
Abstract
Introduction
Maternal and neonatal death review (MNDR) introduced in Bangladesh and initially piloted in a district during 2010. MNDR is able to capture each of the maternal, neonatal deaths and stillbirths from the community and government facilities (hospitals). This study aimed to estimate the cost required to implement MNDR in a district of Bangladesh during 2010-2012.
Materials and methods
MNDR was implemented in Thakurgaon district in 2010 and later gradually extended until 2015. MNDR implementation framework, guidelines, tools and manual were developed at the national level with national level stakeholders including government health and family planning staff at different cadre for piloting at Thakurgaon. Programme implementation costs were calculated by year of costing and costing as per component of MNDR in 2013. The purchasing power parity conversion rate was 1 $INT = 24.46 BDT, as of 31st Dec 2012.
Results
Overall programme implementation costs required to run MNDR were 109,02,754 BDT (445,738 $INT $INT) in the first year (2010). In the following years cost reduced to 8,208,995 BDT (335,609 $INT, during 2011) and 6,622,166 BDT (270,735 $INT, during 2012). The average cost per activity required was 3070 BDT in 2010, 1887 BDT and 2207 BDT required in 2011 and 2012 respectively. Each death notification cost 4.09 $INT, verbal autopsy cost 8.18 $INT, and social autopsy cost 16.35 $INT. Facility death notification cost 2.04 $INT and facility death review meetings cost 20.44 $INT. One death saved by MNDR costs 53,654 BDT (2193 $INT).
Conclusions
Programmatic implementation cost of conducting MPDR give an idea on how much cost will be required to run a death review system for a low income country settings using government health system.
Significance for public health
Maternal and neonatal death review (MNDR) system in a low income county is one of the key indicators to improve quality of health care services. The MNDR also support in the reduction of maternal and newborn deaths. However, to run a comprehensive death review system need to know costs associated with the system. This is crucial in low income countries for planning and designing a public health intervention. Very few studies yet perform to look at the costs to run a death review system. This paper describes health economic cost of death review system in Bangladesh for future public health research in low income countries
Introduction
Globally, maternal and neonatal death reduction is a priority. 1 The UN millennium development goals (MDGs) 4 and 5 focused on a two thirds reduction in maternal and neonatal mortality by 2015. 2 As at 2014, Bangladesh was one of nine countries on track to achieving the MDGs. 3 However, the country is still behind in achieving maternal and neonatal death reduction by 2015. Post MDG goals, United Nations has introduced sustainable development goals (SDG) to be accomplished by 2030. 4 The government has made a tremendous effort and has already been rewarded for its progressive reduction of deaths, 5 but there is no death notification or review system for maternal and neonatal death. A maternal mortality survey has been conducted twice during 2001 and 2010.6,7 This demonstrated that there was a large increase in the number of home deliveries including those supervised by untrained birth attendants. Social factors are also one of the key contributors to deaths of mother and newborn.6,8 Maternal care-seeking rates are still low and therefore remains a challenge to the policy makers and researchers. 9
Bangladesh commenced a maternal and neonatal death review (MNDR) system for the first time in 2010. 10 The Directorate General of Health Services (DGHS) in collaboration with the Directorate General of Family Planning (DGFP) conducted the initial piloting of the intervention in the district, Thakurgaon, with technical and implementation support from two non-government organizations, the CIPRB and UNICEF, Bangladesh. The financial supports was provided by Canadian CIDA (DFATD) and initially funded by the Department for International Development (DFID) & European Commission. 10 In Africa, governments in only seven countries funded a budget for a maternal death review whereas, 18 countries received financial support from development partners. 11 The MNDR is a comprehensive package that addresses maternal deaths, neonatal deaths and stillbirth both from community and facility perspectives. 10 The framework of MPDR system in Bangladesh adopted from the World Health Organization documents.12,13 It receives notification of deaths which is then followed by verbal and social autopsy; these are used to identify medical and social causes of death. The social autopsy, through social interaction, helps the community to respond and prevent future deaths. The entire process of implementation of MNDR is performed by the field level health workers from the health and family planning department at the district and sub-district level, senior staff nurses with the support of doctors conduct the facility death reviews at government hospitals. Findings from MNDR are used by the health managers at a district and sub district level to discuss and develop action plans and implementation. The entire process of the MNDR follows a non-blaming approach while maintaining confidentiality and anonymity at each step. Following 2010, the MNDR has been continued in Thakurgaon district during 2011 and 2012. This helps the health system to respond to a death and take corrective measures to prevent future deaths. This process follows exactly that of the newly developed maternal death surveillance and response (MDSR) that WHO developed in 2013. 14
This study estimated the actual cost of the MNDR in one district during piloting and in the subsequent two years. This estimation provides empirical evidence about the actual cost of running a MNDR system or any of the activities of a MNDR.
