
Abstract
Objectives
Medication understanding is critical for patients who suffer from multiple chronic conditions in order to reduce medication error and is often associated with poor health outcomes and low adherence. This study aims to identify the gap of medication knowledge among multiple chronic condition patients in Bangladesh, in order to aid physicians and other healthcare providers in improving health literacy.
Methods
Individual interviews of a convenience sample of multiple chronic condition patients in Bangladesh were held where they were asked a number of questions for assessing medication related literacy.
Results
More than 26% patients failed to cite the brand name of all their prescribed medications while the rate of patients not knowing the generic names was far worse (88.1%). Nearly 1 out of every 4 patients did not know the purpose of all their medications and more than half of the participants (55%) did not know the strengths of their drugs. While knowledge about medication routes and regimen was satisfactory, awareness regarding risk factors of medicine was lowest of all. Only 1 out of every 4 patients had a habit of reading drug information leaflet. Patient's ability to correctly state the purpose of their medication seemed to be positively associated with age (p=0.004) and negatively associated with number of medicines taken (p=0.03).
Conclusions
Many patients demonstrated poor health literacy regarding medication. Routine review of medications from physician or health provider can significantly improve their health literacy, leading to better treatment outcome and medication adherence.
Significance for public health
Despite having a significant non-communicable disease burden, health literacy and medication understating among patients in Bangladesh is very low. Multimorbidity patients usually consume a high number of medications as part of their treatment, therefore understanding of their medications is critical to ensure no medication error occurs. Identifying the gap of medication knowledge is critical for physicians and other healthcare providers, so that they can be key source for improving health literacy. Our findings suggest sub optimal health literacy regarding medication among the study participants, which can lessen treatment adherence or lead to medication error. Strategies for improving medication understanding is urgently needed for multimorbidity patients, especially physicians and community pharmacists can actively be involved in increasing health literacy of their patients.
Introduction
Health literacy is defined as the extent of an individual's capacity to gather, interpret and understand basic health related knowledge and services in order to make good health decisions. 1 It is composed of knowledge and understanding of several key factors associated with the nation's healthcare system. 2 Poor health literacy have often been associated with patients’ inability to understand labels and health information, not being able to take their medication properly and overall substandard health status. 3 Patients with poor literacy levels comparatively experience greater difficulties in utilizing the healthcare system and have an overall lower health status. 4 Thus poorer health literacy level has often been linked to medication errors, misinterpreting physician's instructions and disease symptoms, low adherence to treatment, poor self-care attitude, overall worse healthcare output and frequent visits to hospital emergency departments.5-11 These problems can easily be aggravated in patients suffering from multiple chronic conditions because of the higher number of medications they usually take.
Multiple chronic conditions, often termed as multimorbidity, has increased dramatically over the past decade and nowadays is very common among adults and elderly who are receiving health care. 12 Patients with multiple chronic condition find it difficult to cope with the health care system as they usually consult more doctors and have significantly higher number of medical appointments than patients with only one disease. 13 Many such patients take multiple prescription drugs, sometimes in combination with self-administered OTC medications which increase the chances of drug-drug interaction and likely toxicity. 14 In prior studies conducted in impoverished population, it was observed that patients who are suffering from chronic conditions such as asthma, hypertension or diabetes and have low health literacy levels have overall lesser knowledge of their disease, poorer understanding of their treatment and prone to more errors in self-management skills compared to literate patients.15,16 Treatment of diseases have advanced in leaps and bounds over the last few years resulting in an overall better healthcare system, but at the price of even more complicated drug, diet and dosage regimens. 17 To improve the health status of multimorbidity patients, they have to be instructed appropriately and provided with sufficient knowledge and skills regarding dosage regimen, drug administration and monitoring. 18 Suboptimal medication knowledge have been observed in multiple studies carried out for determining patients’ knowledge and understanding of their prescribed drugs, where they failed to correctly answer their medication related questions such as drug name, dosage, adverse effects, etc.19-23
Bangladesh, a densely populated developing country of South East Asia, has a significant non-communicable disease (NCD) burden, being accountable for 67% of its mortality rate. 24 The country has an extreme shortage of health care workers, most of whom are centered around the urban areas, and studies conducted in rural villages indicate an alarmingly low level of health literacy. 25 Investigation of health literacy in Bangladesh has so far been inadequate, and this study aims to evaluate the medication related knowledge of Bangladeshi patients suffering from multiple chronic conditions and understand the relation between socio demographics and overall health literacy.
