centres served as resource centres of infotainment, recreational activities such as indoor games, group discussions, and safe spaces for girls. In total, five youth information centres were created in Nagaur and four in Pali. The stakeholders who had an impact on the health practices of women and adolescents, such as husbands, mothers-in-law, and parents, were engaged through community events and mass meetings. A single one-day orientation workshop for frontline workers and medical officers was conducted in each of the two blocks to discuss about the prevention and management of anaemia and nutritional problems among women and adolescents, breastfeeding promotion, and family planning.
In addition, meetings were held with the members of the Village Health Sanitation and Nutrition Committees (VHSNC). VHSNCs are health committees serving as vehicles for community health governance. They are not only an institutional mechanism for the community to voice its needs, share experiences and issues regarding access to health services, but also provide support to frontline workers, facilitate service delivery at facilities, and catalyze village health planning.21 However, VHSNCs were not actively conducting monthly meetings as revealed during the project and evidenced by the previous literature.22 The program staff, by facilitating the conduct of VHSNCs, regularly ensured that the VHSNC members discussed and further addressed the issues of health, nutrition, and hygiene in the villages. At the time of our intervention, most of the community-based activities were done by frontline workers. However, studies highlighted that there were many challenges in the performance of frontline workers; as a result, outreach and effectiveness of the community health programs were limited.23 There were no existing peer-led programs in the community at the time of our intervention.
The young people were trained on financial literacy and livelihood promotion program through a three-day training workshop in both districts. The key issues discussed during the workshop included qualities of starting a business, business preface, requirements to establish an enterprise, business communication skills, preface of business conflicts, registration processes, principles of management and accounting, the opening of bank accounts, fund management, government schemes, marketing management, and non-financial assistance. An external agency facilitated the training. In addition, we sought support from the state development livelihood corporation and micro, small, and medium enterprises. The implementation of the intervention began in 2014 for three years.
The present study
While research has begun to evaluate the effects of integrated health and livelihood project in bringing behaviour change on quantitative outcomes, few investigators have explored the perspectives of change in behavioural practices and norms.9,13 The qualitative data can provide us with insights about what beneficiaries learnt from the project, what were the enablers or barriers of change, or what worked well and what did not. This has the potential to deepen our understanding of processes of behaviour change coinciding with the community dynamics, which otherwise may not be captured in quantitative measurements. This will help us in the future while designing community-based and peer-led interventions on health and livelihood, besides guiding us for measuring short- and long-term outcomes. The present study describes a retrospective, qualitative effect evaluation of an integrated health and livelihood intervention, aiming to explore the effects of the project on i) the perceptions and practices of women related to antenatal and postnatal care; ii) the perceptions and practices of adolescents related to health, nutrition, education, and livelihood and; iii) the social environment surrounding women and adolescents, including the changes observed by front line workers and village heads.
Design and Methods
Study participants
Qualitative data were collected from the project beneficiaries to assess what they learned from the project intervention and what they reported practicing in their lives. Focus group discussions (FGD) were done with women and adolescents, who were in the same area of the study and were associated with the intervention for at least one year. The frontline workers at the facilities were included in the study if they were associated with the intervention for at least one year and participated in the events or meetings organized during the project.
Qualitative analysis
The qualitative interviews at the end of the program were conducted by researchers not associated with the intervention. In total, 12 in-depth interviews (IDI) with frontline workers, four FGDs with women, four FGDs with adolescent boys and girls (two each), and two FGDs with members of VHSNC were conducted. Around 10-12 people participated in every FGD. Each FGD lasted for 60-80 min, beginning with the introduction, explanation on the objective of the assessment, and discussion on the key issues of the assessment.
It took an average of two months at the end of the intervention to conduct all the interviews. The intervention was delivered over a 30-months period from 2014 to 2017. The interviews or discussions were done at a suitable place in villages. The interviews were conducted by a female researcher in both districts (master-level education and not associated with the project). The researcher had the experience of conducting a handful of qualitative interviews in the past. The external researcher was assisted by the staff of the project in facilitating the meetings and managing audio recordings. The researchers met the participants for the first time during the interviews. At the beginning of all the interviews, the researchers introduced themselves as an investigator from MAMTA Health Institute for Mother and Child. The study participants were informed about the study goals and objectives.
