
Abstract
Introducing innovative health interventions into clinic settings requires a comprehensive and creative approach to multiple implementation challenges. To optimize implementation of a sexual and reproductive health intervention for young women with depression, we applied systems thinking and human-centered design thinking methods to develop tools and strategies to address issues influencing intervention implementation in diverse clinics. We recruited staff from three clinics that provide sexual and reproductive health and behavioral health care to young women. Across five sessions (four video conference calls, one in-person workshop), we used systems mapping to identify key stakeholders and their relationships, processes, and challenges to care; formed clinic staff-investigator design teams; brainstormed about challenges that would influence intervention implementation and considered potential solutions; prioritized implementation challenges; and designed prototypes of solutions. Participants responded positively to the systems thinking perspective and collaborative design thinking process. Findings included generalizable considerations about solving implementation challenges for clinic-based interventions, such as forming a team of champions representing the diverse disciplines involved in and impacted by intervention implementation, and creating multiple tools and strategies for implementation that can be tailored to a given clinic's culture.
Significance for public health
Implementing innovative health interventions in clinic systems requires consideration of multiple human, environmental, and process factors. To develop implementation tools and strategies for a sexual and reproductive health intervention for young women with depression, we applied systems thinking to consider clinic system elements and their connections, and human-centered design to tackle challenges with intervention implementation by centering on the clinic staff who would be experiencing these challenges. Using this approach, the investigators and clinic staff efficiently and effectively identified implementation challenges in diverse clinic settings and designed tools and strategies to overcome these challenges. This form of investigator-clinic staff collaboration, attention to system factors, and focus on creative solutions can inform research and care around implementing novel interventions in established clinical systems.
Introduction
Adolescent and Young Adult (AYA) women with depression are more likely to engage in Sexual and Reproductive Health (SRH) behaviors that place them at high risk of unintended pregnancy and sexually transmitted infections.1,2 Factors related to depression such as attempts to regulate affect, 3 including substance use, 4 pregnancy ambivalence, 5 difficulties with communication about condom use 6 and other relationship dysfunction (e.g., reproductive coercion 7 and intimate partner violence) 8 may result in lack of effective contraception, lack of consistent condom use, and sex with multiple or high-risk partners.2,9,10 High-risk AYA women with depression face compounded barriers to access and receipt of both mental health and SRH care, including stigma and lack of integration of medical and mental health services. 11
To address SRH risk in AYA women with depression, we developed the Momentary Affect Regulation–Safer Sex Intervention (MARSSI), which combines in-clinic counseling with a smartphone application for self-monitoring and messaging to prompt healthy behaviors and skills learned during the counseling. 12 Because replicating SRH interventions outside of research contexts can be challenging, 13 we conducted interviews with clinic key informants, 11 who emphasized the need for both clinical and administrative staff to understand how MARSSI aligns with the clinic mission and patient needs.
Evaluating and managing the multitude of facilitating, impeding, interacting, and competing factors in clinic systems and involving stakeholders are important to successful implementation of complex health care interventions. 14 Thus, we used systems thinking, which approaches problem-solving by seeking to understand elements in a system and how they connect and interrelate over time. 15 A systems thinking perspective has been used to support innovation and change in organizations, 16 including health care systems. 17
To develop MARSSI implementation solutions, we applied design thinking (also known as human-centered design), an approach to overcoming challenges that center on the people experiencing these challenges. The Stanford model proposes five stages of human-centered design: Empathize (understand how people think, act, and react in their environment), Define (express the target challenge), Ideate (generate ideas about solutions to the challenge), Prototype (create a simple, tangible solution with which the user can interact), and Test (solicit feedback about the prototypes from users). 18 Through a collaborative and iterative process, design thinking aims to rapidly produce creative solutions to complex problems. When applied to intervention development, implementation, and/or dissemination, design thinking may improve acceptability and effectiveness of health care interventions compared to traditional approaches. 19 The objective of this project was to develop tools and strategies for addressing issues influencing MARSSI implementation in diverse clinic settings through clinic staff/investigator collaboration, taking a systems thinking perspective and applying design thinking methods.
Methods
We conducted the project from December 2018 to May 2019 with institutional review board approval. From the seven clinics participating in key informant interviews, we identified four clinics in which staff expressed interest in improving SRH for AYA women with depression seen in their clinic. Following email solicitation, two staff from each of two clinics enrolled. We expanded recruitment and enrolled two staff from one additional clinic. Participants included a nurse practitioner, a nurse/family planning counselor, a health services advocate/case manager, and three behavioral health counselors (one from each of the three participating clinics). Clinics included a drop-in clinic for runaway, homeless, and high-risk youth; a community health care center serving a low-income, largely Latinx population; and a hospital-affiliated AYA clinic serving a diverse population.
