
Abstract
Background
Antiviral and immune-modulating properties of low-molecular-weight heparin (LMWH) against Coronaviridae have been reported by in vitro studies, but no in vivo evidence is yet available. We sought to know whether the timing of prophylactic doses of LMWH during the course of COVID-19 may affect the time to SARS-CoV-2 nasal-oropharyngeal swab negativization.
Methods
Retrospective monocentric cross-sectional study on patients requiring sub-intensive ward admission due to first SARS-CoV-2 infection and undergoing early (EH; within 7 days from COVID-19 signs and symptoms onset) versus delayed prophylactic LMWH (DH; after 7 days). SARS-CoV-2 RNA was measured by reverse transcription real-time PCR according to scheduled time points: first swab after 2 weeks from COVID-19 onset, then at 1-week intervals until negativity.
Results
Time to SARS-CoV-2 swab negativity was shorter in EH (38 patients) compared with DH (55 patients): 22 versus 37 days (P=0.004). The number of confirmative negative swabs in EH was significantly higher compared with DH at week 2 (21.1% versus 3.6%; P=0.017) and 4 (60.0% versus 19.6%; P<0.001). At univariate, EH differed from DH for several disease severity and clinical management parameters. Nevertheless, after accounting for the differences, Cox regression showed early LMWH administration (hazard ratio [HR] 2.91 [1.51, 5.63]; P=0.002) and higher lymphocytes nadir (HR 1.04 [1.01, 1.08]; P=0.020) as predictors of shorter time to swab negativity.
Conclusions
This potential antiviral and/or immune-modulating activity of LMWH needs further in vivo confirmations by randomized controlled trials.
Introduction
After almost 1 year from the first COVID-19 cases, deaths are still increasing, while the number of drugs with proven benefits is not. As long as the results of randomized clinical trials are not available, the debate surrounding the true effectiveness of several drugs, such as of azithromycin or hydroxychloroquine in SARS-CoV-2 infection will likely continue [1]. From this chaotic scenario, heparin is emerging as one of the few drugs with a proven positive impact upon the clinical outcomes of patients suffering from COVID-19. Indeed, with undoubted anticoagulant activity, heparin use has been associated with a reduced mortality among patients at elevated risk of the thrombotic complications of this ‘viral coagulopathy’ [2,3]. Nevertheless, based on in vitro data, different other activities have been allegedly postulated for heparins: antiarrhythmic, anti-inflammatory, immune-modulating and antiviral [4–7]. Regarding the latter, heparins could potentially reduce virion adhesion to host cells through several mechanisms (Figure 1): by destabilizing the bond between ACE2 receptor and the receptor-binding-domain of SARS-CoV-2, by inhibiting several proteases that cleave SARS-CoV-2 spike proteins, and by competing with cell-surface heparan sulphate, essential for the viral docking to human cells [4,5,7]. Thereby, heparin may eventually hamper SARS-CoV-2 infectivity and replication, as already hypothesized and observed in preliminary studies on cell cultures exposed to other human coronaviruses [4,8]. Considering the physio-pathological dynamics of COVID-19, heparins may express these further advantages more effectively when administered early in the disease course [6]. Notwithstanding, type and doses of heparins aimed at exploiting these possibilities are once again a matter of debate, as these properties probably related to the molecular structure of different heparins and other factors [7].

Potential antiviral properties of low-molecular-weight heparins in SARS-CoV-2 infection
Aim of our study was to assess whether the timing of administration of prophylactic low-molecular-weight heparins (LMWH) dose during the course of COVID-19 may affect the time to SARS-CoV-2 nasal-oropharyngeal swab (NPs) negativization.
Methods
We retrospectively reviewed data from SARS-CoV-2-positive patients admitted to the Infectious Diseases wards (Amedeo di Savoia Hospital, Turin, Italy) between March and June 2020 that consented to data collection and that underwent prophylactic doses of LMWH adjusted for renal function and body weight until discharge/death, as previously detailed [3]. We excluded patients with previous hospitalization for COVID-19 in other wards before referral to ours or previously diagnosed with COVID-19 that required further admissions due to clinical or virological SARS-CoV-2 relapses. SARS-CoV-2 NPs were tested by an in-house reverse transcription real-time PCR according to Corman et al. [9] with the first NPs scheduled after 2 weeks (±3 days) from COVID-19 onset, then at 1-week intervals (±3 days) until swab negativity (two negative NPs 24 h apart). Anti-SARS-CoV-2 S1/S2 IgG were measured by chemiluminescence (Diasorin, Saluggia, Italy) from 1 May and clinically driven schedules. Patients were classified into early LMWH administration (EH; within 7 days from COVID-19 signs and symptoms onset) versus delayed (DH; after 7 days). Mann–Whitney, Kruskal–Wallis, Spearman's correlation and survival analyses were performed (SPSSv26; IBM, Armonk, NY, USA). Variables showing univariate P≤0.10 were included in the Cox regression (entering method). Continuous variables are presented as median (interquartile range), while categorical data as absolute number (proportion). The protocol conforms to Helsinki Declaration and was approved by ‘Città della Salute e della Scienza’ Ethics Committee (protocol 00304/2020).