All the interviews were recorded in Dictaphone, which were transcribed and written later. The interviews were conducted in the local language (Hindi). The transcripts were coded inductively using thematic analysis in Microsoft Excel (Excel v.2007, Redmond, WA, USA). The data-driven themes that emerged consistently related to change in perceptions of the people for health and livelihood were analysed. The analysis resulted in the following thematic areas:
Perceived changes in antenatal and postnatal care
Perceived changes in adolescent's health, nutrition, education, and livelihood, and
Frontline workers’ and villages heads’ perception of change in service utilization by women and adolescents and livelihood opportunities in communities
In addition, we collected the socio-demographic details and attendance of the beneficiaries (women and adolescents) who enrolled in the program during sessions. The socio-demographic details included age, gender, caste, religion, education status, and age at marriage. This additional data was also analysed using Microsoft Excel.
Results
Overall, 4853 women and 8158 adolescents were engaged in the intervention, out of which 68.2% of women and 52.0% of adolescents were from Nagaur, while 31.8% of women and 48.0% of adolescents were from Pali. The socio-demographic details of women and adolescents engaged in the intervention have been shown in Tables 2 and 3, respectively. Approximately 8% of the women had married before the age of 18 years. The majority of the population in the two areas were Hindus (96.4%). Around 86-87% of the adolescents and 85-87% of the women belonged to marginalized populations. More than two-thirds of the women who were enrolled in the intervention attended any education session in both districts.
District-wise distribution of the descriptive data of adolescents engaged in the intervention.

District-wise distribution of the descriptive data of the women engaged in the intervention.

Change in the perceptions of women on maternal and child healthcare practices
Based on the interviews, it seemed that the perceptions related to preconception, antenatal, and postnatal care changed, whereas some of the practices with regard to these themes remained unchanged. It appeared that pregnant and lactating mothers were not aware of the importance of delayed marriage, delayed birth of the first child, and early antenatal visit before the intervention, influenced by cultural norms and traditions. The interviews seemed to indicate that such perceptions had changed after the intervention. Women now understood that a woman should marry when she is at least 20 years old and should undergo pregnancy at least 2-4 years after marriage. However, our interviews indicated that practices related to the visit to the health facility within the first trimester did not change. The qualitative findings suggested that socio-cultural norms and superstitious thoughts prevented women from disclosing their pregnancy status within the first three months.
A woman should have a child four years after marriage. A woman is weak in the early years of life and would give birth to a weak child. She should enjoy her married life before getting pregnant and understand her relations (Women during FGD).
If we visit a health facility within the first trimester, people will come to know. And evil's eye will be on us. This will hamper the growth of our child. We do not want this (Women during FGD).
The qualitative findings suggested that women realized the importance of the consumption of nutritious food during pregnancy. Women realized that locally available food products in their villages, such as milk and milk products, were nutritious and would keep them healthy. The qualitative data gave the impression that women became aware of the common danger signs in pregnancy, such as bleeding, abdominal pain, and high fever, antenatal checkups, immunization of child, anaemia, iron-folic acid consumption, and blood tests during the project. However, it seemed that the barriers in accessing health services, such as long distances to the facility from villages, lack of enough medical staff, and disrespectful attitude of the health centre staff were persistent. Yet, it appeared from the interviews that despite such barriers, women opted to deliver in a hospital and received 48 hours of postnatal care where they were taken cared of well and given counselling on new born care.
We got to know a lot about health check-ups during pregnancy in the project. We should get abdominal ultrasonography done, take medicines and vaccines, blood tests, registration at Anganwadi centre, and receive nutritional counselling. We need to get our children immunized to protect them against disability and illnesses. We need to consume iron-folic acid tablets because of anaemia. We did not face any problem while taking iron-folic acid tablets (Women during FGD).
There are problems; for example, midwives are not available at the centres. They come for delivery mainly, and the sub-centre is quite far from our village. In case we fall sick or develop complications, we had to travel a long distance to access services. Moreover, it's difficult to call an ambulance or any other transport because of a lack of good roads (Women during FGD).
We tend to arrange our vehicle for transport to the hospital for delivery, or we hire a taxi. We had even rented a vehicle for this purpose. We had to pay rupees 2000-4000 for the vehicle, but it is ok. We had to face more problems if we deliver at home (Women during FGD).
