
Abstract

Defining migration
Human migration is the movement of people from one location to another with the aim to settle and ensure improvement of their social and economic status as well as to generate beneficial societal outcomes for countries of destination and of origin with remittances of more than half-a-trillion USD in 2016. Currently, population movements are mainly driven by economic purposes such as poverty, unemployment and poor living conditions, as well as humanitarian reasons with people fleeing from conflicts, oppression and natural disasters.
The phenomenon of mixed migration (individuals using the same routes and means of transport but for different reasons; Table 1) 1 has increased with the improvements of affordability in transportation and telecommunication technology. This situation has led to an acceleration and change of migration patterns with an estimated one billion people on the move, or 14.3% of the world's population, in 2015. From an economic point of view, migration's pattern changes from a high-emigration state to a high-immigration one as the country's economy grows. On the other hand, the surging numbers of asylum seekers (3.2 millions in 2015), refugees (21.3 millions in 2015) and other migrants such as internally displaced persons (40.8 millions in 2015) are due to oppression, conflicts and domestic inequalities in countries of origin. 2 Therefore, characterising countries is challenging as, for instance, previous destination countries have become nowadays land of transit (i.e., Libya) towards higher-income ones (i.e., European Union Member States).
Definition of migrants. 1
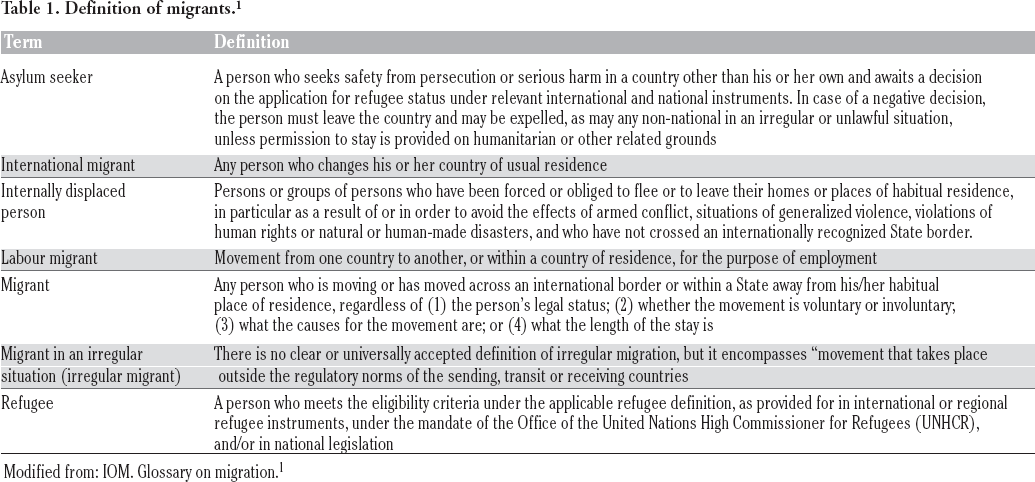
Modified from: IOM. Glossary on migration.
Impact of migration on health of people
During their journey towards the destination, migrants face serious health problems due to the unsafe routes undertaken, exposure to smuggling and trafficking networks, and crowded living conditions. Additional distress might be experienced by migrants due to changes in their administrative status during the journey and in country of destination, which may lead to further marginalization. For instance, an asylum seeker may acquire a refugee status and then become irregular once employment is lost or the allowed permission to stay is expired. 3
In general, migrants have health problems that are similar to those of the general population, although they have the extra challenge of facing a new cultural and environmental situation which may result in serious social and economic stress. 4 This adds to the existing linguistic and legislative barriers when trying to access public services. The end-result is that migrants may become increasingly susceptible to ill health and develop both communicable and non-communicable diseases (NCDs) while living at the edges of the society.
Vulnerability to infectious diseases
In general, the first concern in high-income countries is one of protecting the indigenous community from infectious diseases imported through irregular migrants. However, this is unusual and when exotic infections are detected in high-income, recipient countries they generally involve regular travellers such as tourists and health care workers rather than migrants and refugees. Migrants, however, are at risk of infectious diseases during the different phases of migration because of exposure to a variety of pathogens, difficulties to access health care, frequent treatment interruption, and poor nutrition and living conditions. Infectious diseases screening in countries of transit and destination are generally the same and are focused on tracking persons with tuberculosis (TB) and latent TB infection; human immunodeficiency virus (HIV) infection; sexually transmitted diseases; hepatitis B and C. These diseases tend to reflect the epidemiological profile of the countries of origin, even though a number of cases are acquired once arrived at destination given the frequent risk of exposure.