Methods
Study design
A cross sectional qualitative study was conducted from January to March 2020 by means of structured individual interviews of multiple chronic disease affected patients across the different regions of Bangladesh.
Interview setting and participants
Interviews were taken in participants’ home by pharmacy undergraduates of University of Asia Pacific, Bangladesh. Prior to conducting the study, the interviewers were thoroughly trained about the interview process and questionnaire by the principal researcher. To maintain consistency of interviews, there were multiple simulated interviews taken by the principal researcher in front of the interviewer so that they could understand how to ask the questions in easy to understand language and also be prepared for any queries raised by the participants. The interview questionnaire was pilot tested before on a number of people by the principal researcher to ensure the questions were valid and clear to understand. The participants were selected by the individual interviewer and in most cases were their close relatives or family members. This strengthened the level of trust and understanding between the participant and the interviewer and ensured more reliable answers. Participants were eligible for the study if they were Bangladeshi, aged 16 years or older, having multiple chronic conditions and were at least receiving two medications for their conditions. Chronic condition of the patients included in the study were classified into 7 classes as defined by the ICD-9-CM (International Classification of Diseases, 9th Revision, Clinical Modification) diagnoses codes with some slight modifications. 26 The interview was taken in English or Bangla, whichever language the participant was more comfortable in. Exclusion criteria included severe cognitive disorders and inability to communicate clearly with the interviewer.
Measurement
A guideline for conducting the interviews was developed based on a prior medication related health literacy survey conducted in the U.S. 19 Participants were asked to bring forth all their currently prescribed medications. The interviewer would then collect all the medicines and ask the participant to name their prescribed medications (brand names) one by one from memory. In the event of the participant failing to answer the name of their medications, the interviewer would begin by placing the medication in front of the participant. After that 10 questions were asked to the participants on each of their prescribed medicines. The questions were designed to test the level of information that the participants had on the medicines they were taking. They were asked to cite the name (both brand and generic), strength, administration route, dosage regimen of the medicine; which disease condition they were taking the medicine for, risk of any potential side effect or risks that may arise due to overdose, knowledge of any alternate brands and whether or not they ever read the drug information leaflet of their medications.
Data analysis
The data collected from the interviews were assigned a unique code for anonymity and analyzed using IBM SPSS Statistics package for Windows, ver. 25.0 (Armonk, NY, USA). The entered data was checked for entry errors and normality. Demographic characteristics of the participants were analyzed using descriptive statistics. Continuous variables were expressed as means and standard deviations, whereas categorical variables were expressed as frequencies. The association between categorical variables such as gender, education, occupation, language proficiency etc. were evaluated using Pearson's Chi Square test or the Fisher's exact test in case the expected cell count was less than 5. Multivariate logistic regression analysis was performed to analyze the factors associated to patients being able to name all their drugs and patients being able to state the purpose of their medications.
Ethics approval
The Ethical Review Committee, Department of Pharmacy, University of Asia Pacific granted their approval to conduct this study (Ref: UAP/Pharm_ETA: 05_12/2019).
Consent and confidentiality
Written consent was collected from each participant before their interview. The participants were informed about the purpose of the study and had been assured that all personal and medical information will be treated as confidential. Audio recordings were kept of each interview using the mobile phone of the interviewer, with the consent of the participant.
Patient and public involvement
Patients were informed about the nature of the work and what outcome we wish to achieve before their interview. After the interview was conducted, all interviewer reviewed the answers with the participant, informing the answers they did not know and corrected them of their errors.
