
Abstract
Background
One of the constraints in the utilisation of maternal healthcare in India is the out-of-pocket expenditure. To improve the utilisation and to reduce the out-of-pocket expenditure, India launched a cash incentive scheme, Janani Suraksha Yojana (JSY), which provides monetary incentive to the mothers delivering in public facility. However, no study has yet examined the extent to which the JSY payments reduce the maternal healthcare induced catastrophic out-of-pocket expenditure burden of the households. This paper therefore attempts to examine the extent to which the JSY reduces the catastrophic expenditure estimate household expenditure on maternity,
Materials and methods
The study used data on 396 mothers collected through a primary survey conducted in the rural areas of the Varanasi district of Uttar Pradesh state in 2013-2014. The degree and variation in the catastrophic impact of households’ maternity spending was computed as share of out-of-pocket payment in total household income in relation to specific thresholds, across socioeconomic categories. Logistic regression was used to understand the determinants of catastrophic expenditure and whether the JSY has any role in influencing the expenditure pattern.
Results
Results revealed that the JSY beneficiaries on an average spent about 8.3% of their Annual Household Consumption Expenditure on maternity care. The JSY reimbursement could reduce this share only by 2.1%. The study found that the expenditure on antenatal and postnatal care made up a significant part of the direct medical expenditure on maternity among the JSY beneficiaries. The indirect or non-medical expenditure was about four times higher than the direct expenditure on maternity services. The out-of-pocket expenditure across income quintiles was found to be regressive
Conclusions
It can be concluded that the JSY appeared to have achieved only a limited success in reducing the economic burden due to maternity. To reduce the catastrophic burden, policy makers should consider increasing the JSY reimbursement to cover not only antenatal and postnatal services but also non-medical expenditure due to maternity. The government should also take appropriate measures to curb non-medical or indirect expenditure in public health facilities.
Keywords
Significance for public health
Improving the well-being of mothers is an important public health goal for India. For improving maternal health, it is necessary that mothers utilize maternity services. However, maternity often becomes an economic burden, especially for disadvantaged and poorer groups of the society. To encourage mothers to utilize services, India launched a conditional maternity benefit transfer scheme back in 2005. This study explored whether the scheme has been able to help alleviate the burden of maternity expenditure or not. The study finds that the scheme has been successful only partially to reduce outof- pocket expenditure suggesting that maternity is a costly affair in rural India. Since the scheme is unable to save mothers from catastrophic expenditures, it is also unable to save mothers from a wide ranges of health illeffects caused by catastrophic expenditure.
Introduction
Maternal mortality is the main contributor to female mortality during the reproductive span. India, the largest democracy in the world, bears the brunt of the highest number (56,000 in 2010) of maternal deaths in the world. 1 It is an established fact that ensuring facility-based skilled professional care for every mother could bring down maternal mortality significantly.2,3 However, the level of maternal healthcare utilisation in the country is still low. One reason behind such a low usage of these services is that a considerable number of households have very low or no capacity to pay for such services.4-6 For such households, the out-of-pocket expenditure on maternity care at times become catastrophic due to the lack of insurance or other risk pooling mechanisms.7-13
To increase the utilisation of maternal health care and to reduce the out-of-pocket expenditure of maternity care, India in the year 2005 launched the
A review of previous literature reveals that there exist several studies on the coverage of maternal care services and the differentials in the out-of-pocket expenditure on maternity care in India. However, most of them do not focus on the JSY. For instance, Goli
The JSY was launched to encourage mothers to use free services at the point of delivery in addition a cash incentive of $22. Although maternal healthcare services in all public health facilities are supposed to be free, childbirth in these facilities often incurs a variety of medical (direct) and non-medical (indirect) out-of-pocket expenditures. Previous studies have considered only medical or direct expenditure while calculating the out-of-pocket expenditure on maternity care even though the indirect or non-medical costs such as loss of wages of women during maternity, loss of wage of husbands for accompanying, transportation and special food costs for the woman may impact households’ financial situation negatively. To the best of our knowledge, no study has measured the role of indirect or non-medical expenditure yet.