Materials and methods
Thakurgaon district has a population of 1.4 million in five sub-districts (upazilas). 10 At the initial stage, a number of technical group discussion meetings and workshops were conducted with the professional experts from the gynaecology-obstetrics, paediatrics and public health departments. A draft of the framework was developed for implementation along with a number of tools, guidelines and a training manual for death notification, verbal autopsy, social autopsy, and facility death review. A number of committees were developed from the national level to district level and below. Those teams included the national MNDR core committee, technical group committee, district MNDR core committee, maternal and child welfare centre based MNDR committee, district hospital based MNDR committee and upazila MNDR review committee. The Directorate General of Health Services and Directorate General of Family Planning endorsed the committees, tools, guidelines, manuals and implementation framework.
Implementation of maternal and neonatal death review system
In the district, five upazila coordinators were assigned to provide technical assistance to the government. They attended an initial orientation meeting about capacity development of health staff and ensured validity and reliability of death notifications, the quality of verbal and social autopsies, and facility death review. Coordination and technical support in review meetings helped the upazila and district managers to initiate local level planning that was based on MNDR findings.
Initially, a one day training of trainers (ToT) was performed to train the upazila mangers and doctors on how to provide training on death notification for grassroots level health workers. Moreover, another two days ToT was performed to train the health managers about verbal and social autopsy. Grassroots level health workers received one day death notification training at the upazila level to notify community maternal deaths, neonatal deaths and stillbirths. Following that, a two day training was held on community verbal autopsy and a one day training on social autopsy at community level. In addition, a two day training was offered to doctors and nurses about facility death notifications and reviews.
Collection of data
Field level health workers (health assistants and family welfare assistants) in the community were assigned to certain working areas. Therefore, all areas were covered by the health workers for the notification of deaths. They used a death notification form, using community network or household visit, identified the cause of death and recorded it in the form and then returned back to the upazila health complex. 10 A verbal autopsy (VA) is performed usually after at least seven days following the death but within two weeks. The first line supervisor from the Health and Family Department is responsible for conducting the VA in the home of the deceased. 15 In addition, health workers (first line supervisor) perform the social autopsy in the village, near the deceased's house, in participation with the community people adjacent to that house. Facility death notification and review is performed at the upazila health complexes, district hospital and in maternal and child welfare centres by the senior staff nurse. In addition, medical doctors from obstetrics- gynaecology and paediatrics support the MNDR and are assigned to identify the causes of death. Monitoring takes place at the district from the national level and a review meeting platform is used for analysis of findings then an appropriate priority basis action plan is prepared and implemented.
All the data are given back to the assigned focal point in the upazila health complex and in the district hospitals. Upazila coordinators were responsible to review the quality of data. One copy of the all files are sent back to Dhaka for further review by the technical experts of the technical implementing organization, CIPRB. At all stages the economic costs of data collection were recorded.
Assign causes of death and identification of vulnerable areas
The upazila and district MNDR review meetings are used as a platform to analyse and discuss the deaths, and to prepare local action plans based on areas where maternal and neonatal deaths are high within the upazilas. Upazila managers participated in the MNDR review meetings and the discussions about the deaths. Technical support was provided by the technical research organization, CIPRB, in analysing the maternal deaths, neonatal deaths and stillbirths. Statisticians working at the upazila health complexes and upazila coordinators from the CIPRB analysed key variables (date and time of death, place of death, place of delivery) of community death notification and community verbal autopsy data locally at the upazila level.
