
Abstract
Background
Inadequate funding for vaginal delivery can be one of the barriers to reducing the maternal mortality rate. It could be therefore critical to compare the vaginal delivery cost between total hospital cost and INA-CBGs cost in national health insurance.
Methods
This was a retrospective cross-sectional study conducted from October to December 2019 in Universitas Airlangga Academic Hospital. It collected data on primary diagnosis, length of stay, total hospital cost, INA-CBGs cost, and counted disparity. The data analyzed statistically using t-test independent sample (or Mann-Whitney test).
Results
A total of 149 vaginal delivery claims were found, with the majority having a level II severity (79.87%) and moderate preeclampsia as a primary diagnosis (20.1%). There was a significant disparity in higher total hospital costs compared with government INA-CBGs costs (Rp. 9,238,022.09±1,265,801.88 vs 1,881,521.48±12,830.15; p<0.001). There was also an increase of LOS (p<0.001), total hospital cost (p<0.001), and cost disparity (p<0.01) in a higher severity level of vaginal delivery.
Conclusion
Vaginal delivery costs in INA-CBGs scheme are underneath the actuarial value. There was also an increase in total hospital costs and a more significant disparity in the higher severity levels of vaginal delivery.
Significance for public health
The inadequate availability of funds for childbirth can be one of the administrative constraints that are directly or indirectly related to efforts to reduce maternal mortality. This study will give references to government, stakeholder, and researchers to highlight the urgency of vaginal delivery cost in a country.
Introduction
One of the most significant problems in the Indonesian health sector is the implementation of the national health insurance system (JKN). This aims to achieve universal health insurance so that all citizens benefit from health services and protection in meeting primary health needs. As one of the systems declared by the state with law number 40/2004, this system has been running since 2014. 1 One of the fundamental changes in the payment system to hospitals is from a retrospective payment (service fee) model to a prospective payment system or bundling known as Indonesia Case Base Groups (INA-CBGs).2,3 The number of claims or bundling is significant to be adjusted with actuarial value in order to ensure adequate quality of health services.
In maternal health services, JKN influences the management of maternal patient management in health facilities. Another important consideration is the situation of the Maternal Mortality Rate (MMR) in Indonesia, which is still high, which is around 305/100,000 live births. 4 Meanwhile, the World Health Organization (WHO) has set a global target for maternal mortality, which is no more than 70/100,000 live births by 2030. 5 JKN is expected to support the elimination of causes of maternal death known as “three delays”. This consists of: delays in recognizing signs of danger, delays in achieving proper health care and delays in receiving adequate care remain primary considerations for improvement.6,7
The insufficient availability of funds for delivery can be one of the administrative obstacles that are directly or indirectly related to efforts to reduce maternal mortality. From the above background, this study aims to compare the cost of claims for INACBGs in hospitals with the actual cost of vaginal delivery as the largest proportion of delivery mode nationally (81.5%). 8 At the same time, the adequacy of this financing is predicted to be closely related to the quality of delivery services in Indonesia by using national health insurance.
Methods
The study used a cross-sectional design by utilizing data on total hospital costs and INA-CBGs claims. It was taken from October to December 2019 at Airlangga University Academic Hospital (RSUA), Surabaya East Java Indonesia.
All claims data related to vaginal delivery were selected and included in our study. Additionally, to eliminate bias from the study, the authors included only single pregnancies because of the more significant costs associated with caring for more than one baby if the mother had multiple pregnancies. We also excluded cases of severe preterm preeclampsia that required conservative care before delivery to prolong the period of hospitalization and increase the total cost. In the INA-CBGs classification, delivery is included in the Case-Mix Main Groups (CMG): O (Deliveries group). Then in the current INA-CBG grouping, vaginal delivery whose complexity is divided into vaginal delivery (CMG: O-6-13), vaginal delivery with procedures other than sterilization/dilation/ and curettage (CMG: O-6-12), and vaginal delivery discharge with sterilization/dilation/ and curettage (CMG: O-6-11). All severity levels (level I to level III) for each type of vaginal delivery group were included in this study and will be stratified for analysis.
Data collected from each claim case includes the primary diagnosis, length of stay, total hospital cost, INA-CBGs cost and counted cost disparity (INA-CBGs cost - total hospital cost) and will be grouped into severity levels in the vaginal delivery of INA-CBGs group. The rates of INA-CBGs taken here are adjusted to the classification of Airlangga University Academic Hospital, which is inpatient cases in Regional 1 area (East Java), government, and class B Hospitals which has been regulated based on the minister of health regulation number 64/2016. 9 The categorical variables are shown in terms of frequency and percentage (%), while continuous variables were reported using the mean ± standard deviance (SD). The T-Test independent sample (or Mann-Whitney test) was used to compare the difference in the continuous variables between groups. Paired samples t-test or Wilcoxon signed-rank test were also used to compare cost disparity in all samples. All statistical analyses were performed using the SPSS software package (IBM Corp., Armonk NY, USA) version 24.0. A p-value of <0.05 was taken to signify statistical significance.