Results
Patients’ socio-demographic characteristics
A total of 250 eligible participants were interviewed out of which 213 responses were considered valid for the analyses (85% response rate). Among the 37 interviews not analyzed, 14 of them were excluded as the participants were taking multiple medications for a single chronic condition only, 12 of them were excluded because of inaudible or missing audio recording and 11 were excluded due to insufficient demographic information. Table 1 shows that study participants had nearly equal gender distribution with a slightly higher female count (56%) and a mean age of 48.5 years old (SD ±13.5 years, range 16-90 years old). Participants had different levels of education ranging from people who were illiterate or had less than 10 years of schooling (14.7%) to university graduates (45.4%). Most of the participants could read English (86.6%), lived in urban areas of the country (75.6%) and had different occupational statuses such as employed (43.3%), unemployed (43.3%), retired (11.1%) or others (2.3%).
Patients’ health related factors
Table 1 shows the different health related factors of the study participants which includes the type of chronic conditions they are suffering, their medication dosing strategies and level of satisfaction over communication with healthcare provider. The most prevalent chronic condition seen among the participants were hypertension and diabetes. For these conditions, patients were taking 3.56 (SD ± 1.46) number of medicines on an average. Majority of the participants were able to take the medications by themselves; some without any particular strategies (31.6%), some used pill boxes (27.4%) while some associated the administration of their medication with their regular routine (35.3%). Around 5.6% participants were dependent on the assistance of their care-giver for their medications. A 5-point Likert scale ranging from very satisfied to very unsatisfied was used to measure the level of satisfaction of the participant regarding communication with his/ her health care provider where 66.2% participants were either satisfied or very satisfied with their healthcare provider.
Naming (brand name and generic name)
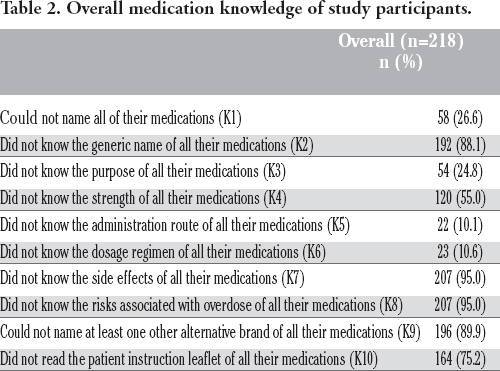
Table 2 shows that 26.6% of participants were unable to correctly name the brand names of all the medications that they were taking at the time their interview was conducted. Nervous system and mental disorder patients had the highest percentage of participants among this group (40%) while the other group of patients ranged between 20-34.4% (Table 3). In the Pearson χ2 test, no significant difference in ability to correctly name all medications was observed between participant groups of different age, level of education, area of residence, medication dosing strategy and level of satisfaction with healthcare provider (p=0.19 to p=0.77). Significant differences were observed for participants having different gender (χ2(1) = 4.08, p=0.04), language proficiency (χ2(1) =8.26, p=0.004), occupation (χ2(2) =6.44, p=0.04) and number of medicines taken (χ2(2) =5.99, p=0.05).
88.1 percent participants failed to correctly answer the generic names of all their medications (Table 2). In the Pearson χ2 test, no significant difference in ability to correctly say the generic names of all medications was observed between participant groups of different gender, area of residence, occupation and medication dosing strategy (p=0.10 to 0.28). Significant differences were observed for participants having different age level (χ2(2) = 35.73, p<0.001), level of education (χ2(3) =8.07, p=0.05), language proficiency (χ2(1) =4.58, p=0.03) and number of medicines taken (χ2(2) =6.71, p=0.04).
Purpose of medication (indication)
Approximately one fourth of the participants (24.8%) failed to correctly answer the purpose of the medication they were taking (Table 2). Patients suffering from genitourinary and liver diseases and nervous system and mental disorders were the ones with the least knowledge about their medicine's purpose (42.9 and 41.7 %, respectively) as seen in Table 3. In the Pearson χ2 test, no significant differences were observed between participants of different age group and occupation (p=0.15 to 0.13) in their ability to correctly answer the purpose of their medication. Significant differences were observed for participants having different gender (χ2(1) = 3.87, p=0.05), level of education (χ2(3) =8.14, p=0.04), language proficiency (χ2(1) =5.49, p=0.02), area of residence (χ2(1) =10.37, p=0.001), medication dosing strategy (χ2(3) =8.84, p=0.03), satisfaction with healthcare provider (χ2(1) =5.01, p=0.03), and number of medicine taken (χ2(2) =6.39, p=0.04).
