
Abstract
Background
Studies have shown that public awareness of ovarian cancer is weak, and women are often diagnosed at late stages when treatment is difficult. This study aimed to determine the barriers for seeking early medical care and level of knowledge and awareness among women regarding ovarian cancer.
Design and methods
A structured questionnaire was designed and adapted from the validated cancer awareness measure.
Results
The recognition level of ovarian cancer symptoms among women in this study varied from 12-51%, and the most alarming ones, back pain, eating difficulties, and persistent abdominal pain, were missed by most of the surveyed women. The most recognized ovarian cancer risk factors were never being pregnant, having a history of infertility, and going through menopause, while the least recognized was having personal or family history of breast cancer. Non-UAE nationals women with higher educational levels had better knowledge of ovarian cancer compared to their peers.
Conclusions
A change or implementation model is highly recommended in order to improve women's awareness of ovarian cancer symptoms. Strengthening education among women with regards to risk factors, early symptoms, and the need to seek early medical help should help to increase ovarian cancer awareness and reduce a delay in the diagnosis.
Significance for public health
In the absence of effective screening, “appropriate clinical suspicion” of the signs and symptoms of the ovarian cancer is currently the best strategy to detect the disease. To reduce the diagnostic interval, several countries have implemented referral guidelines and organizational changes. Most of these guidelines suggest that individuals presenting with symptoms indicative of cancer (alarm symptoms) should be urgently referred to specialized investigative trajectories. However, many studies worldwide have shown that public awareness levels of ovarian cancer are poor, therefore women are often diagnosed at late stages when treatment is difficult. Our findings demonstrate that the overall level of recognition of risk factors and symptoms of ovarian cancer among women in the UAE is indeed low and within a critical level. Thus, strengthening education among women with regards to risk factors, early symptoms, and the need to seek early medical will be helpful in increasing ovarian cancer awareness and reducing the delay in diagnosis.
Introduction
Ovarian cancer is one of the most challenging gynecological cancers in the world, with a profound negative effect on the quality and length of life affecting more than 70% of the women diagnosed with advanced disease. 1 The absence of specific symptoms and useful screening tests make it difficult to establish an early diagnosis of ovarian cancer. In addition, most women have little or no knowledge about the risks, possible symptoms, and the dangers ovarian cancer poses to them. 1 Worldwide, ovarian cancer is the seventh most frequent cancer in women, accounting for 3.6% of various cancers diagnosed in women. It is the third most prevalent genital tract malignancy after cancers of the cervix and uterus. 1 According to the UAE cancer registry report in 2014, ovarian cancer is the fifth most commonly diagnosed cancer affecting women with a prevalence of 4%. 2
In the past, ovarian cancer was believed to be a silent killer due to a lack of symptoms in the early stage leading to late presentation of the disease with its related high mortality rates. 3 In the absence of effective screening, “appropriate clinical suspicion” of the signs and symptoms of the disease is currently the best strategy to detect ovarian cancer. 4 The hypothesis that ovarian cancer outcomes could be improved through better symptom recognition has been primarily advanced by Goff et al. who proposed a “symptom index” as a tool to screen women for further evaluation for ovarian cancer. The index is considered positive if pelvic or abdominal pain, increased abdominal size, bloating, difficulty eating, or early satiety occur more than 12 times per month but for less than one year. 5 Unfortunately, because these symptoms are non-specific, they may be attributed to other causes either by the women themselves 6 or by an inexperienced physician. 7 When these symptoms are detected promptly and investigated appropriately, they may aid early diagnosis and management, resulting in better prognosis and outcome for the patients. 8 This is because the survival rate of ovarian cancer depends significantly on the stage of the disease with the early-stage disease having more than a 90% five-year survival rate compared with less than 30% in advanced stage disease. 9 The risk of developing ovarian cancer is increased with advanced age; family history of ovarian, breast, uterine, and colon cancer; use of fertility drugs and nulliparity. 9 However, the awareness of these risk factors and symptoms of ovarian cancer is generally poor among women.8,9
Several studies have shown that late-stage cancer diagnosis is associated with reduced survival. 10 This is especially the case for gynecological cancer, and timely diagnosis and treatment are thus considered essential for prognosis. For most patients with ovarian cancer, the diagnostic process is still initiated based on symptom presentation, although some patients are diagnosed through screening programs. 11 To reduce both the patient interval and the diagnostic interval, several countries have implemented referral guidelines and organizational changes. 12 Most of these guidelines suggest that individuals presenting with symptoms indicative of cancer (alarm symptoms) should be urgently referred to specialized investigative trajectories.