This paper therefore attempts to estimate maternity expenditure,
Materials and Methods
Area of the study
The study area, Varanasi district, is in Uttar Pradesh, the most populous state in India, with over 200 million people living over an area of 93,000 square miles. Due to high levels of pre-NRHM maternal and infant mortality,16,23 the state was identified as one of the
Sampling and data collection
To obtain a comparison of maternal health care expenditure incurred by JSY and non-JSY beneficiary, it was necessary to select a district with a fair share of both type of institutional deliveries – deliveries conducted in public and deliveries conducted in private facilities. Therefore, all 70 districts of the state were ranked by their coverage of institutional delivery as reported in the Annual Health Survey (AHS), 2010-11. The district of Varanasi was selected as it satisfied both criteria - the percentage of institutional delivery in the district was relatively high, and it also had a fair share of both kind of deliveries - about 25% conducted in public health facilities and about 40% in private health facilities. 15
A field survey was conducted during October 2013 to April 2014 in rural areas of the Varanasi district. Only those households that had at least one woman with a history of child birth during the period of 12 months preceding the survey, were considered for inclusion in the study. To select the households, the survey used two-stage sampling - villages in the first stage and from these villages, women with a birth during the reference period in the second stage. The villages were selected with probability proportional to size after stratification by village population size and the number of women to be selected from each village was specified so that the sample becomes self-weighting.
From each village, a list of women who delivered in the specified reference period was prepared with the help of community health workers and the stipulated number selected at random. A sample size of 400 was proposed taking into account sampling error and in order to accommodate non-response the sample size was raised by 10% to 440 so that about 400 women would be successfully interviewed. However, a total of 396 women could be contacted and were interviewed; of whom, 223 women had received JSY benefits as they delivered in public healthcare facilities and 173 women had not received any JSY benefits since they either delivered at home (n=31) assisted by unskilled birth attendant or at a private health facility (n=142). In this paper, the terms
Informed consent
A permission to carry out the study in villages was sought from the Chief Medical Officer (CMO) of Varanasi district. The village head (
Measurement of maternity expenditure and monthly per capita consumption expenditure
To estimate maternity expenditure,
Measurement of catastrophic expenditure and catastrophic overshoot
The calculation of catastrophic expenditure on maternity care requires data on the total out-of-pocket maternity expenditure and the total household consumption expenditure/income.
20
As mentioned earlier, the household consumption expenditure has been used as the proxy income variable in the study.
25
The MPCE is multiplied by twelve to obtain the annual consumption expenditure. This study considers 10% of the total annual consumption expenditure and 40% of the
Examining predictors of catastrophic maternal health care expenditure
A binary logistic regression was carried out to examine how catastrophic maternity expenditure is associated with socio-economic characteristics. The dependent variable
This regression analysis included several key socio-economic and demographic variables as predictors of catastrophic expenditure. The choice of the variables to be included was guided by the existing literature in the Indian context.9,27,29 Household income, religion, caste, and education are some important socio-economic variables that previous studies have found to have considerable influence the health seeking behaviour of women in India.9,12,26,30 Among demographic variables, the age of woman is considered an important predictor variable of the utilization of maternity care services. The parity of woman and the sex of the child have been found to determine the decision to go for an institutional delivery; women with higher age and higher birth order are less likely to use maternity services. 3 All independent variables were categorical.
Results
Table 1 presents the descriptive statistics of the study population. It reveals that a great majority of the sampled JSY beneficiaries were Hindu and belonged to OBC category. About 65% of the JSY beneficiaries had two to three children whereas the proportion of such women among non-JSY women was about 57%. About half of the women included in the study were illiterate and over 65% women who received JSY did not work outside other than their household chores. About 36% JSY beneficiaries reported that their husbands worked as casual labourer; the corresponding figure for the non-JSY women was about 30%. The distribution across consumption quintiles did not reveal any significant difference between JSY beneficiaries and non-JSY women. For most variables, the two groups were within a close range.
Background characteristics of surveyed women, field survey, Rural Varanasi, 2013-14.

Note: n=number of women.
Table 2 presents descriptive statistics of direct and indirect expenditure incurred due to maternity segregated by JSY beneficiaries and non-JSY. It reveals that the mean total expenditure for JSY beneficiaries and non-JSY women was Rs.5975 and Rs.23632, respectively. In other words, the mean total maternity expenditure incurred by JSY beneficiaries was about one fourth of the amount incurred by non-JSY women. The total direct expenditure among the non-JSY women was about 16 times higher than JSY beneficiaries while the indirect expenditures for both groups were similar. A major part of the total expenditure came from the indirect expenditure indicating that maternity not just incurs medical (direct) costs but also brings about other financial burden. The median expenditure on ANC and PNC for the JSY beneficiaries and on PNC for non-JSY women indicated that about half of the women either did not utilize the service or did not spend anything on the same.