Estimating cost
We calculated the total programme cost which includes the costs of national level meetings, development of tools and guidelines, capacity development, office set up at field sites, head office and field office expenditures, monitoring, travel and per-diem and personnel costs. During the development stage, the costs of the planning workshops at the national and district levels, and the tools finalization workshops were also included. Capacity development included the ToT about death notification and verbal/social autopsy, training of 872 grassroots level health and family planning staff about death notification, 88 first line supervisors from health and family planning department were trained on verbal and social autopsy, training of 34 doctors and nurses about facility death notification and review also took place.
Office expenditures by the head office and project field office were considered. Head office costs included rent of the office, maintenance, utilities, stationary, photocopies, phones, fax, communication, internet services, rental laptop computers and desktop computers, printers and equipment charges. At the project office cost included renting five offices in five upazilas, furniture, stationary, photocopies, and communication and internet services. Initially, the field office set up required five rental computers, one printer and accessories item, five phones with internet connection, and five rental motorcycles for the upazila coordinators. Personnel cost of project staff included five upazila coordinators and office support staff for each of five upazilas, one accountant, one data entry operator, one team leader and senior finance and admin officer, a statistician and director (part time) salaries. Stationary costs at head office and field office covered printing of different forms used in MNDR. Travel and per-diem cost covered field staff travel in the district and head office travel to do supportive supervision and monitoring in the field. The study also considered costs of monitoring the project. Here we have included expenditure of technical professionals and cost of focal persons for project implementation. These also include different stakeholders who visited Thakurgaon to see the progress of the MNDR.
Among the total programme costs, the costs for the development of tools and guidelines and capacity development were spent just for the development stage in 2010, whereas the intervention continued until 2015. Therefore, we have calculated these expenditures on a per year basis. On the other hand, we have calculated an implementation activity average cost for each of the MNDR components; these include community death notification, verbal autopsy, social autopsy, facility death notification, facility death review, and review meetings at upazila and district level. We have compared the expenditure of 2010 with the expenditure in the subsequent years (2011-2012). All monetary units were collected in Bangladeshi Taka (BDT) and then converted to purchasing power parity (PPP) adjusted International Dollar ($INT). The purchasing power parity conversion rate was 1 $INT = 24.46 BDT, as of 31st Dec 2012. Cost elements were estimated following standard cost calculation rules and guidelines.16,17 MNDR component costs were presented as average costs as per strong recommendation of Graves and colleagues who argued that No amount of statistical analysis can compensate for poor quality cost data. 18
Ethics statement
The institutional ethical review committee of the Centre of Injury Prevention and Research, Bangladesh in Bangladesh reviewed and approved the research study. The current paper has used economic data and does not use any human samples.
Results
We have calculated the MNDR cost in the first, second and third years. The cost was determined as a total programme cost and also cost as per activity (Table 1).
Programme cost of maternal and neonatal death review during 2010-2012.
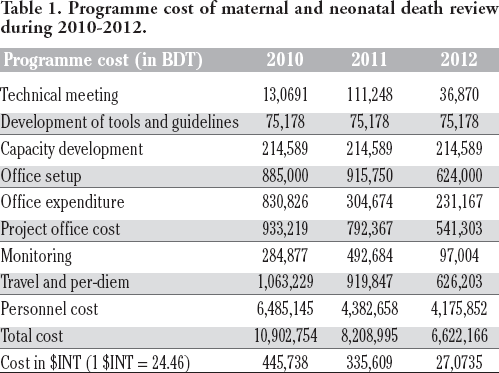
Maternal and neonatal death review cost in first year
In the piloting year, the total cost spent on implementing the programme was 10,902,754 BDT (445,738 $INT). We have calculated implementation costs for each of the activities in the field. A total of 3551 activities were conducted in the first year. The average cost of the MNDR activity in the first year was 3070 BDT (=10,902,754/3551), equivalents to 126 $INT. We have also counted average cost for each activity. Death notification at community level cost 3170 BDT (130 $INT), verbal autopsy cost 3270 BDT (134 $INT), social autopsy cost 3470 BDT (142 $INT), facility death notification cost 3,120BDT (128 $INT) and facility death review cost 3,570BDT (146 $INT) for each of the death cases whether maternal, neonatal death or stillbirth. However, to conduct the upazila MNDR review meeting cost 7,841 BDT (321 $INT) for each of the meeting, The MNDR district review meeting cost 22,510 BDT (920 $INT).
