
Abstract
Background
To date, no instrument in Portugal has evaluated the attitudes of the population about advance care directives. This paper describes the development and testing of the General Public's Attitudes Toward Advance Care Directives (GPATACD) Scale.
Design and methods
Methodological study. The development of the instrument was based on a literature review, updated in 2018. Face and content validity were verified by an expert panel and piloted among six participants. Data were collected in an online survey of 1024 Portuguese adults. The obtained data were analyzed using Varimax rotation, while the reliability was evaluated by calculating Cronbach's alpha.
Results
The scale achieves good Item-Content Validity Index (I-CVI) values, between 0.89 and 1.00, and scale-CVI values of 0.91. A principal component analysis generated four dimensions with 26 items as a final scale, with overall Cronbach's alpha of 0.848.
Conclusions
The findings demonstrate that the scale is valid and reliable as a vehicle for assessment of the general public's attitudes toward advance care directives.
Introduction
Significance for public health
Public education to disseminate the concept of ACD is needed to raise its awareness. Being asked to complete ACD and receiving information about ACD were found to predict ACD completion.7 What is clear, however, is that passing out information in the form of booklets and asking people if they have ACD is not sufficient to provide the depth of information the population needs to make decisions.33 Nurses are proven patient advocates and have communication skills ideal for ACD education. They encourage people to think unthinkable things, facilitate ACD discussions and reflection upon decisions, and help appoint surrogates. These strategies can be further developed with training programs providing opportunities to practice specific communication skills through role-play with the use of appropriate decision aids. The involvement of health professionals, patients, providers, and community stakeholders might also be required to design an efficient caregiving system for delivering ACD and EOL care.
One of man's greatest challenges has been to prolong life and postpone the moment of death. Advances in medicine and technology, as well as the entire health-related industry, have greatly contributed to a worldwide increase in average life expectancy. 1 This evolution has created a new health paradigm, as well as the need to care for people with chronic illness, situations that are sometimes accompanied by great suffering. Concomitantly, individualism emerges, where a person's rights and freedoms are recognized in defense of the principle of the user's self-determination.
Consequently, this brings about a dilemma in the area of health between prolonging life or allowing natural death to occur. If these technological advances have given life many gains over death, it is also no less true that often too much is invested in what cannot be cured. 2 End-Of-Life (EOL) has been the subject of great reflection in recent decades, particularly in recent years. The main topics of discussion are a person's dignity at the time of death and the increasing autonomy in their right to life and death. 3
Europe remains in a turmoil regarding euthanasia and medically assisted death. In countries where these practices are not legalized, namely in Portugal, strategies have been created that allow the person to have an EOL with dignity. Examples of these strategies include a palliative care network and advanced care planning.
In Portugal, according to the Basic Law of Palliative Care (Law No. 52/2012 of 5 September), the national palliative care network tries to provide care aimed at improving the quality of life of the sick person and their family members, relieving and preventing suffering in EOL. 4 According to Meeussen et al., 5 one of the crucial aspects in EOL care is congruence between the quality of care provided and the patient's wishes, namely in situations where the person cannot make a decision and his/her preferences are unknown, thereby making it difficult to deliver quality care. One way of managing the future is the Advance Care Directive (ACD), a legal declaration of a person's will regarding EOL that guarantees compliance with their rights when they are unable to give informed, free and informed consent. 6 Decisions taken by the patient imply consent with prior information and clarification, which is of greater relevance before a person becomes incompetent due to illness or age and is unable to consent, dissent or refuse medical treatment or intervention. It attempts to ensure that patients receive the treatment they want, promoting patient-centered care. This greater focus on a patient's autonomy and right to self-determination was concomitant with a decline in or abandonment of medical paternalism. 4
The Portuguese Living Will Law has a triple objective: i) to establish the ACD's legal regime; ii) to regulate the appointment of the healthcare proxy; and iii) to create the former register of the ACD in the Living Will National Registry (RENTEV). 4 According to the Law, any citizen over eighteen years old and duly capable may declare in advance, and in a clear, conscious and informed manner, his or her wishes regarding medical care, by preparing an advance directive. These directives may take the form of a living will and a health care power of attorney.