Descriptive Statistics for all components of maternal health care expenditure, field survey, rural Varanasi, 2013-14.

ANC: Antenatal care; PNC: Postnatal care; INR: Indian National Rupee. One US$ was approximately equal to Rs.60 in 2014; SD: Standard Deviation. Here the total expenditure is the amount before JSY reimbursement. After JSY reimbursement the amount is Rs.4575 (Mean) and Rs.3000 (Median). JSY beneficiary (n=223), non JSY (n=173).
Table 3 presents the expenditure on maternity care as the share of annual consumption expenditure of the household by expenditure quintiles. It also provides information about the reduction in out-of-pocket expenditure after JSY beneficiaries got reimbursed. The results show that on an average total maternal expenditure among JSY beneficiaries worked out at about 8% of their annual household consumption expenditure, whereas among non-JSY women, it turned out to be much higher – about 28% of their annual household consumption expenditure. The reimbursement of the JSY money reduced the share of maternity expenditure only by 2.1% of annual household consumption expenditure. It is evident from the results that the expenditure burden declines progressively as one moves from a lower to a higher expenditure quintile. A sharp rich-poor gap in the share of expenditure indicated that health care expenditure was highly regressive,
Expenditure on maternity as share of annual household consumption expenditure, field survey, Rural Varanasi, 2013-14.

TDE: Total direct expenditure, TIDE: Total indirect expenditure, TMHCE: Total maternal health care expenditure, AHCE: Annual household consumption expenditure.
Catastrophic headcounts and overshoots at different thresholds, field survey, Rural Varanasi, 2013-14.

JSY beneficiary (n): 223, non JSY (n): 173, JSY beneficiary without reimbursement
Table 5 presents differentials in the mean out-of-pocket expenditures on maternity by selected background characteristics. The average out-of-pocket expenditure was lower among Muslim women compared to Hindu women. The total expenditure incurred by ‘working’ women was found to be high as the loss of wage due to maternity substantially raised the burden of OOP expenditure on maternity. The JSY beneficiaries whose husbands were engaged in agricultural activities incurred the highest OOP expenditure on maternity followed by those women whose husbands worked as casual labour. Poorer JSY beneficiaries spent belonging to two bottom (poorest and poor) quintiles more money on maternity than the ones beloning to the two top (rich and richer) quintiles.
Expenditure on maternity, catastrophic headcounts, odds ratios by background characteristics of women, Rural Varanasi, 2013-14 (n=396).
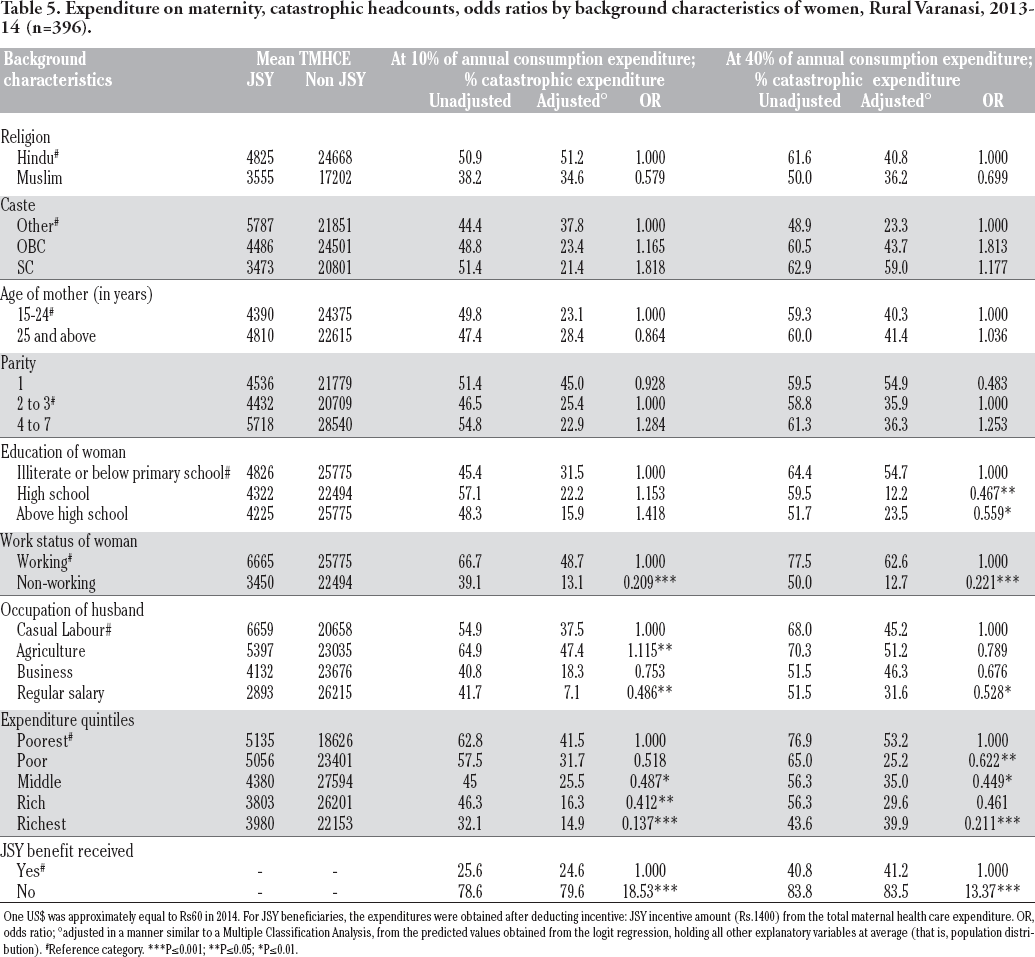
One US$ was approximately equal to Rs60 in 2014. For JSY beneficiaries, the expenditures were obtained after deducting incentive: JSY incentive amount (Rs.1400) from the total maternal health care expenditure. OR, odds ratio; °adjusted in a manner similar to a Multiple Classification Analysis, from the predicted values obtained from the logit regression, holding all other explanatory variables at average (that is, population distribution).
Reference category.
P≤0.001
P≤0.05
P≤0.01.
The gross (unadjusted) and net (adjusted based on logistic regression coefficients) percentages of catastrophic head counts for both, the 10% of total annual consumption expenditure threshold and the 40% of non-food expenditure threshold, are also presented in Table 5. Results of logistic regressions showed the determinants of catastrophic maternity expenditure. Adjusted percentages are the predicted probabilities (expressed as percentages) of the dependent variable computed for each category from the logit regression coefficients, holding the other variables at average level or distribution. The results show that more