We conducted the implementation design process across five sessions (Table 1), progressing through the Empathize, Define, Ideate, and Prototype stages of the Stanford design thinking model. 18 Recognizing that our clinic staff participants were volunteering their time, we aimed to maximize flexibility and efficiency by conducting the sessions primarily via 1-hour video conference calls (Sessions 1, 2, 4, and 5), with one 4-hour in-person workshop (Session 3). We remunerated participants for time/effort (up to $300 in gift cards) and parking for the workshop.
In Session 1, after reviewing the key informant findings, we used systems mapping to show how people and processes in the clinic system are related and how change occurs within different clinics. 16 Each participant shared a system map for before and after a new idea, process, or tool was introduced in their clinic. We then discussed steps in planning for change. 20 Between Sessions 1 and 2, we formed three design teams of two staff from different clinics and one investigator, making assignments to maximize diversity of training, experience, and communication style. The MARSSI research coordinator participated in each design team's video calls to assist with meeting documentation and planning.
In Session 2, teams met separately to develop ideas about implementation strategies. Each team generated a systems map representing an ideal clinic system that provides SRH care to highrisk young women, conducted stakeholder mapping to identify who would be invested in MARSSI implementation, and describe stakeholders’ mindset, needs, and goals. 21 Each team member imagined being a champion and/or counselor for MARSSI and identified challenges within the ideal clinic system. 21 Each team discussed the challenges, related considerations, and potential solutions, then rated their ideas by importance to successful MARSSI implementation and by difficulty to put into practice.
For the in-person Session 3 workshop, teams continued brainstorming. In a Round Robin, 21 one team member identified a challenge, the next member proposed an unconventional solution, and the third member suggested a reason the solution would fail. The team brainstormed improved or alternative solutions, and shared their ideas with the large group. We compiled proposed solutions to implementation challenges and participants voted on solutions to prioritize for prototyping. Based on the votes, we selected three challenge-solution areas and randomly assigned one to each team. Teams then prototyped solutions for their challenge-solution area via a physical model and/or role-play (“show the details”) and storyboarding to tell the story of the user's (patient's and/or staff's) experience with the solution (“show the big picture”). 11 Each team presented their prototypes to the group.
After the workshop, project personnel edited the prototypes to reflect the discussion, then teams met separately to review, refine, and expand on their prototypes (Session 4). Project personnel made desired changes to the prototypes, then teams shared with each other their refined prototypes and discussed plans for a future study to test the prototypes (Session 5).
Description of implementation design sessions.

We evaluated the project through emailed surveys following each session. The surveys included 6-13 items about session logistics and content (1-Strongly Disagree to 5-Strongly Agree) and free text on participants’ most and least favorite parts of the session.
Results
Mean item scores on feedback surveys were all 4-Somewhat Agree or 5-Strongly Agree. For each session, all participants agreed with the statement, “I had the opportunity to contribute to the session”. Participants’ favorite parts of the sessions were: creating, sharing, and/or discussing their system maps (Session 1); brainstorming about MARSSI implementation as a team using the shared whiteboard, and discussion (Session 2); Round Robin brainstorming, prototype model creation, and storyboarding (Session 3); seeing the prototypes and designing next steps (Session 4); and seeing the revised prototypes and collaborating with other teams (Session 5). Participants described different aspects of their team's solution that they thought was most important, including “presenting/explaining MARSSI to providers and staff”, “increasing the buy-in/marketing”, “the prototype”, and “LGBTQ inclusion”.
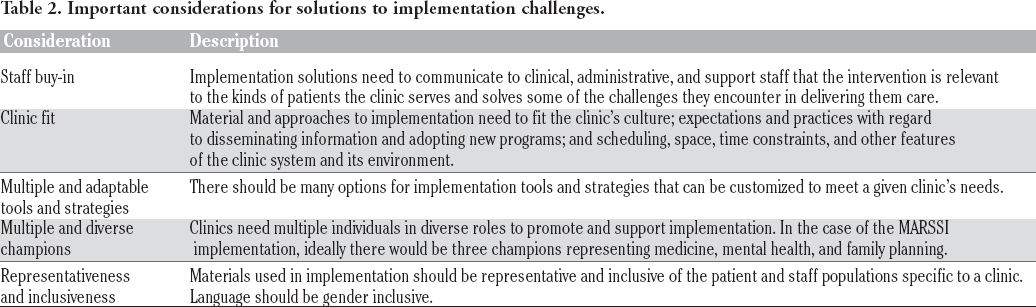
The design thinking process yielded several generalizable considerations regarding solutions to innovation implementation challenges (Table 2). Participants discussed the critical importance of staff investment in the program's implementation, which was reflected in the prototypes. Specifically, staff would need to understand how the program was relevant to their patients, addressed problems with patient care, and/or connected to their clinic's mission. Participants talked about fit of implementation materials and approaches with a specific clinic's culture, setting, and operations, as well as fit with the clinic's expectations for implementation of new programs. Participants expressed desire to create multiple options for flexible and adaptable implementation tools and strategies that could be customized to meet a given clinic's needs.