Results
Primary diagnosis, severity levels, and total claims of vaginal delivery
For three months, we found a total of 149 vaginal delivery claims were included in the study. The majority of cases had level II severity based on INA-CBGs group (119 cases, 79.87%). The general primary diagnosis for vaginal delivery at the Airlangga University Academic Hospital includes a diagnosis of moderate pre-eclampsia (30 cases, 20.1%), the prolonged first stage of labour (24 cases, 16.1%), premature rupture of membrane, and excessive weight gain in pregnancy respectively 21 cases (14.1%). For severity level I, in vaginal delivery, most cases that came to the hospital were caused by the prolonged first stage of labour (23/30 cases, 76.7%). Meanwhile, at severity level II, the highest diagnosis was moderate pre-eclampsia (30/119 cases, 25.2%). The data distribution of the primary diagnosis is reported in Figure 1.
INA-CBGs claim for vaginal delivery
For the INA-CBG group in all cases of vaginal delivery included in this study, only two types of complexity were found: vaginal delivery (CMG: O-6-13) and vaginal delivery other than sterilization/ dilatation/and curettage procedures (CMG: O-6-12) group with only two levels of severity. Table 1 illustrated the claims of INA-CBGs for each group at Airlangga University Academic Hospital (Regional 1 area, government, and class B Hospitals), based on the regulation of the Indonesian Ministry of Health. 7
Comparison of total hospital costs and INA-CBGs cost in vaginal delivery
By comparing the bundling price for vaginal delivery that has been determined by the government in the INA-CBGs, it has been found that the total hospital cost is significantly greater than the price determined by the government through the INA-CBGs (p<0.001) (Table 2).
Analysis of severity level in vaginal delivery
There was also a significant increase in the length of the stay (LOS) (p<0.001), total hospital cost (p<0.001) and cost disparity between INA-CBGs determined by the government and total hospital costs (p<0.01) in this study (Table 3).
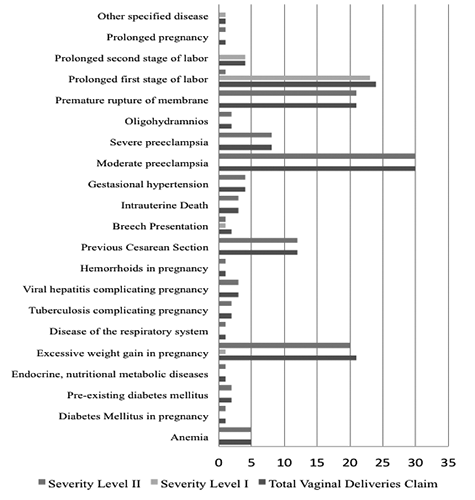
Distribution of primary diagnosis, severity levels, and total claims of vaginal delivery.
INA-CBGs claim for vaginal delivery.