Table 5 also presents the odds of suffering from catastrophic expenditure. Religion, caste, and parity of women did not turn out to be statistically significant predictors of incurring catastrophic expenditure. The likelihood of incurring catastrophic expenditure at 10% of income threshold was higher in women with primary to secondary-level of education compared to illiterate and less than primary educated women while the odds at 40% of non-food expenditure were higher among women with primary-level education.
Discussion
The present study estimates all direct (formal and informal medical expenditure) and indirect expenditure incurred by households due to maternity and examines the extent to which the JSY incentives reduced the burden of cost incurred. The findings of the study suggest that the JSY beneficiaries incur a substantial amount of direct out-of-pocket expenditure on maternity care even though the publicly-funded health system is supposed to provide its services free of cost. It turns out that close to one-fourth of total outof- pocket expenditure on maternity care by the JSY beneficiaries comes from direct expenditures which ideally should not incur as the public health system is supposed to provide maternity services free of cost.
This direct out-of-pocket medical expenditure may have incurred due to several reasons. Previous studies have found that the low availability of essential medicines at public health facilities and corrupt practices prevalent among doctors and pharmacists force patients to purchase medicines from private pharmacies where there is higher availability of medicines and for many medicines, only one brand of the product is available usually the costly one. This leaves patients with no choice but to buy that costly branded product thereby incurring catastrophic drug expenditure. 31 The user charges and informal payments (bribes) to the providers and other health workers are also added to the expenses.
Kickbacks and bribery in India's public health facilities are a common phenomenon. 32 Kickbacks are illegal in India, but they are nearly impossible to avoid in public health facilities, especially for the poor and illiterate. Patients incurr a lot of informal payments during various stages of maternity in lieu of services received from the health facility. Moreover, the public health system is generally perceived to be incompetent to treat emergency obstetric complications and the patients prefer to visit the private providers for the treatment. Also the women who undergo C-section in the district hospital have to bear additional treatment costs. It is also a fact that most women are unaware of the benefits they are entitled to receive under the JSY for C-section delivery in accredited private hospitals. An important finding of the present study is that the indirect or non-medical expenditure forms a major chunk of the out-of-pocket payments made towards maternity. A deeper look into the data collected from the field reveals that mothers often have to pay for transportation from their own pocket. Although the state has a 24×7 free ambulance services, the fact of the matter is it is not always available, at least in Varanasi district, forcing patients to use unregistered private vehicles.