Participants identified that clinics needed multiple staff members representing different constituencies to cheerlead, organize, and motivate program implementation, with the ideal “team of champions” representing medical care, mental health care, and family planning. As one team observed, the system map was helpful in identifying these three staff groups. Acknowledging connections between clinical care and leadership, ideally at least one champion would “have the ear of clinic administration”.
Participants emphasized representativeness and inclusiveness throughout the design process. They created materials that could be adapted to represent staff as well as patients in a specific clinic. For example, one proposed strategy to enhance buy-in was to have staff create patient-facing postings about MARSSI. To avoid excluding individuals who identify as transgender or nonbinary, participants suggested that program materials be gender-inclusive.
Each team designed prototypes for both processes and materials to support MARSSI implementation (Table 3). Process prototypes included job descriptions for the implementation champions and the program coordinator; a guidance document describing key considerations for developing a clinic-specific poster for patients; and recommendations for a toolkit of sample materials and strategies from which a clinic could customize tools for their implementation. Material prototypes included posters advertising MARSSI to staff and to patients, and incentives for staff branded with the program logo.
Discussion
This study demonstrated a flexible approach to clinic staff/investigator collaboration that can be used to generate design ideas and create prototypes for innovative program implementation in community clinics. By planning and structuring two initial video conference sessions, we were able to efficiently present systems mapping and design thinking activities in preparation for a fertile discussion about challenges to implementation and creative hands-on activities to design prototype solutions during our in-person workshop. Work done by the investigators in between sessions accelerated the design process.
Important considerations for solutions to implementation challenges.
Process and material prototypes for solutions to implementation challenges.

The systems thinking perspective led participants and investigators to consider aspects of complex clinic organizations related to SRH care of AYA women with depression throughout the implementation design process. We created and iterated on systems maps; identified and discussed challenges to MARSSI implementation within clinics; and designed and produced potential solutions to key challenges that involved cultural, structural, and/or operational organization changes. Participants enjoyed the systems thinking process and found it helpful in identifying and solving implementation challenges. Such practical application of systems thinking can inform intervention implementation by identifying key system components, gaps in implementation plans, and unintended as well as intended effects in context. 22
Participants prioritized staff buy-in and champions for successful implementation of MARSSI, expanding on results from our key informant interviews. 11 According to Diffusion of Innovations theory, champions contribute to the success of innovation within an organization by overcoming resistance or indifference through their charisma and personal efforts to support change. 23 Champions both for specific projects and for organizational change are critical for effective implementation of innovations in primary care.23,24 For interventions involving multiple disciplines within a clinic, our findings suggest that forming a team of champions through solicitation of representatives from each discipline may be an important part of the champion component of the implementation strategy. Participants also emphasized the importance of fit and flexibility in implementation approaches. Clinic culture strongly affects effectiveness of intervention implementation; thus, implementation planning must identify and accommodate organizational processes and characteristics that comprise a clinic's culture. 25 Our findings suggest that multiple and adaptable tools and strategies may facilitate tailoring implementation approaches to a specific clinic's culture.
Participants recommended that program implementation materials be tailored to reflect the sociodemographic diversity of clinic staff and patients. Based on characteristics associated with positive program effects for adolescent pregnancy prevention programs, 26 we designed MARSSI for AYA women, gender specificity that excludes other individuals who might benefit from MARSSI (e.g., transgender or gender nonbinary individuals who may be able to become pregnant). Adolescent pregnancy prevention programs need to give careful consideration to balancing evidence-based recommendations for gender specificity 26 with best practices for promoting gender-inclusive clinic culture and health care. 27
Despite enthusiasm from clinic leadership, we were able to recruit staff from only three of the five clinics we approached. We had hoped to conduct Session 1 in a single video conference so that we could introduce participants to each other “live”. However, it was difficult to schedule a single time based on participant availability. We did not have the time or funding to continue to iterate on our prototypes, test our tools and strategies in clinics, or experience early failure; therefore, we were unable to determine effectiveness of our strategies on MARSSI implementation. 19 We will be testing the implementation prototypes resulting from this study in a pilot study of MARSSI in community clinics that is underway.
With systems thinking and human-centered design methods, a clinic staff/investigator collaboration created innovative tools and strategies to support implementation of an SRH risk intervention for AYA women with depression. Through this project, we designed new approaches to optimizing MARSSI uptake and sustained use in diverse clinics, in collaboration with clinic staff, and included an enhanced understanding of gender diverse populations and program delivery. Applying systems thinking and design thinking to improve program implementation may be useful to researchers and practitioners seeking to introduce novel interventions to established systems of care.
Footnotes
Acknowledgments
The authors would like to acknowledge the clinic staff participants who gave their time, effort, and creative energy to this project. This opportunity is made possible by Grant Number TP2AH000046 from the HHS Office of Adolescent Health as part of the Innovative Teen Pregnancy Prevention Programs (iTP3) project. Contents are solely the responsibility of Boston Children's Hospital and do not necessarily represent the official views of the Department of Health and Human Services, the Office of Adolescent Health, or Texas A&M University.