Many studies worldwide have shown that public awareness levels of ovarian cancer are poor, and women are often diagnosed at late stages when treatment is difficult.13,14 Poor public knowledge of early symptoms of cancer has been considered to be the predominant reason for late-stage presentation or delay in the diagnosis. 15 The purpose of this study was to determine the level of knowledge and awareness among women regarding ovarian cancer risk factors, symptoms, and barriers to seek early medical care in the UAE.
Design and Methods
Study design
This descriptive cross-sectional survey was conducted among women (aged 20 and above) of all nationalities; from September 2019 until April 2020.
Study participants and procedure
The participants living in the UAE and willing to provide written informed consent were selected for the study. The participants were assured of the confidentiality of the information provided and the protection of their rights to privacy, mandated by the research ethics guidelines of the human research ethics committees. The inclusion criteria mandated participants to be women aged 20 and above, who are not health care providers, willing to participate in the survey and able to sign informed consent, having appropriate cognitive skills, ability to read and understand in English or Arabic (e.g., the local language). Both UAE citizens (nationals) and expatriates were included in the study. Participants that had poor mental health and were unable to meet any of the above criteria were excluded from the study. The sample size was calculated using epidemiological information for a population of 682,000 (population of females in the UAE), with an alpha of 5% and a 95% confidence level. We needed a minimum required sample size of 384. 16
Survey design (evaluation tools)
A structured questionnaire was designed and adapted from the validated cancer awareness measure (CAM), 1 ovarian cancer awareness measure (ovarian CAM), 17 and a questionnaire developed by the National Ovarian Cancer Coalition. 18 The evaluation tool was then pre-tested among 20 women to assess the ease of understanding and time required for completion. The bilingual questionnaire in Arabic and English is represented in APPX I. The survey instrument consisted of 44 items. The first part of the questionnaire collected sociodemographic data, including Age, Nationality, Ethnicity, Marital Status, Education Level, Employment Status, Monthly Family Income (AED), history of cancer, Smoking status, and Body Mass Index (BMI). The remaining sections of the questionnaire focused on knowledge and attitude toward ovarian cancer.
Selected questions under ovarian cancer knowledge (30 questions), and practices (4 questions) were used to develop a scaled scoring system to categorize these aspects as good, fair, or poor. Each correct or favorable answer chosen by participants was given one or two points; then, the points were summed for each participant. No points were deducted for wrong or unfavorable answers. The participants’ scoring system was as follows:
- Knowledge: Good (12–18 points), Fair (6–11 points), Poor (0–5 points)
- Practice: Good (7–10 points), Fair (3–6 points), Poor (0–2 points).
Data analysis and statistics
All collected data was entered into STATA version 15 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC.) for statistical analysis. Descriptive statistics were computed for the socio-demographic variables. The overall responses to each item of the survey were recorded as a percentage of the total. The percentage differences in the total responses were determined using the Chi-square test and statistical significance recorded for non-parametric data. For all analyses, alpha (α) was set at 0.05. We selected only those variables that had a moderate or higher correlation (>0.40) that was also statistically significant (p<0.05). A Pearson correlation of 0.00-0.19 is considered to be very weak, 0.20-0.39 weak, 0.40-0.59 moderate, 0.60-0.79 strong, and 0.80-1.0 very strong. We also calculated Φ as an effect size for all significant correlations (0.0-0.19 is weak, and 0.20-0.49 is moderate and >= 0.50 is strong).