Some researchers have explored reasons why ACD discussions are not initiated. Early studies showed that lack of knowledge and inaccessibility to ACD documents were the primary reasons. 7 Efforts to improve both education and accessibility have failed to increase the number of ACD discussions initiated. Only a few studies have explored the reasons why the general public perceives ACDs as either positive or negative, and the effect those perceptions have on the decision to initiate ACD discussion. In the study conducted by Chung et al. 8 about the knowledge, attitudes and preferences of the population of Hong Kong in relation to ACDs, a low percentage of the population reported having heard about them. However, after informing people about ACDs, the majority agreed that they were a good approach to declare their preferences before they became mentally incapable and more than half of the population who participated in the study stated that they would be willing to make an ACD. Age, sex, terminal illness diagnosis and prior knowledge showed a statistically significant correlation with the desire to perform an ACD, while the remaining variables, such as other sociodemographic factors (e.g. education, religion beliefs, marital status, type of housing) and health status, did not show a significant relationship. In another study conducted by Gao et al. 9 , perceptions about EOL care, and knowledge and realization of ACDs were investigated among Chinese and Americans living in Phoenix. This study revealed the population had scarce awareness and knowledge about ACDs. In contrast, in an Italian nationwide population-based survey, 70.1% of respondents declared they had heard about the law on informed consent and ACDs. Respondents were asked to express their overall opinion on the law's utility and importance: 88% declared that the law was quite or very important and 76% had a positive attitude toward making/registering advance directives. 10
Several studies have also evidenced the positive outcomes and effectiveness of ACDs. Some of the benefits identified included less aggressive medical care 11 and better quality of life near death, 12 with higher satisfaction and a reduction of psychological distress of both patients and families. 13 While an estimated 35% of adults in the US have done an ACD 14 , in Portugal completion rates are approximately 1%. 15 A study performed in 2014, by the Catholic University in partnership with the Palliative Care Association, found that 78% of Portuguese adults did not yet know what a living will is. 16 Among the 22% who knew what a living will is, only 50.4% Portuguese knew what to do and where to go in order to execute an ACD, and only 1.4% actually had formally executed one. 16 To date, no instrument in Portugal has evaluated the attitudes of the general population about ACDs. The existing instruments have been applied at specific groups of the population, such as health professionals17-19 and students. 20 Thus, the aim of our study is to develop and validate a questionnaire that explores the attitudes of the general population toward ACD, so that in future studies it may be used to evaluate public attitudes and experiences about ACD.
Design and Methods
Study design
The study adopted a quantitative approach and consisted of two phases of instrument development21,22, namely: i) construction of the initial instrument using two steps and ii) a psychometric evaluation phase, with one step.
Phase I: Development of a questionnaire
Step 1. To generate an item pool
An inductive approach was applied to generate items, as recommended when there are few available scales.21,22 The researchers developed a questionnaire guided by Colton and Covert's 21 guidelines. A literature search was conducted from March to April 2018, using key words such as “advance care planning”, “advance care directives”, “end-of-life”, “decision making”, in three databases: EBSCOhost, CINAHL, PubMed. Additional searches were also made in Google scholar, in relevant grey literature and by manually studying reference lists of identified articles. The literature search included 19 articles written in English, screened and reviewed by LG and AQ. In the end, eight articles were deemed relevant. Based on evidence and inspired by available instruments,23,24 the authors developed the General Public's Attitudes Toward Advance Care Directives (GPATACD) scale with 30 items with a 5-point Likert-type scale, where the participants mark their level of agreement between 1 (strongly disagree) and 5 (strongly agree).
The scale measures the extent of one's positive or negative views about decisions regarding ACD, specifically personal values and wishes related to EOL care, impact of ACD on the individual and family, and perceptions about EOL decision-making.
Several questions were phrased negatively to prevent “response acquiescence”, defined as the tendency to agree rather than disagree. Items 1; 2; 4; 5; 6; 9; 10; 12; 15; 16; 19 and 22 were inverted in the decreasing direction (lower values, more positive attitudes). Aside from the GPATACD scale, the research instrument included questions on basic socio-demographic information, such as age, gender, level of education, and professional status.
