
Abstract
Background
Acute otitis media (AOM) is the most common disease in young children requiring antibiotic treatment. Information on AOM-related determinant risk factors in primary school children is still limited, particularly in Indonesia. This study aims to identify risk factors related to AOM in primary school children in Banyumas Regency, Central Java, Indonesia.
Design and methods
This is an analytical study with a casecontrol design in Banyumas Regency, Indonesia. 3574 children from 6 regions of the Banyumas Regency were recruited for the screening of AOM detection, and confirmation of AOM diagnosis was determined by Otolaryngologist. One hundred and twentyfive cases and 125 control were involved in this study. Data collection was carried out using a structured questionnaire focusing on several variables such as household cooking fuel, house environment, smoking exposure, knowledge of parents, and nutrition status. Univariate, bivariate using chi-square and multivariate with regression logistic was conducted for data analysis.
Results
This study highlights the risk of household firewood use (p=0.003), poor nutritional status (p=0.009), and a family history of ear infections (p=0.015) with an increased risk of otitis media.
Conclusions
Household firewood use, poor nutritional status and family history of ear infection are factors associated with the occurrence of acute otitis media. It is necessary to provide public health education to prevent exposure to fuel at risk for children and to improve their nutritional status.
Introduction
Significance for public health
This study has important public health benefits because it offers valuable information about Acute Otitis Media (AOM) that is still limited in previous studies, particularly in Indonesia. This study confirms that problems related to AOM are still important because cases are still present in the community, particularly among primary school children. The basic advantage of this paper is the information that household firewood use, poor nutritional status and family history of ear infection are factors associated with acute otitis media in primary school children. This critical knowledge should be followed up by related parties to prevent the incidence of AOM cases in the community.
Acute otitis media (AOM) is one of the most common infections in early childhood and can be considered as a complication of upper respiratory tract infections. 1 This disease is characterized by the presence of middle-ear effusion and the acute onset of signs and symptoms caused by middle-ear inflammation. 2 Symptoms of AOM include earache in older children; or pulling, tugging, or rubbing of the ear or non-specific symptoms such as fever, irritability, or poor feeding in younger children. Signs of AOM involve a distinctly dark, yellow, or cloudy tympanic membrane. 3 The detection of AOM is improved by the presence of a bulging tympanic membrane, air-fluid level behind the tympanic membrane, tympanic membrane perforation, and/or discharge into the ear canal. Pneumatic otoscopy and/or tympanometry can be used to determine the presence (or absence) of middle ear effusion (MEE). For children with breathing tubes (grommets) in place, the discharge of the ear is a symptom of AOM, where the fluid that has collected in the middle ear flows through the tube into the child's ear canal. 4 The most common bacterial causes of AOM are Streptococcus pneumoniae, non-typeable Haemophilus influenzae, and Moraxella catarrhalis. There is increasing evidence that the predominant causative pathogen in AOM is changing from Streptococcus pneumoniae to non-typeable Haemophilus influenza since the introduction of pneumococcal conjugate vaccines. Group childcare outside the home and passive smoking is thought to be the most important risk factor for AOM. 5 Otitis media (OM) cover a diverse group of diseases, which contain some degree of inflammation or infection located in the middle ear and the tympanic membrane. OM is also the primary cause of narrow and broad-spectrum antibiotic prescriptions for children in developing countries, including Indonesia. There are several types of otitis media, including acute otitis media (AOM), effusion otitis media (OME), chronic suppurative otitis media (CSOM), and adhesive otitis media. 6 In Indonesia, the prevalence of CSOM is relatively high, with the majority of diseases occurring in rural areas. High rates in rural Bali with early progression to tympanosclerosis suggest a significant burden of potentially vaccine-preventable disease. 7 AOM is still considered a neglected disease in Indonesia since the community seems not to have enough awareness of this disease. The previous study stated that 38 children from Surabaya, Indonesia, who suffered from chronic suppurative otitis media (CSOM) were studied using the strict microbiological methodology. 8 Information on risk factors related to AOM in children is also very limited, therefore, this study focuses on the AOM case in the community. A previous study identifying risk factors for chronic otitis media (COM) and recurrent otitis media (ROM) and reveal that snoring, previous history of AOM/ROM, second-hand smoke, and low social status are important risk factors for COM/ROM. 9 Another study also found that low parental educational attainment, exposure to smoke, indoor exposure to mold, laryngopharyngeal reflux disease, and the lack of breastfeeding; an increased risk of otitis media recurrences were observed in the presence of an allergy, persistent cough, and runny nose. 10 However, there is no study yet about the risk factor of AOM in children, particularly in Indonesia. The objective of this study is to determine the risk factor of AOM in primary school children in Banyumas Regency. Results of this study will provide valuable information about risk factors which related to incidence of AOM. Identification of modifiable risk factors could give important input for AOM prevention in community.