Results
Out of 602 individuals approached, 532 agreed to participate in the study (response rate of 88%). The majority of our respondents were between 25-39 years, UAE national, with middle eastern ethnicity, retired or homemakers, had college or higher degrees certificate, married, had low income, never smokers, and having an average body mass index (BMI) (Table 1). Most of our respondents have read about ovarian cancer, had regular check-ups with physicians, did not have a family history of ovarian or breast cancer.
Descriptive demographic characteristics of participant women (n=532).

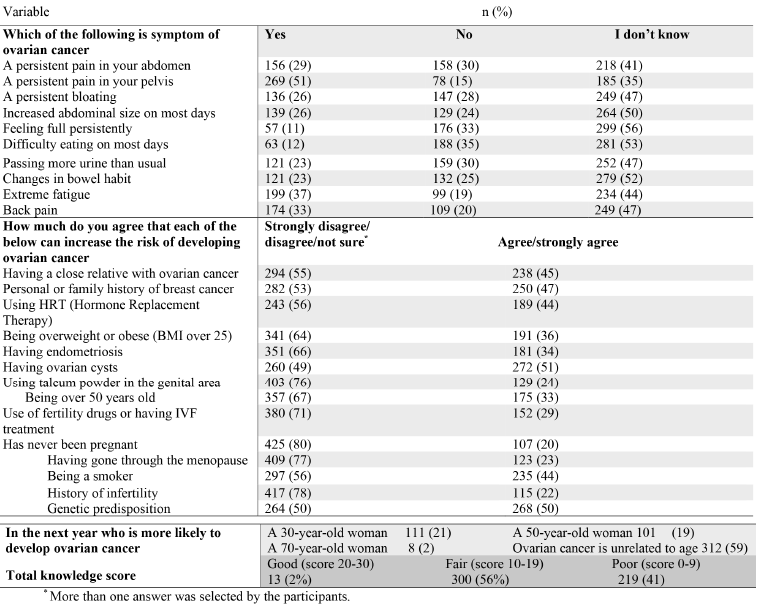
It was encouraging that the majority of individuals surveyed mentioned that they had heard about ovarian cancer; however, when we assessed their knowledge, the majority had fair or poor knowledge (Table 2). When evaluating the attitude of participants, the majority (379, 71%) mentioned that if they notice a symptom that might be a sign of ovarian cancer, they will visit a doctor within a week. Yet, most of the participants (376, 71%) mentioned that they are not that confident on noticing an ovarian cancer symptom and most of the participants did not relate age with the incidence of cancer. We calculated Pearson's correlation coefficient between variables; a multiple regression model was also fitted to explore the role of possible predictors of the knowledge score. There were no statistically significant predictors of the Knowledge score using a multiple regression model.
Knowledge on ovarian cancer among the women participants (n=532). The answers were on Likert scale as a five-point scale; however, they were re-grouped to 3 scales for knowledge scoring.
There was a significant difference (p<0.0001) between UAE nationals and non-UAE nationals on the regard of hearing about ovarian cancer, having a family history of ovarian cancer (p<0.0001), and having a family history of breast cancer (p<0.0001) (Table 3). There was a significant difference between educated and non-educated women participants in confidence level regarding noticing ovarian cancer symptoms (Figure 1). Having a history of cancer, or having a family member or a friend with history of cancer was significantly associated with higher ovarian cancer knowledge score. Reading about ovarian cancer was significantly associated with BMI (p<0.001) and having a regular checkup with physicians (p<0.0001). There were no statistically significant predictors of the Knowledge score using a multiple regression model. Knowledge score was only significantly associated with educational level (p<0.01).

There was a significant difference between educated and non-educated women participants in confidence level regarding noticing ovarian cancer symptoms.
The relationship between knowledge and practice on ovarian cancer with demographic characteristics among participant women (n=532) are presented.