Step 2. Face and content validity
Following the literature review, the generated items and scaling responses were tested using a standard pilot study with six individuals considered experts in the health field (1 physician specialized in Public Health and 1 nurse trained in the field of bioethics), in the field of building measurement instruments (2 professors), and two Portuguese language experts. The time taken to complete the questionnaire ranged from 5-10 min. Their participation helped check the facial and content validity, 21 contributing to its improvement. The Content Validity Index (CVI) was calculated for all individual items (I-CVI) and the overall scale (S-CVI). Each item was reviewed, and the relevance and appropriateness of each item was discussed. The experts’ evaluation used the 4-point rating scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant and 4 = very relevant). Higher score means better items. In two open questions, experts were also asked to suggest revisions and items that should be included. The feedback resulted in minor revisions of eight items (changes in word order and replacement of one word with a more neutral word). For each item, I-CVI was computed as the number of experts giving a rating of three or four, divided by the total number of experts. For example, an item rated three or four by five out of six experts has an I-CVI of 0.80. The I-CVI should be 1.00 in case of five or fewer judges and in case of six or more judges; I-CVI should not be less than 0.78. The S-CVI was computed to ensure content validity of the overall scale. S-CVI (average) focuses on average item quality rather than average performance of the experts. The S-CVI should be at least 0.8 to reflect content validity. 25
Phase II: Evaluation of the psychometric properties
Sample and setting
We used convenience and snowballing sampling techniques, with a Portuguese general population aged 18 years or older who answered a questionnaire made available online through social media platforms (Facebook and emails) between March and May 2018. The study was first advertised by the IPLeiria Media and Communication Department using the institutional e-mail contacts of the workers and students and also published on the IPLeiria's Facebook page. We targeted potential participants by asking those who completed the survey to forward the announcement link to their friends and/or colleagues by e-mail. For practical reasons, the authors also sent the survey by email to their network contacts, mainly health care professionals. The study involved only those participants who had access to the internet.
The necessary sample size to perform factor analysis was calculated based on a rule of thumb of 10 participants per item in the GPATACD. 26 Our instrument included 30 items that could be validated, hence the number of participants required was 30*10 = 300.
Data analysis
All analyses were performed using the Statistical Package for Social Sciences version 25.0 (IBM Crop., Armonk, NY, USA). Descriptive statistics was used to summarize the demographic data and responses.
Reliability analysis involved calculating Cronbach's α to assess the internal consistency of the 30 items measured on a Likert-like scale. Cronbach alpha values greater than 0.9 suggest redundancy of some items, values between 0.70-0.90 imply adequate internal consistency, values between 0.50-0.69 indicate poor internal consistency, and values below 0.50 indicate unacceptable internal consistency. Corrected item-total correlations were then used to identify items that did not agree well with other items in the questionnaire. Corrected item-total correlation values should exceed 0.2 to be considered as acceptable. 27
Exploratory factor analysis was used as a data reduction technique, to investigate the dimensionality of the GPATACD scale. In the factor analysis, we noted the number of factors and factor loadings, the inter-item correlations and Keiser-Meir-Olkin (KMO) values.
Results
Demographic characteristics of sample
The sample included 1024 individuals who agreed to participate in the study and who met the previously established criteria. Initially, 1030 people had access to the questionnaire through social networks, of which only 0.58% (n=6) refused to participate in the study.
The mean age of the sample was 40.28 (±11.41) years (range 18–78 years) corresponding to an adult population of working age (Table 1). Most of the participants were female (79.69%) and had finished higher education (79.89%), and 61.62% were married or living together. Of all participants, 71.09% reported they had health care work experience.
Demographic characteristics (n=1024).

Content validity
The I-CVI for all items ranged from 0.89 to 1. The overall SCVI for the 30-item scale was 0.91, which indicated high content validity of the items for the construct of attitudes toward ACD.
Reliability
In order to assess the reliability of this scale, Cronbach's Alpha Coefficient was calculated for all the instrument's items, as well as the scale after excluding each item individually. After successive rounds, items 3, 21, 23 and 24 were removed (corrected item-total correlations were low) as they impaired the instrument's internal consistency, leaving the instrument with a total of 26 items. Table 2 shows the total Cronbach's Alpha of 0.848, where no item impairs this value. The validity of each item on the scale can be attested through its correlation with the total scale. According to Streiner and Norman, 22 this is a good indicator of the total instrument, since almost all items showed values greater than 0.2. Items 5 and 6 revealed lower correlation values, respectively 0.193 and 0.168, but these items were retained as they were deemed to represent theoretically important aspects of the construct (attitudes toward ACD). 22
Mean, standard deviation, coefficient of item-total correlation, and alpha Cronbach if the item is excluded of the General Public's Attitudes Toward Advance Care Directives (GPATACD) scale.