Design and Methods
Description of the study area
The study site used in this analysis is the Banyumas Regency, located in the southwest of Central Java Province, Indonesia. Coordinates for this location are as follows: 108″ 39’ 17″ – 109″ 27’ 15″ East longitude, and 7″ 15’ 05″- 7″ 37’ 10″ South latitude. The total area is 132,760 km2, with a population of 1.85 Million inhabitants at a male to female ratio of 50:50. Banyumas Regency consists of 27 sub-districts and has 39 community health centers and a total of 331 villages. The environment in Java is characterized by a tropical monsoonal climate, with a dry season lasting approximately 6 months and a heavy monsoon the rest of the year. Total annual precipitation averages at 1755 mm (69.1 inches) and there are 2975 hours of sunshine on average per year. The location of this study was the selected primary school in the Banyumas Regency.
Study design and sampling
This is an analytical study with case-control design in Banyumas Regency, Central Java Indonesia. The population of this study is all primary school children in Banyumas which reach 50,000 students. Determination of the number of samples was carried out by software calculation, taking into account the estimated proportion of the previous research which is 0.0245 (with an error rate of 0.005, a confidence level of 95%), with the acquisition of a total sample of 3574 children. The distribution of primary schools in this study was carried out by stratified sampling in 6 regional divisions in Banyumas Regency. Primary school participation requirements/inclusion criteria used in this study are schools with more than 200 students. The 3574 samples were distributed to 6 regions of Banyumas Regency, namely in Region 1: Pekuncen, Ajibarang, Region 2: Karanglewas and Cilongok, Region 3: Rawalo and Kebasen, Region 4: Sumbang and Kembaran Region 5: North Purwokerto, South, West Purwokerto and Region 6: Kalibagor, Banyumas and Kemranjen. The selection of primary schools in the chosen areas was made based on inclusion criteria. There are 9 elementary schools selected for screening tests in six regions of the Banyumas Regency. The location of the primary school in the study site can be seen in Figure 1.
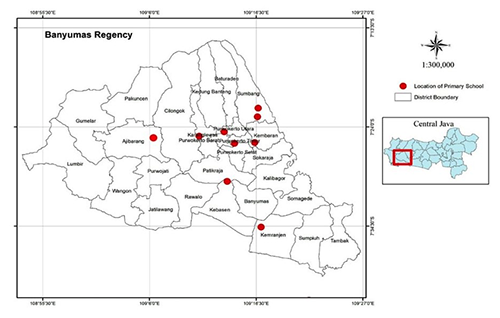
Location of the primary school at the study site, the red dot indicates the location of the primary school.
Screening and detection of AOM
This study has received permission from the health office, education office, and elementary school where the study was conducted. Screening for AOM was carried out by a clinician, Faculty of Medicine, Jenderal Soedirman University, Purwokerto, Indonesia. The inclusion criteria for AOM sampling were patients who experienced a cough and cold for approximately one week and experiencing pain in the middle ear. Informed consent was obtained from the parent of the children, which was also signed by the witness. Based on screening tests 987 children from 3574 were classified as the suspect of AOM. Then confirmed diagnosis was determined by otolaryngologist and 166 children diagnosed as positive cases of AOM. From 166 positive cases, only 125 participants were willing to partipate in this study.
Data collection
One hundred and twenty-five case group from positive AOM and 125 control group were recruited in this study based on diagnosis by ENT specialist (otorhinolaryngologist). Determination of the case by an ENT specialist based on otoscopy examination of suspected children. The control group was the children who negative based on the screening test and taken with the same sex and class matching criteria. Data collection was obtained by a structured questionnaire about sample characteristics such as nutritional status, birth order, parental education, parental occupation, parental income, number of family members, history of ear infection, history of allergies, history of acute respiratory infections, snoring habits. In addition, it was measured related to parents’ knowledge of AOM and also observed the condition of the home environment by visiting respondents’ homes. Several variables related to the condition of the house observed include the presence of smoke disposal, cooking fuel, the condition of the roof, walls, windows, and exposure to cigarette smoke in the house. Questions were answered by parents or guardians of these children. Informed consent was given to parents of students verbally and in writing before data collection was carried out. The consent form was signed by the parents or guardians of students which were also signed by the witness. Recall bias has been mitigated by using a structured questionnaire with validated questions.
Data analysis
Univariate analysis of each variable was described, and then bivariate analysis was carried out using chi-square to analyze the correlation between independent variables and dependent variables. Multivariate analysis using logistic regression was conducted to determine the most influential variables to the incidence of AOM by the enter method.