Maternal and neonatal death review cost in second year
In the second year, the total cost of implementing the programme was 8,208,995 BDT (335,609 $INT). We have calculated the implementation costs for each of the field activities. A total of 4351 activities were conducted in the second year. The average cost of an MNDR activity for year two was found 1887 BDT (=8,208,995/4351), equivalents to 77 $INT. We have also counted individual cost per activity. Death notification at community level required 1987 BDT (81 $INT), verbal autopsy required 2087 BDT (85 $INT), social autopsy required 2287 BDT (93 $INT), facility death notification required 1937 BDT (79 $INT) and facility death review required 2387 BDT (98 $INT) for each case of death whether maternal, neonatal death or stillbirth. However, the upazila MNDR review meeting required 11,944 BDT (488 $INT) for each meeting, and the district review meeting cost 24,901 BDT (1018 $INT).
Maternal and neonatal death review cost in third year
In the third year, the total expenditure to implement the programme was 6,622,166 BDT (270,735 $INT). We have calculated the implementation cost for each of the field activities. A total of 3001 activities were conducted in the third year. The average cost of MNDR activity for year three was 2207 BDT (=6,622,166/3001), equivalents to 90 $INT. We have also counted individual cost per activity. Death notification at the community level required 2307 BDT (84 $INT), verbal autopsy required 2407 BDT (98 $INT), social autopsy required 2607 BDT (107 $INT), facility death notification required 2257 BDT (92 $INT) and facility death review required 2707 BDT (111 $INT) for each cause of death whether maternal, neonatal death or stillbirth. However, to conduct the upazila MNDR review meeting cost 9709 BDT (397 $INT) for each of the meetings, and the district review meeting cost 19,914 BDT (814 $INT).
In addition, we have also described actual field costs for each of the components (Table 2). The actual field cost for the notification of community deaths was 100 BDT (4.09 $INT) to pay the health and family planning staff, verbal autopsy cost 200 BDT (8.18 $INT), social autopsy cost 400 BDT (16.35 $INT), facility death notification cost 50 BDT (2.04 $INT) and death review cost 500 BDT (20.44 $INT).
Actual field implementation cost.

During 2012 and 2013 maternal and neonatal deaths were 929 and 776 respectively at Thakurgaon district. We can assume that during MNDR implementation in 2012 with an expenditure of 8,208,995 BDT (335,609 $INT) we have saved 153 (=929-776) deaths.
Therefore, one death saved by MNDR costs 53,654 BDT (2193 $INT).
Discussion
Like other programs, the first year cost was more than second and third year to run the MNDR in the district. At the beginning, piloting required establishment costs, office set up and mobilization of more funds in monitoring (travel and per-diem). However, in the following years, establishment cost was reduced and monitoring (travel and per-diem) was optimized. At the initial stage of development of tools, guidelines, manuals of MNDR including capacity development of health staff of different tire required huge funding. The programme continued until 2015, therefore costs were calculated as cost per year, indicating the cost distribution.