Medication dosage (strength, administration route and dosage regimen)
To assess patient's medication knowledge, study participants were asked whether they knew the strength of their drug, which route to administer it (oral, injectable, etc.) and the dosage interval. Although 55% of participants could not answer the strength correctly, only about 10% participants failed to answer administration route and dosage interval of all their medicines (Table 2). In the Pearson χ2 test, no significant differences were observed in ability to answer strengths of all their medications correctly among participants of different age group, gender, area of residence and satisfaction over communication with healthcare provider (p=0.12 to 0.67). Significant differences were observed among participants of different level of education (χ2(3) =11.79, p=0.008), language proficiency (χ2(1) =13.48, p<0.001), occupation (χ2(2) =7.28, p=0.03), medication dosing strategy (χ2(3) =7.90, p=0.05) and number of medicines taken (χ2(2) =9.79, p=0.007).
Demographics and health condition related factors of study participants (n=218).
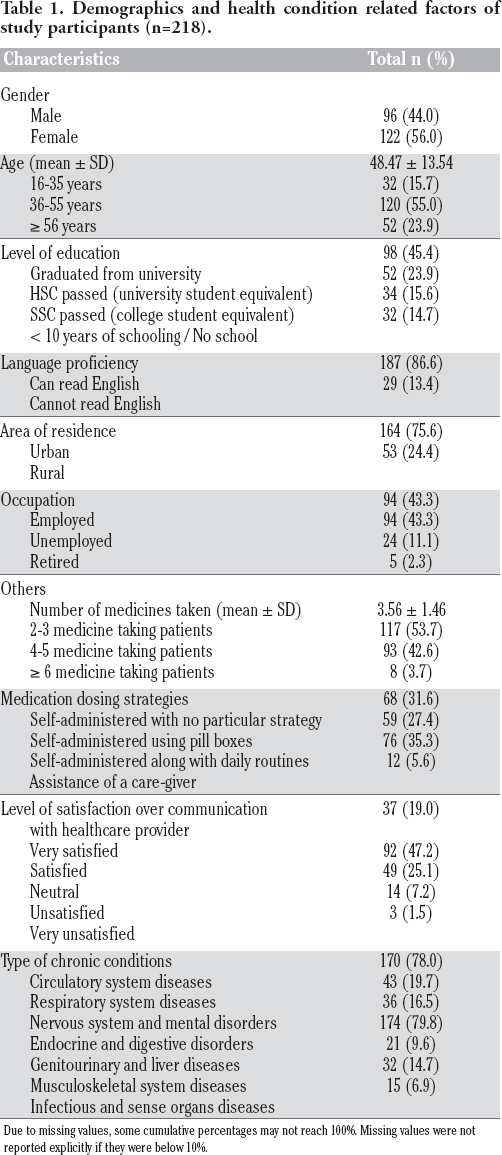
Due to missing values, some cumulative percentages may not reach 100%. Missing values were not reported explicitly if they were below 10%.
In case of participants ability to answer all route of administrations correctly, no significant differences were observed for any demographic group (p=0.12 to 0.85) other than medication dosing strategy (χ2(3) =17.04, p=0.001). Similar results were seen in case of dosage regimen where no differences were observed for different demographic groups (p=0.08 to 0.91) other than medication dosing strategy (χ2(3) =16.08, p=0.001).
Risk factors (side effect and overdose)
Participants’ knowledge of risk factors of their medication was associated with their ability to answer at least one side effect or at least one overdose correctly. In both cases, approximately 95% patients failed to answer at least one side effect or one overdose of all their medications (Table 2). In case of participants’ ability to answer at least one side effect of all their medications correctly no differences were observed for any demographic groups (p=0.17 to 0.97) other than number of medicines taken (χ2(2) =6.48, p=0.04). Similarly, no differences were observed any demographic groups (p=0.07 to 0.83) other than number of medicine taken (χ2(2)=6.48, p=0.04) in participants’ ability to answer at least one overdose related complication for all their medications.