EOL, end of life; ACD, advance care directive; *reversed items.
Validity
Regarding the construct validity, we used factor analysis (analysis of the main components of correlations between variables), as it allows us to synthesize relationships between items of an instrument into factors. 27 Specifically, to inspect the validity of the GPATACD scale, we conducted exploratory factor analysis using the condensation method in main components and according to the Kaiser criterion (latent roots equal to or greater than one), thus obtaining a scale composed of four factors: F1 - Autonomy and dignity of the person at the EOL (7 items); F2 - EOL decisionmaking (8 items); F3 - Application of ACD (6 items); F4 - Perception of the EOL (5 items).
These four factors, after using the Varimax rotation method, explained 50.06% of the total variance (Table 3). For the organization of each item in these factors, we considered three criteria: greater saturation between four factors; saturation between the four factors with a minimum difference of 0.100; and theoretical interpretability of each item. The data indicated a Bartlett's Sphericity Test value of 8683.057 (p<0.0001), with a Kaiser-Mayer-Olkin value (0.856) close to one. These values represent a satisfactory factor analysis to obtain a scale composed of 26 items and divided into four factors.
Factorial loading for four extracted factors after varimax rotation (n=1024).
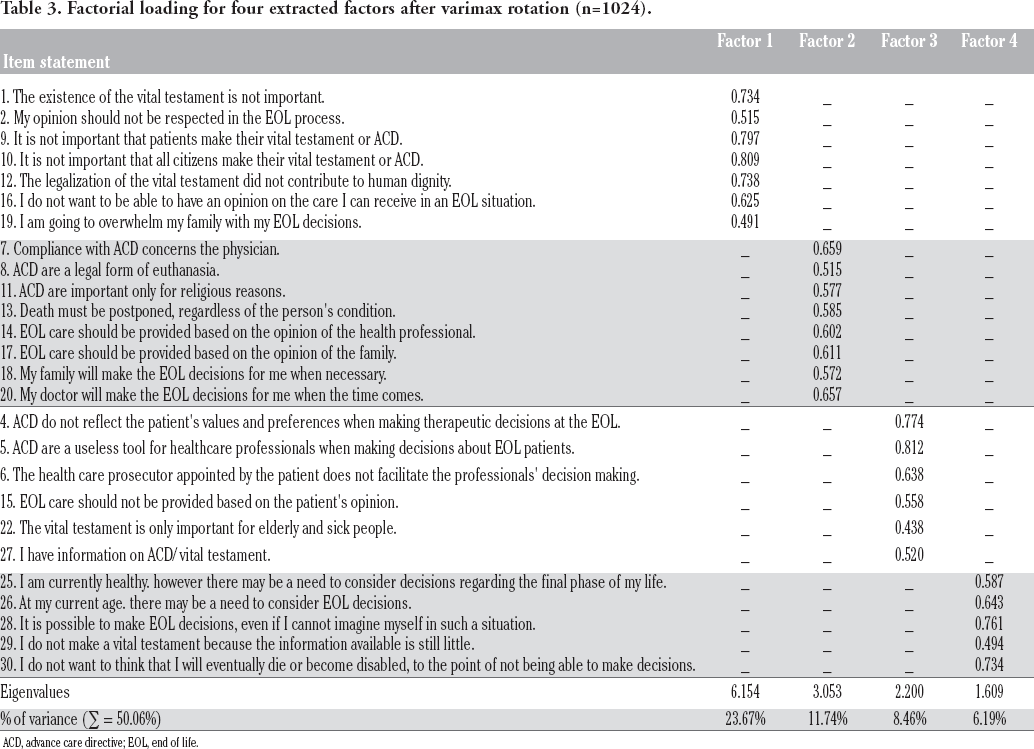
ACD, advance care directive; EOL, end of life.