Discussion
Ovarian cancer has been regarded as a “silent killer” due to the majority of patients being diagnosed at later stages of the disease (60% at stages III/IV) with low 5-year survival rates (6-22%). 19 To our knowledge, this is the first study conducted in the UAE to evaluate the level of awareness among women of ovarian cancer risk factors, symptoms, and anticipated time to seek early medical help should they develop suspicious symptoms. The recognition level of ovarian cancer symptoms among women in the UAE in this study was varied from 12-51%, and the most alarming ones, back pain, eating difficulties, persistent abdominal pain and bloating, were missed by most of the surveyed population. The most recognized ovarian cancer risk factors among UAE women were never having been pregnant, having a history of infertility, and going through menopause, while the least recognized were having a personal or family history of breast cancer, having ovarian cysts, and having a genetic predisposition for cancer. Previous studies conducted in several countries, such as USA, Malaysia, Oman, and Jordan, have shown that knowledge of risk factors of ovarian cancer among women was also low as found in our study.1,3,20,21
The observed positive association between education level and awareness of ovarian cancer risk factors and symptoms indicate that educated women are in a better position to access and understand information regarding ovarian cancer. It is not surprising that women with a tertiary level of education had significantly better knowledge as compared with their counterparts. This is similar to the findings from other countries, where women with higher levels of education were more knowledgeable of the symptoms and risk factors of ovarian cancer.6,22 Thus, education is an essential factor in increasing awareness of cancer symptoms and predisposing cancer risk factors, such as smoking, physical inactivity, obesity, and an unhealthy diet. 23 The role of education in increasing awareness among women of risk factors and symptoms of ovarian cancer in this study confirms findings from earlier studies conducted worldwide, which showed that people with higher levels of education recognized cancer symptoms better than those who were literate alone or less educated. 20 Indeed, previous studies have shown that a low level of education is associated with a delayed presentation among breast and colon cancer patients, whereas those with a higher level of education showed a greater knowledge of early symptoms. 15,24
Our study also revealed that women were more knowledgeable about the risk factors of ovarian cancer compared to its symptoms, and this is consistent with the findings of another investigation. 21 Although participants did better in recognizing ovarian cancer's risk factors than its symptoms, it is still evident that they have only a low knowledge level. Knowledge of ovarian cancer risk factors is fundamental; it may facilitate participation in screening programs and early detection.
This emphasizes the potential importance of raising women's awareness of the symptoms and risk factors, particularly in a country like UAE, where low awareness and knowledge levels seem to be dominant. This could be achieved by using announcements in the general media and social media channels. Leaflets could be distributed in local health centers, and hospitals in different regions in the UAE that might help to increase ovarian cancer awareness. Investigating potential interventions to increase awareness would seem to be the next step in our research. Besides, ovarian cancer awareness programs comprising regular lectures and workshops for women in general and women in secondary schools and universities should also be considered. When developing such programs, specific considerations for a UAE context should be borne in mind. First, an educational program should target women with low incomes and low levels of education. Second, these programs should be freely developed and easily accessible to the former group at schools, and primary health care centers close to their homes. To improve women's awareness of ovarian cancer symptoms and change their attitudes toward early detection practice and programs, using a change or implementation model is highly recommended.
Conclusions
Our findings demonstrate that the overall level of recognition of risk factors and symptoms of ovarian cancer among women in the UAE was low and within a critical level. Thus, strengthening education among women with regards to risk factors, early symptoms, and the need to seek early medical help should help to increase ovarian cancer awareness and reduce a delay in diagnosis.
Limitation of study
The results of this study are limited due to the cross-sectional study design; hence, any association found from the results cannot infer causal relationships. The findings of the study cannot be generalized for a larger population as the study respondents were recruited from the Dubai health authority, but could be considered indicative of the context measured. Nevertheless, a more extensive national study with recruitment of women from all emirates in the UAE is needed for better representative sampling.
However, despite these limitations, the present study findings may be helpful to the health policymakers, health educators, clinicians, and nursing professionals in designing the interventions to increase the knowledge and awareness of women in the UAE on ovarian cancer symptoms and risk factors.
Footnotes
Acknowledgments
Appreciation is expressed to all participants in this study.