Patient's awareness (knowledge of alternative brand and drug information leaflet)
Study participants were asked whether they knew the name of at least one alternative brand of the medication they were taking and whether they ever read the drug information leaflet provided along with their medication. Approximately 90% participants could not answer the name of at least one alternative brand of the medicines they were taking and only one fourth of all participants had ever read all their medicine's patient instruction leaflet (Table 2). In the Pearson χ2 test, no significant differences were observed among different demographic groups in their ability to name at least one alternative brand of the medicines that they were taking (p=0.051 to 0.89) except for the number of medicines taken (χ2(2) =10.6, p=0.005). In case of patient's willingness to read all their patient instruction leaflets, significant differences were observed in participants of different age group (χ2(2) =8.28, p=0.02), level of education (χ2(3) =12.83, p=0.005)language proficiency (χ2(1) =11.17, p=0.001) and number of medicine taken (χ2(2) =7.69, p=0.02) where no differences were observed in groups such as gender, area of residence, occupation, medication dosing strategy and satisfaction with healthcare provider (p=0.19 to 0.70).
Multivariate logistic regression analysis
The multivariable logistic regression analysis revealed that there was no significant correlation between the different demographic and health related factors with the participants’ ability to answer names of all their medications correctly (Table 4). However, being of older age (p=0.004) seems to be positively associated and number of prescribed medications seems to be inversely associated (p=0.027 for patients taking ≥6 medicine) with participants ability to answer purpose of all their medications correctly (Table 5).
Overall medication knowledge of study participants.
Comparison of medication knowledge of study participants and among patients suffering from specific conditions.

Participants who could answer names of all their medications correctly - Multivariate logistic regression.

Analysis was conducted using the ENTER method.
Participants who could answer purpose of all their medications correctly - Multivariate logistic regression.

Analysis was conducted using the ENTER method.
Discussion
We assessed multimorbidity patients’ ability to name their medication, state its purpose and other dosage related information and asked whether they knew any adverse effect regarding their drugs. Furthermore, their knowledge on alternate generic brands and awareness of reading drug information leaflet were also evaluated. The aim was to evaluate the health literacy of these multiple chronic condition affected patients and analyzing the factors associated with their medication knowledge.
Results of our study showed that majority of the study participants were able to correctly name and state the purpose of their medication. However, more than 26% of participants (n=58) could not name what medicine they were taking and almost 25% of participants (n=54) did not know or were confused regarding the purpose of their medication. Being unable to name your own medication is a matter of concern, as worse adherence to medication has been seen in hypertensive patients who rely only on visual identification of their medications. 27 In case of medical emergencies, forgetting one's medication during travel or beginning treatment at a new clinic can create a crisis situation when patients would only be relying on their recollection of medications. 19 What is even more alarming is the fact that 88% of patients (n=192) did not know the generic name of their medications. Prescribing a drug by its generic name is scarce in Bangladesh, thus people have little to no knowledge regarding the difference of brand and generic names. Almost 90% of the study participants did not even know any alternate brands of the medication they were using. If a particular brand is unavailable in a drug store, it may cause panic in patients as they might not know that there are other generic versions of that brand available in the store.
Almost a quarter of all participants had no clear knowledge about why they were taking their medication. Inadequate knowledge about the purpose and benefits of one's medication is a known cause behind low adherence in chronic patients. 28 In case of patients with multiple chronic conditions this can be even more severe, potentially leading to confusion between medications resulting in under-dose, overdose or toxic drug interactions. In the multivariable logistic regression analysis, age was seen to be positively associated with knowing the purpose of medication while number of medications taken seemed to be negatively associated. Though health literacy is generally poor in the elderly, it seemed that in our study, participants of higher age were more concerned and knowledgeable regarding their medication which is certainly interesting. This could be because most of the participants were close family members of undergraduate pharmacists, thus this impacted their overall knowledge regarding their medication. On the other hand, an increase in the number of medications a patient has to take can create more confusion and thus can lead to poorer medication knowledge, as was seen in our study.