Discussion
The implementation of the National Health Insurance (JKN) in Indonesia from 2014 has changed various financing systems in health facilities. In terms of JKN's participants or users, this program provides an advantage because access to health facilities can be obtained at an affordable price of about Rp. 42,000 (USD 2.83) per month for the lowest class according to the latest presidential regulation.10,11 It can be shown through an increased number of participants. It started from 133,423,653 residents in 2014 to 224,149,019 residents (83.86% of the total population in Indonesia) in 2019 who are registered as JKN's participants. Also, the number of the referred hospital, which collaborates with this program rise every year (46.28% from 2014 to 2019). 12
This study focused on national health insurance in vaginal delivery services. The results of this study showed that the main diagnosis of vaginal delivery in Airlangga University Academic Hospital is predominantly due to preeclampsia, the primary diagnosis for both overall and severity level 2 vaginal delivery is moderate preeclampsia. Meanwhile, dystocia disorders in the prolonged first stage of labour dominate vaginal delivery with severity level 1. Several reports in Indonesia showed a high prevalence of preeclampsia up to around 12.7 compared to reports in developed countries such as in the US (8.34%). 13 This is in line with Wardhana's findings study, which showed a very high prevalence of preeclampsia, with up to 1106 cases (21%) in 2 years in a referral teaching hospital in Surabaya. 14 Indeed, this affects preeclampsia referrals where labour and delivery cannot be done in primary healthcare, which is not adequate resources to handle cases.11,15
Delivery services are essential health services in human life, although specific diseases do not always follow them and often result in significant health financing. 14 Delivery services also had the highest cost of all episodes of maternal care.16,17 The main issue of this study is that the government's claim for vaginal delivery through the INA-CBGs group is significantly lower than the total costs incurred by the hospital. The higher the severity of vaginal delivery, the higher the disparity and increase in the length of stay (LOS) so that the hospital financing package will increase. There has never been a study comparing the costs of vaginal delivery, particularly in Indonesia. However, this study shows low claims of funding from the Indonesian government for vaginal delivery. Claims for vaginal delivery cost with the lowest complexity based on the hospital classification where the study was conducted were Rp. 1,626,200 or if converted around USD 109.49. 9
In other hands, some observations from the Independent Hospital Pricing Authority report in Australia show that a single vaginal delivery episode with DRG O60C - ‘vaginal delivery, minor complexity’ has a higher claim of about 34 times (AUD 4,777 or USD 3,422) than vaginal delivery cost claims in Indonesia.18,19 A report from the US also states that Medicaid financing using a blended payment in Minnesota in 2009 gave a price of USD 3144 to 3528 USD. 20 Another study from Bellanger of 11 European countries, shows claims that vary widely different. For cases of vaginal delivery with one day LOS, the lowest DRG claim prices were found in Poland (479 Euros ∼ 561 USD) up to 2047 Euros ∼ 2343 USD in Sweden. The lowest price in the Polish area has a vaginal delivery payment rate of up to 5 times the INACBGs claim for vaginal delivery in Indonesia. 14
In addition, Nugraheni's report from the Ministry of the Health Republic of Indonesia shows the impact of the national health insurance program on a significant reduction in vaginal delivery cost. 21 As is well known, financial problems, particularly in poor people, will give harmful conditions for health status. 22 The high expense on health service costs will surely have an impact on the family's finances. 23 Nevertheless, on the one hand, health insurance must strive for high-quality health services for everyone not excluded. The low price of vaginal delivery claims needs to be a concerning issue. It is crucial to define a grouping algorithm as Diagnosis-Related Group (DRG), which we refer to as INA-CBGs, to have a fair performance comparison and hospital reimbursement. 24 The optimal design of the DRG system for labour cases is critical to ensure adequate performance comparisons and appropriate reimbursement for these causes of frequent hospitalizations. 14 The impact of low financing can certainly disrupt service quality and hospital cash flow, which needs to be further investigated.
Although the study did not investigate the correlation in Caesarean Section (CS) rate, low vaginal financing could also be associated with an increase in CS rate. The CS rate report from one of the referral hospitals in the territory of Indonesia also shows an SC rate of up to 50.2% for patients using the national health insurance program (JKN). 25 Furthermore, several comprehensive national reports from BPJS Kesehatan also state that the CS rate rose around 57% in 2017.8,26,27 Research shows that CS rates above 10% are not associated with a reduction in maternal and infant mortality. However, the WHO has never recommended a specific rate in a country or hospital because each region has different particular situations. FIGO (The International Federation of Gynecology and Obstetrics) gives one of the recommendations to reduce unnecessary CS, including similarity cost both CS and vaginal delivery for medical workers.28-30 Indeed, this is difficult to do in Indonesia, where INA-CBGs financing claims for a vaginal delivery are still deficient. The limitation of this study is that the investigation was conducted only in one hospital. We need more hospitals to compare hospital cost rates, even though in general if we look at the claims of INA-CBGs from the government it is much lower than in other countries. Increasing vaginal delivery costs is a critical need to increase according to the actuarial level. So the financing scheme in the national health insurance system can support in providing high-quality maternal services and reduce maternal and infant mortality rates in Indonesia.
Comparison of total hospital costs and INA-CBGs cost in vaginal delivery.

Analysis of severity level in vaginal delivery.

Conclusion
The cost of vaginal delivery from the National Health Insurance System is below the actuarial value. There is a reasonably high disparity, where bundling financing from the Indonesian government in the form of INA-CBGs is lower than the total hospital costs. As the severity increases, the patient's LOS will be longer, followed by a higher total hospital cost and a more significant disparity in financing compared to the government's INACBGs package. So, from these findings it is assumed that the government can review policies and improve the system for the cost of services for vaginal delivery to improve the quality of maternal services, control the caesarean section rate, and reduce the maternal mortality rate.
Footnotes
Acknowledgements
We acknowledge all the Airlangga University
Academic Staff who participated in the data collection.