Death reviews for maternal and neonatal deaths, including perinatal deaths, are undertaken in many countries worldwide. In the Asian region: Sri Lanka, Nepal, India, Pakistan, Maldives are experienced in reviewing maternal and neonatal deaths, 19 but there was no determination of economic costs for any of those death review systems. No literature about costing and performing a verbal autopsy system that analyses causes of death was found in low income country settings. 20 We have identified just one study that proposed a framework for calculating the costs for collecting vital statistics. 21 One study conducted in India found the costs for running a verbal autopsy based surveillance system for maternal mortality was 54 $INT, while it didn't cover training and infrastructure costs. 22 Another study undertaken in India reported that running a verbal autopsy based mortality surveillance system cost about 0.10 $INT per capita per year. 20 In our study, the notification of the maternal deaths, neonatal deaths or stillbirths cost decreased in 2011 in comparison to the pilot year. During initial piloting in 2010, verbal and social autopsy required more economic cost than in 2011. However, the cost of verbal and social autopsies in 2012 slightly increased in comparison to 2011 because the total number of activities was higher in 2012 than in 2011. Actual implementation cost was only 100BDT (4.09 $INT) for community death notification. To review death in the community required 200 BDT (8.18 $INT). In Africa, a study has shown that external funding sources from developmental partners are crucial to run maternal death review and scale up. The study has also indicated that scarcity of government funding has influence in programme implications. 11 Our study demonstrates that to capture a death in the community followed by performing a death review requires only a small amount of fund. The small amount of money can be easily supported by either that government or by the developmental partners for the improvement of overall maternal and neonatal health. One maternal and neonatal death saved by MNDR costs 53654 BDT (2193 $INT). This should be considered for Bangladesh because there are still significant numbers of deaths occurring in the community which do not present to hospitals or medical centres and therefore the information for those deaths is missing. It is important that the information is collected to estimate maternal mortality ratio and neonatal mortality rate and it also helps to initiate appropriate intervention based on death review findings. The MNDR is comprehensive because it covers the entire spectrum of a death review from its notification to the end using reviews and discussing findings followed by implementation of specific action. The cost for this included costs related to the programme establishment as well as the implementation of the different components of the MNDR. Cost effectiveness and economic cost was calculated for disease related intervention but no costs have been calculated to implement the maternal and neonatal death review system. The present study has provided assumptions about how much such a programme will cost within a government health system. Most importantly the study has indicated how much MNDR costs to save one death. We should keep note that MNDR was at the beginning phase in Bangladesh. When MNDR will continue for couple of more years the cost per death saved could be lower. The average costs of MNDR elements such as community death notification, conducting of verbal autopsy, social autopsy, facility death notification and review meetings are not so high which provide a clear invitation from the policy makers to scale up the program. Therefore, in low income country settings, we suggest that it is worth implementing such an intervention, even a smaller scale one that might cover any of the components of the MNDR.
The study has used existing costs to estimate, retrospectively, the costs of running such a programme. This was a pilot and therefore, the cost elements estimated in the study are from just one district. A broader study that covered a larger population may provide a different estimate of costs. However, we would anticipate these to be lower due to system costs being shared across districts.
Conclusions
Initial costs of initiating a program are always high. However, program implementation costs decrease over time as establishment costs reduce and monitoring (travel and per-diem) is optimized. There was a large one-off cost of the initial development of tools, guidelines, manuals, and the MNDR framework in addition to capacity development of health staff. The MNDR system is urgently needed in Bangladesh to reduce maternal and neonatal deaths. We believe that the costs of death notifications, followed by death reviews are not so high and are important for the country. This study has provided empirical evidence about the actual cost of running a MNDR system and any of the activities of MNDR. Based on the death review findings, effective local level planning can reduce future deaths to achieve the sustainable development goal by 2030.
Footnotes
Acknowledgements
The authors would thank the Directorate General of Health Services (DGHS) and Directorate General of Family Planning (DGFP), Ministry of Health and Family Welfare (MOHFW) of Government of the People's Republic of Bangladesh for implementing Maternal and Neonatal Death Review under a joint GoB-UN Maternal Neonatal Health Initiatives. We are also grateful to UNICEF, Bangladesh for providing technical and financial support via Canadian CIDA (DFATD) and the Department for International Development (DFID) and European Commission (EC) to initiate the pilot study. Finally, we are thankful to Dr. Toity Deave, Assoc. Prof. for Family and Child Health at University of the West of England, Bristol for editing the English language of the manuscript. Contributions; AB and KD planned the study; AB, AH, FR performed the study; AB, KD, analysed data; all authors wrote the paper; CE, AH and KD critically reviewed the paper.
Conflict of interest: the authors declare no conflict of interest.