In terms of medication dosage knowledge approximately 90% of participants were able to answer administration route and strength correctly. This can be attributed to the fact that most of participants in our study administers their medication by themselves. However about 55% participants had no idea about the strength of their medication which can be extremely dangerous because buying medication of wrong strength can either lead to potential toxicity or fail to achieve therapeutic effect.
Regarding knowledge about medications’ risk factors, only 5% patients could answer at least one side effect and one risk associated with overdose of all their medications. This is unsurprising, as adverse drug reaction related knowledge of patients have been very poor in several prior studies, ranging between 7% to 15% in surveys conducted in community pharmacies of Portugal and Spain.21,23 For safe and appropriate use of medication and making informed decisions regarding one's therapy, patients require a good basic apprehension of the risk and benefits of their prescribed medication and knowledge on how to administer them. 29 Even a patients’ compliance to recognize adverse effects and tolerate them depends on their ability to depict they symptoms and associate it with drugs.21,30
There are a number of drug information sources available today, many of which are unreliable and can spread misinformation among patients. Therefore, the drug information leaflet is considered the most trustworthy and highly regulated source of particular medication. 31 Only one fourth of our study participants claimed that they had read all their drug's instruction leaflet at least once. We found a number of literature with variable rate of patient reading drug information leaflet, insufficient rates of reading the leaflets being more common.32,33 Patients often cited the leaflets to be difficult to understand, some even implying that potential risk related information in the leaflet causes anxiety in them often leading to poor adherence.34,35We encouraged our participants to learn how to read the drug information leaflet from their healthcare provider, as it is an essential tool for enhancing health literacy of patients.
It is our opinion that lack of proper implementation of pharmaceutical care in our country culminates into poor health literacy as well as medication adherence. Physicians are at charge of both prescribing and dispensing medicines in Asian countries like China, Hong Kong, Thailand, and Malaysia and this is not uncanny for Bangladesh, too. 36 Though according to the National Drug Policy 2005, medicine distribution and utilization in retail pharmacies and hospitals should be under the supervision of qualified pharmacist, reality is quite different. As yet, no graduate pharmacist is working in retail pharmacies or Government hospitals of Bangladesh except very few tertiary private hospitals.37,38 As drug stores are often the first point of contact that patients have with the health system, lack of qualified pharmacists makes it difficult for the patients to gather proper information regarding generic and brand name of the drugs, brand alternatives, possible side-effects and adverse drug reactions. Given the large pharmacy graduates and workforce in Bangladesh, it could be argued that the expertise of the pharmacist is underutilized. 38 Pharmacists in community and primary care settings can be a key resource working in an interdisciplinary model for better medication management of patients with improved health literacy.
Conclusions
This study investigated the knowledge of medication name, purpose, dosage information, risk factors, alternate brand name and drug information leaflet reading rate among patients having multiple chronic conditions. A significantly large portion of participants had difficulty in remembering their medications’ name and could not state for which purpose they were taking it. Knowledge regarding dosage information was also pretty low and only a small proportion of participants had optimal knowledge on risk factors associated with their medication. Only a handful of participants could name alternate brands of their prescribed medication and only a quarter of the participants had ever read the drug information leaflet of their medication. This sub-optimal level of health literacy observed in the study participants could result in overall poor adherence to treatment. Patients may benefit greatly if their physicians or pharmacists could communicate the medication safety and use either verbally or by illustrated medication information brochures.
Strengths and limitations of this study
To our knowledge, this is the first qualitative study to explore the inadequacy of medication understanding among multiple chronic condition patients in Bangladesh. Study participants included had diverse levels of literacy, health related practices and had a balance of urban and rural population. Interviews were conducted in patients’ home, ensuring minimal wrong answers due to nervousness in unfamiliar settings. Generalizability of our study findings is greatly limited due to the small sample size and different habitats of participants. Different parameters of medication adherence were not measured nor the source of knowledge identified.
Footnotes
Acknowledgements
The authors would like to acknowledge Department of Pharmacy, University of Asia Pacific for providing facilities to conduct this research.