Vulnerability to non-communicable diseases
In most settings, health information concerns infectious diseases rather than NCDs, the risk of which increases alongside the time spent in the country. The rise in prevalence of such diseases is generally due to either lack of inclusion of migrants in screening programmes and failing of preventive measures. Furthermore, migrants may disproportionally suffer from mental disorders attributable to the cause of displacement like conflicts and oppression, migratory processes that often include physical and psychological violence, and destination settings where racism, marginalization and stigma may prevail. In this contest, children, especially those unaccompanied, are the most vulnerable groups at great risk to develop depression and symptoms of a post-traumatic syndrome disorder due to conflict-related violence, physical and sexual abuse, and loss of relative or carrier. To complicate matters, migrants might suffer from self-stigmatization due to perceived negative beliefs about mental disorders in the country of origin that affects their health-seeking behaviours. Finally, untreated mental disorders, stress of adapting to a new environment, including that of the bureaucratic process, and the psychological consequences of previous war experiences might lead to an increase consumption of alcohol and other substances. 5
The international response
In light of the importance of migration-related health issues, the international community has enhanced actions, starting from the 2008 World Health Assembly (WHA) Resolution on the health of migrants, 6 and the subsequent Global Consultation in Madrid in 2010 aiming to identify and improve migrant health strategies and priorities. The general tendency of such initiatives was to move from a disease-control approach towards a people-centred approach. Therefore, greater emphasis has been placed on human right-based, equity-driven health system strengthening also through a multisectoral approach. The first pragmatic measures were conceived by the World Health Organization for specific diseases such as TB, 6 malaria, 7 and Ebola virus infection through the post-Ebola revision and implementation of the International Health Regulations 2005. All these approaches had in common an increased attention to the human mobility in cross-country border areas and along mobility pathways, as communicable disease spread is one of the main concerns. Regrettably, in the same period of time migration was not recognized in other international frameworks for health equality such as the Social Determinants of Health agenda (2008-2011) and the framework on integrated people- centred health services (2015), which address equity in access to care on the basis of nationality and citizenship.
Finally, in 2015 the United Nations General Assembly adopted the 2030 Sustainable Development (SDG) Agenda and its 17 SDGs based on the principle of leave no one behind. Embedded into the new framework there are specific goals and targets promoting action on migrant health through a multisectoral approach with different actor and stakeholder engagement. The specific goals, directly or indirectly, related to migrants are shown in Table 2. 8 For the first time in history, the new agenda establishes an explicit objective for migrants under SDG 10, target 10.7 facilitate orderly, safe, regular and responsible migration and mobility of people, including through the implementation of planned and wellmanaged migration policies. Furthermore, in line with SDG 3, target 3.8 on Universal Health Coverage (UHC), one would expect that mobile individuals living at the edge of society and struggling to access public services would be prioritised through the establishment of reliable and accessible migrant-sensitive services.
Sustainable Development Goals (SDGs) and Targets related explicitly (*) or indirectly to migration.

Modified from: United Nation. Transforming our World: The 2030 Agenda for Sustainable Development. 8
Migrant-sensitive health services
To achieve the target of provision of migrant-sensitive access to health there is a need to renovate and strengthen both service delivery and the system organizational framework. 9 The aim of the WHA70.15 resolution of 2017, Promoting the Health of Refugees and Migrants was to build such framework to identify priorities in migrant health management utilising evidence-based information on best practices. The framework was focused on ensuring a proper attention on health issues and on drafting of an action plan on migrant health, taking into consideration the Office of the High Commission for Human Right's CESCR General Comment No. 14 (E/C. 12/2000/4) on the right to health of migrants. This document highlights four types of barriers in access: physical, financial, information and discrimination. Such obstacles have a great impact among migrants, particularly those experiencing poverty and social exclusion. Therefore, a proper migrant-sensitive system should provide free of charge services, with availability of interpretation and language-appropriate written materials. To reduce discrimination, health care workers must be trained to be culturally sensitive and well-informed, thus knowing how to raise a topic according to the beneficiary. Efforts should be made to overcome possible societal stigma originating from the home country culture, especially when handling mental health disorders, as well as lack of trust in providers. In addition, adapting services for adverse living and working conditions through regular working hours and reasonable service locations can increase adherence and outcomes of treatment. The model of care should also account for the nature of risk factors and health determinants, together with the co- or multi-morbidities connected with social disadvantages. Engaging people and local communities in the strengthening of health services may prove crucial.
Migrant-sensitive information systems: A key to solutions
To better comprehend and address the needs and the barriers of migrants and sustain evidence-based policy planning, enhancing health information system capacity is critical. 6 Digital health technology is a key to achieve the SDGs and to improve the well-being of people. 10 At local level, health authorities can assess and capture data on the reason why people do not access, and benefit from, health services. This information is needed to avoid falling into empirical imprecise approaches to address migrant health issue not founded on accurate and reliable data, especially given the complexity and variety of modern displacement and migration. At supranational level, there are no common indicators and variables, nor is there standard methodology to collect migration-relevant data. As a result, information is often not standardized and comparable. For instance, some countries collect data only on current nationality, country of birth and nationality at birth, while others collect information on migratory status, country of origin, mode of travel and reason for migration; or just country of origin and reason for migration. To address this heterogeneity, it is crucial that the international community identifies indicators and migrant-relevant data enabling international comparison and interpretation of shared information. Furthermore, it is important to establish a common terminology on migrants’ administrative status, because the collection and monitoring of health data might differ among migrant populations. Finally, national health information systems should collect standardized and disaggregated data for all migrants. Indeed, well-informed, reliable databases are needed to support rational national and international health policies and planning.
Conclusions
Migrant health is today a global health priority given the high mobility of people and populations and the formidable challenges people must face when reaching their destination. The more migrant-sensitive systems and services are, the less stressful the experience will be for both migrants and care providers. In the end, the SDG 3 imperative is to ensure healthy lives and promote wellbeing for all at all ages. More vulnerable people like migrants deserve to be prioritised and receive the best possible prevention and care services: hosting healthy, rather than sick, individuals and citizens – whatever their country of origin and birthplace is – is in the best interest of all societies.
Footnotes
Contributions: MCR, conceptualization and supervision, writing, final review and editing; SV, data elaboration and literature review, writing, original drafting.
Conflict of interest: the authors declare no potential conflict of interest.
Funding: none.