Results
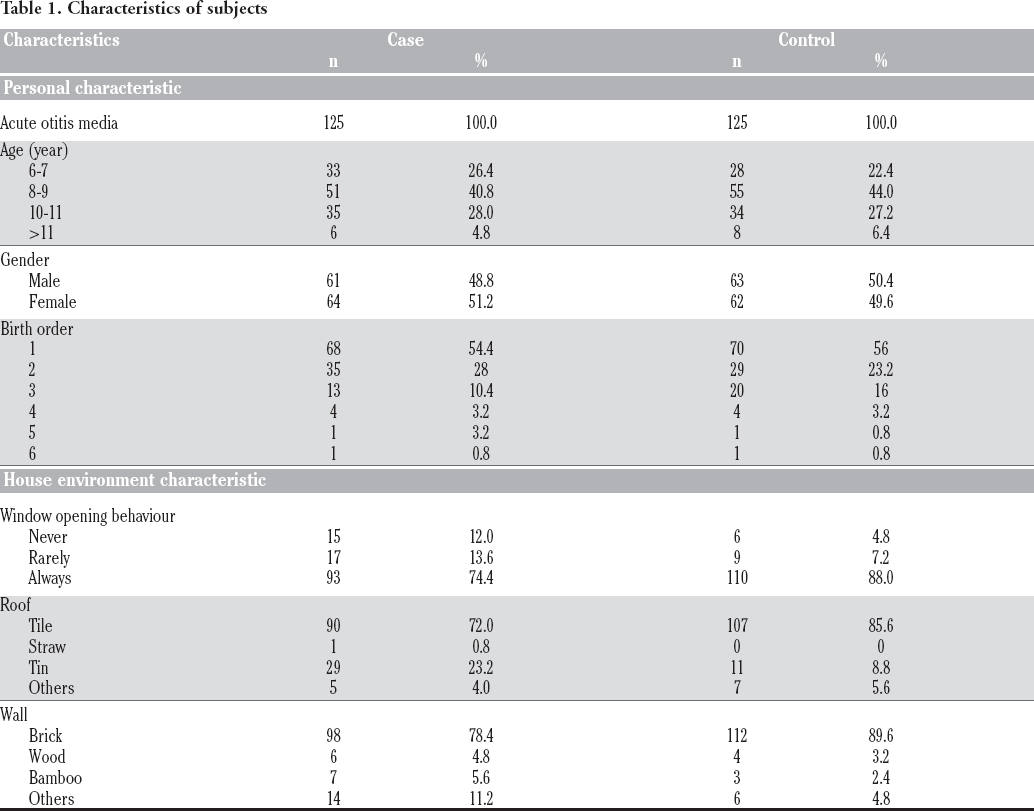
Of 3.574 children, 166 were diagnosed with AOM, so the prevalence of AOM in the Banyumas District was 4.64 percent (95% CI=3.95-5.32). Nevertheless, only 125 supporting participants can continue engaging in this risk factor study. The features of the participants and their house environment variables can be seen in Table 1. Characteristics of the research sample showed that the comparison between men and women in the case group was not quite different. Meanwhile, 40.8% of children diagnosed with AOM in primary schools are 8-9 years of age. Then for environmental characteristics, most of the case group (72.0%) and the control group (85.6) had houses with tile roofs. In the meantime, the knowledge of AOM in parents is also relatively low in both the case and control groups. 16.8% of children in the case population have had a history of prior ear infections. We performed a bivariate analysis test of several variables with the incidence of AOM, and the results are shown in Table 2.
Characteristics of subjects
Risk factors analysis.

All variables tested were then evaluated by bivariate analysis to analyze their relationship to AOM events. Based on the bivariate analysis, there are four variables linked to AOM: family history of ear infection, smoking exposure, household cooking fuel, and nutritional status. Multivariate modeling analysis with multiple logistic regression with the enter method is conducted to determine which variable is most important to AOM. The final results of the multivariate are shown in Table 3. Household cooking fuel turned out to be the variable most associated with AOM with an Odds Ration (OR) value of 3,437, which means that households using wood fuel for cooking have a chance of 3,347 times that their children being exposed to AOM.
Multivariate analysis.