Another major source of the indirect expenditure is the loss of mother's wages during maternity period. It is a well-established fact that poor women continue to work to earn a living for the family right up to the last days of their pregnancy, thus not being able to put on as much weight as they otherwise might. They also resume working soon after childbirth, even though their bodies might not permit it preventing their bodies from fully recovering, and their ability to exclusively breastfeed their new born in the first six months. Therefore, there is urgent need to introduce a modest maternity benefit in the JSY to partly compensate for their wage loss. Although, the Government of India has announced a new scheme entitled
The analysis showed that the maternal health expenditure even in the public sector was regressive. In other words, the poor women a relatively higher proportion of their disposable income compared to the rich women to avail maternity services from publicly- funded health facilities. Even in absolute terms, the expenditure of poorer JSY households on maternity care exceeded that of richer households by about Rs.2000. It is argued that that due to low social capital, the poor people are often forced to make a lot of informal payments in public health facilities to receive services, while the rich pay no extra or informal fees and enjoy the service free of charge.
One important question that this paper asked at the outset was that to what extent the JSY protects households from incurring catastrophic expenditure. The analysis revealed that the monetary incentive of the JSY helped only about 8.1% (33.7% without JSY benefit and 25.6% with JSY) households at 10% of consumption expenditure threshold and 15.3% households (56.1% without JSY benefit and 40.8% with JSY) at
The study also examined the determinants of catastrophic expenditure on maternity. In this regard, the finding that the richer, educated, and regularly salaried women were less likely to incur catastrophic maternity expenditure is similar to the findings of previous studies conducted in India and elsewhere.9,12 It is argued that richer and educated women are often more aware about the functioning of the health system and government health schemes through their greater exposure to the mass media, and know their healthcare rights as a mother which helps them avoid making any informal payment to avail services in public health facilities. The findings revealed that the non-JSY women were several times more likely to experience catastrophic maternal expenditure compared to the JSY beneficiaries. It should sound an alarm bell for the government as this finding suggests exorbitant costs of maternity care prevailing in the private healthcare sector.
Limitations
The most apparent limitation of the study might be in collecting the household consumption expenditure. The study followed the methodology for calculating the same as guided by the National Sample Survey Organization (NSSO). NSSO used an extensive survey tool to collect the household consumption expenditure for the rounds of consumption expenditure survey which was practically not time and cost effective for an individual researcher, besides the prime motive of the survey was to collect the expenditure incurred on maternity extensively. Next, the survey relied on the reporting of expenditure by the respondents which was further cross checked by the reporting of elder member (s) of the households (who were mostly present during interviews). This was the method also applied by the NSSO in India, still one may not deny under or over reporting of expenditure by the respondents and hence could be regarded as a limitation of this study.
Conclusions
This study reveals that JSY beneficiaries are spending a substantial amount on the services that are supposed to be provided free-of-cost in public health facilities. This is a loophole in the implementation of the JSY scheme that needs to be plugged urgently to stop spillage of the JSY money. Moreover, the amount of JSY incentive should be revised taking into consideration the rise in inflation since the year 2005 when the incentive was first fixed. As women incurred a significant amount of expenditure during antenatal and postnatal care as well, the JSY incentive should be linked to prenatal and postnatal care to encourage the use of full continuum of maternity services available at public health facilities which in turn could help reduce maternity related complications and thereby expenditure as well. A significant portion of out-ofexpenditure was due to wage loss and it should be incorporated in the JSY benefit. The findings that even the JSY beneficiaries incur a huge indirect expenditure on maternity and the exiting JSY incentive can save only a limited number of households from incurring catastrophic expenditure suggests there is an urgent need to review this demand-side financing scheme.
Footnotes
Funding: SM was a recipient of University Grants Commission's (India) doctoral research fellowship for this research.
Contributions: SM designed the study, collected data, conducted the statistical analysis and wrote the manuscript. AS wrote the manuscript, contributed to the interpretation, revised the manuscript during the review process.
Conflict of interest: the authors declare no potential conflict of interest.
Acknowledgements
the authors are indebted to Dr. P.M. Kulkarni (Retired Professor, Jawaharlal Nehru University, New Delhi, India) for his valuable comments and suggestions in the paper.