The FGD gave the impression that the consumption of ironfolic tablets was not common among pregnant women; despite being emphasized during the intervention. The reasons included for not consuming iron-folic acid tablets were its side effects, such as nausea, headache, and metallic taste. It seemed that women were not consuming supplementary food supplied at Anganwadi centres because of its low quality. The discussions indicated that women had understood about exclusive breastfeeding practice and its importance during the intervention.
We need to give the yellow milk that comes out initially to our child and breastfeed them until six months of age. But we need to give ‘ghutti’ (a combination of Ayurvedic medicines) at the time of birth to the child. It's a tradition in our villages, and we could not avoid it (Women during FGD).
Furthermore, it appeared that misconceptions related to breastfeeding among women, to some extent, were addressed by the interventions.
Earlier, we have been asked not to breastfeed our child if we were sick or feel weak (Women during FGD).
The qualitative data suggested that women were aware of family planning methods even before becoming a part of the project. They were aware of the side effects of multiple pregnancies and a big family. They recited a slogan, ‘We two, ours two’ in the local language (Hindi). However, it appeared that the use of contraceptives among newly married couples was low, despite having knowledge about them. The discussions seemed to indicate that women's attitude towards the use of contraceptives was not positive, and most of these women experienced pressure from their families to give birth to a child soon after marriage.
We know about Copper T, sterilization, etc. We are also given condoms by midwives for husbands. But our husbands don't use them. Why should we take condoms from health workers if we have to undergo sterilization? After sterilization, we had complaints of lower backache and weakness. We had to do a lot of household work, including chopping grasses in the fields. If we fall sick, how will the work at home be managed? (Women during FGD).
The findings gave the impression that women were not aware of HIV/AIDS or sexually transmitted infections. Many women were referred for HIV testing during pregnancy, but they were unaware of the reasons for the testing. In addition, it seemed that the uptake of postnatal care visits was low earlier, and in fact, many did not know about it. However, women's postnatal care visits by frontline workers had increased post-intervention. Women shared that they benefited from attending meetings with MAMTA. They got the clarity of many issues and felt encouraged to change more and more women.
Change in perceptions of adolescents with regard to health, nutrition, education, and livelihood
The qualitative data suggested that adolescents attended meetings conducted by MAMTA regularly, but many adolescents did not visit youth centers during their leisure time. The common reasons enumerated included the long distance between households and the center, limited availability of time to visit the center after school, and the parents’ denial of permission for the visit. It seemed from the data that early marriage was still common and was perceived not to have been changed. It appeared that girls were married off early before the legal age of marriage. The findings gave the impression that the norms of early marriage were prevalent though adolescents knew about its harmful effects. The common reasons for early marriage that emerged from the interviews were traditional beliefs, societal pressure, and parent's wish.
We were told in meetings that the marriage should be delayed. We believe that the age of marriage should be 24 for boys and 22 for girls, at least. By this age, boys and girls are mature, and they know how to run a family. And before this age, girls should study. Child marriage is wrong. Girls are not mature before the age of 18 years, and it's difficult for them to handle themselves, their families, and child. Big responsibilities at an early age are not good (Adolescent girls during FGD).
The results indicated that school drop-out was common among boys and girls even at the end of the intervention. It seemed that the reasons for drop-out among boys were pressure from the families to earn and contribute to the income of the family and lack of good quality teachers in schools. On the contrary, long distances to secondary schools, poverty, issues of safety or security, and early marriages were the common reasons for the drop-out of girls. This gave the impression that as a result of lower education, both boys and girls had limited opportunities for employment.
An old custom of selling and auctioning their daughters is still common in some of the communities of Nagaur (Adolescents during FGD).
It was indicated from the data that both boys and girls had a very comprehensive knowledge of sexual and reproductive health and rights, which beneficiaries reported to have increased postintervention. They were able to explain what are the typical bodily changes and growth among boys and girls. Adolescents reported that they had been benefited by coming to the meetings organized during the project. It appeared that talking about sex education was considered taboo, and most of the people were hesitant in talking about it openly. However, discussions gave the impression that boys and girls considered men to be equally responsible for household work post-intervention. They believed that girls should also be given an opportunity to study, work, and drive. It seemed that