Discussion
Epidemiological AOM studies in Indonesia are still very rare as it is still considered a neglected disease. While this research indicates that there are still cases of this disease in the population, they have not been reported. The detection of risk factors is also essential to the determination of AOM prevention efforts. The disease is a neglected disease in society so that the community's knowledge and understanding of how to prevent the disease are still weak. Knowledge of risk factors for this disease in Indonesia is still very limited, so this study was conducted to provide useful information to reduce the incidence of this disease in the population. As the AOM case number report in health institutions in Banyumas Regency is inadequate, we perform a clinical examination in children in selected primary schools by ear, nose, and throat/ENT specialist who has been involved in the study. Based on the results of the examination, the prevalence of OMA in the Banyumas Regency was 4.64%. This percentage is quite high because some previous studies in Indonesia such as in North Sumatra province recorded a prevalence of 2.1. 11 A study by Anggraeni et al. (2019) in 7005 public school children (6-15 years) in Indonesia found that the prevalence of OM was 2.5%. 12
In this study, it was found that there are several variables related to the AOM, i.e. AOM history, nutritional status, and cooking fuel. Interestingly, household cooking fuel was found to be the most influential variable related to AOM in primary school. It supported the previous study which found that the exposure of children to environmental wood, charcoal, and tobacco smoke is associated with otitis media in childhood. 13 This research was conducted in 6 regions in the Banyumas Regency which consisted of urban and rural areas. Most households use wood fuel and charcoal predominantly in rural areas, and this is related to economic factors. Exposure to smoke from fuel in children is possible even higher when mothers carry their children while cooking. The findings from studies of wood smoke exposure and increased risk of OM in children are consistent with the toxicological effects of wood smoke on lung epithelial cells. An experimental study also found that constituents of wood smoke increase epithelial cell oxidative stress. 14 Increased exposure to cooking fires multiplies the risk of catching respiratory diseases by four and, perhaps, this should be considered more specifically in developed or underdeveloped rural communities. Particles produced by indoor cooking with biomass fuels have been shown to surpass those produced by two-pack-perday smokers by almost 20 times. 15 Information on the risk factors for the use of firewood in cooking in Indonesia, also in the study area, is still limited in the community, so no preventive measures have been taken. The results of this study may be influenced by the habitual factors of the population in Indonesia, especially in rural areas who still use firewood for cooking. Of course, this result differs from the risk factors found in other countries especially in more developed European countries. Previous research in five East European countries has shown that childcare and allergy history are connected to the occurrence of AOM. 16 While other studies across Western countries mention several variables such as the number of siblings, smoking, breastfeeding, birth weight, and socioeconomic status. 17 The household cooking fuel factor in this study may be linked to air pollution in other countries. This confirms that the risk factors for a disease can be linked to the habits of life and the local culture of a specific region. The identification of these particular risk factors is essential for the implementation of an effective prevention program.
In this study, we also found that nutritional status correlated with the incidence of AOM. The poor nutritional status frequently occurs in developing countries and reflects the low economic status of their families. This condition could increase the risk of having inflammatory ear disease. 18 Previous studies revealed the evidence of low zinc, iron, vitamin A and vitamin D levels are associated with AOM.19,20 However, the limitation of this study we measure the nutritional status based on anthropometry by measuring body weight divided by the age of the respondent. Further investigation of specific macro or micronutrients would be beneficial.
A family history of ear infection history is also correlated with AOM incidence in this study. There is insufficient and contradictory proof of the impact of positive family history on AOM. 21 It is a much-debated matter whether this fact has a genetic basis or an environmental one, and both factors are likely linked. Several previous studies have demonstrated that genetic factors are significantly associated with OM. The association of some relevant genes to OM including several interleukin (IL) genes, mucin genes, TLR4, FBXO11, TNFα also discovered.22,23 In addition to genetic factors, this correlation of family history is also possible because they live in the same house environment conditions so that they have the same risk factors associated with AOM.
This study emphasizes the risk of using firewood in the household, low nutritional status, and a family history of ear infections with an increased risk of otitis media. Therefore, it is necessary to educate the community to avoid exposing their children to environmental hazards. Improving nutritional status for children is also important to prevent ear infections. Health institutions also need to educate the public about otitis media and how to prevent this disease. One of the drawbacks of this research is that the assessment of AOM cases is carried out only by otoscopy without audiometry and tympanometry examinations. This examination by otoscopy is not an objective examination so that the sensitivity is not good enough to assess whether there is an effusion (fluid) behind the tympanic membrane. Future research using improved audiometry and tympanometry investigations will be good to improve the quality of the study.
Footnotes
Acknowledgments
We acknowledge the Ministry of Research and Technology, Indonesia No 176/SP2H/AMD/LT/DPRM/2020 for the funding. We would like to thank students of the public health department, students of the biology department and co-assistant doctors, faculty of Medicine Jenderal Soedirman University who have assisted in conducting research and data collection. We also thank the Banyumas District Health Office and the Education Office for their assistance during this research.