Publics’ Attitudes toward ACD
To examine the general public's attitudes toward ACD the total scores on the GPATACD were analyzed using mean scores and standard deviation (see Table 2). A global average of 1.922 ± 0.440 was obtained (values closer to one are more positive and closer to five are more negative), that is, the majority of participants expressed their level of agreement in the positive sense of attitudes toward ACD.
Discussion
The aim of the study was to develop a scale to measure the general public's attitudes toward ACD and evaluate its psychometric properties. The analyses show that the GPATACD scale possesses good psychometric qualities and can contribute to understand how the Portuguese population perceives ACD.
Cronbach's alpha was used to estimate reliability of the total scale. The overall Cronbach's alpha of the GPATACD scale was 0.848, considered satisfactory for measuring instruments. 28
To enhance the validity of the study, content validity was done to ensure the congruence between the target of the research and the data collection tool. 29 The content validity of GPATACD scale was explored based on a literature review and judgments of six experts, resulting in 30 items. A CVI on the relevancy of dimensions to concepts indicated a high degree of agreement among experts, which meets an acceptable CVI of 0.80 or greater. 25
Exploratory Factor Analysis was used to explain the maximum portion of variance in the original variable and drive the minimum number of its components. The assumptions of normality, factorability, and sample size had been tested prior to data analysis, and showed acceptable assumptions for factor analysis. The four-factor structure identified in the factor analysis showed that the GPATACD scale can capture various reactions to ACD, which implies the population has opinions and can assess these issues. Although studies of public awareness about ACD are rare in the empirical literature, our findings indicate such studies are feasible.
According to our results, the participants seemed moderately knowledgeable about EOL issues. Since most participants were HCPs, they tended to rate themselves highly in terms of their knowledge and preparedness to engage with ACD, although this was not unanimous. 30 In this regard, Hamilton 31 implied that practitioners may be uncomfortable with having ACD conversations for fear that patients could potentially endure undue anguish. Research shows that care providers miss opportunities to start a discussion about advanced care planning in part when they lack skills to initiate a conversation or prefer not to engage in discussions when seriously ill patients are feeling well. 32
In contrast, public awareness of the concept of ACD and EOL issues remains insufficient for widespread, effective and appropriate EOL care to be accepted as the norm. 33 According to the studies by Andrès-Pretel et al., 34 Chan et al., 7 Aguilar-Sanches et al., 35 most participants have favorable/ positive attitudes toward ACD. Moreover, the public has reported wanting more information about ACD, and discussion around dying should be addressed. Education on EOL care represents the foundation to disseminate knowledge in the general population.
Methodological considerations
The strengths of this study include the large sample size and the use of a culturally sensitive, valid, and reliable questionnaire. The GPATACD scale relies on a robust methodology, integrating empirical findings with perspectives from theory and practice. We believe this combination contributes to the scale's relevance and usefulness for future studies, which can contribute to understand attitudes and awareness about ACD. A valid self-assessment scale enables studies with larger populations, where various perspectives of ACD can be studied and compared over time. Despite the GPATACD scale's promising psychometric properties, its overall validity should be interpreted in light of potential methodological weaknesses, including the use of convenience sampling composed mainly of subjects with professional background related to healthcare. We were not able to perform discriminative validity (in a population that is generally unaware of ACD) and convergent validity (as no other ACD have been validated in Portugal).
The scale's psychometric properties can still be improved, and additional analyses need be conducted, such as a test-retest reliability analysis and a Confirmatory Factor Analysis based on supplementary data to confirm the scale's factor structure.
Comparative research or experimental research designs need to investigate whether family centered, community based, and ethnically appropriate approaches to education result in different levels of ACD completion. Combined with the qualitative data, these approaches would provide the information needed to suggest any need for policy revision. A qualitative research design would be beneficial in exploring those factors related to refusal to complete ACD. As the topic is quite sensitive and people may be hesitant to speak about death, and as their distrust of the system, their religious beliefs and other personal factors may contribute to decision making, 36 the qualitative design should plan for approaches to increase trust between researcher and respondent.
Conclusions
The GPATACD was a valid and reliable instrument to assess the general public's awareness and attitude toward ACD. We intend to apply the GPATACD with a larger cohort in Portugal. This data can provide government stakeholders with the information required to implement campaigns promoting literacy about ACD in Portugal.
Footnotes
Acknowledgements
We acknowledge all the volunteers who participated in the online survey to make this study possible.