Results
A total of 93 patients were included. 67.7% were male. The median age, the ratio of arterial oxygen partial pressure (mmHg) to fractional inspired oxygen (P/F ratio) nadir, serum creatinine nadir and platelet count nadir were 68 years (60–80), 225 (127–321), 1.02 mg/dl (0.88–1.24) and 166,000 cells/mm3 (133,500–213,250), respectively. 24 patients both underwent CPAP/reservoir and Venturi mask, 5 intubation, while the others were on low-flow wall-oxygen (24) and ambient air (16). 11 deaths occurred, of which 8 were COVID-19-related. The median time from COVID-19 signs and symptoms onset to hospitalization, prophylactic LMWH start, first positive serology (available for 45 patients, 48.4%) and SARS-CoV-2 NPs negativity were 6 (2–9), 8 (4–12), 32 (15–45) and 33 days (21–41; 4 patients were still swab-positive when writing this report and 8 died swab-positive), respectively.
Compared with DH (55), EH (38) showed shorter times from COVID-19 onset to hospitalization (3 versus 9 days; P<0.001), to NPs negativity (22 versus 37 days; P=0.004) and to the first positive serology (16 versus 35 days; P=0.043; Table 1). As shown in Table 1, EH were characterized by lower first-determination of anti-S1/S2 IgG titres, higher nadir of lymphocytes and of P/F ratio and by a larger proportion of patients that underwent remdesivir and a smaller one that required ventilation supports other than none or low-flow wall-oxygen (44.7% versus 65.4%; P=0.048), anti-inflammatory drugs and corticosteroids. At week 2 and 4 from COVID-19 onset, higher proportions of patients in EH were confirmed swab-negative: 21.1% versus 3.6% at week 2 (odds ratio [OR] 0.14 [0.028,0.71]; P=0.017) and 60.0% versus 19.6% at week 4 (OR 0.16 [0.062,0.43]; P<0.001; Table 1). In accordance with the evolution of clinical practice during the pandemic, patients admitted in May–June were more likely to belong to EH compared with those admitted previously (63.4% versus 36.6%; P<0.001). No other significant differences were observed (Table 1).
Comparison of demographic, clinical, laboratory and viro-immunological features of patients starting low-molecular-weight heparin within versus after 7 days from COVID-19 onset

Continuous variables are presented as median (IQR).
Antivirals included: 27 lopinavir/ritonavir, 59 hydroxychloroquine and 15 remdesivir.
Anti-inflammatory drugs included: 1 ruxolitinib, 2 imatinib, 35 tocilizumab. COVID-19, novel coronavirus 2019 disease; CPAP, continuous positive airway pressure support; DH, delayed low-molecular-weight heparin administration group; EH, early low-molecular-weight heparin administration group; IL-6, interleukin 6; LMWH, low-molecular-weight heparins; P/F ratio, arterial pO2/fraction (%) of inspired oxygen ratio.
The time from COVID-19 onset to NPs negativity correlated with that to LMWH start (ρ=0.48, P<0.001) and to the first positive serology (ρ=0.66, P<0.001), and with the lymphocytes nadir during the hospitalization (absolute number; ρ=-0.28, P=0.012; percentage: ρ=-0.31, P=0.006).
Log-rank analysis was performed confirming a significant difference in the time to NPs negativity in favour of EH compared to DH (Mantel–Cox P<0.001). The Kaplan–Meier curve is shown in Figure 2. At the Cox proportional-hazards model (χ2 P=0.007) that included age, most intensive type of oxygen support, anti-inflammatory, remdesivir and corticosteroid use, admission period (early versus late pandemic) and time to hospitalization, lymphocytes nadir (HR 1.04 [1.01,1.08]; P=0.020) and LMWH administration within the first week from COVID-19 onset (HR 2.91 [1.51,5.63]; P=0.002) independently associated with shorter times to SARS-CoV-2 NPs negativity (Table 2). The corresponding regression curve is shown in Figure 2.
Cox proportional hazards model for SARS-CoV-2 nasal-pharyngeal swab negativity
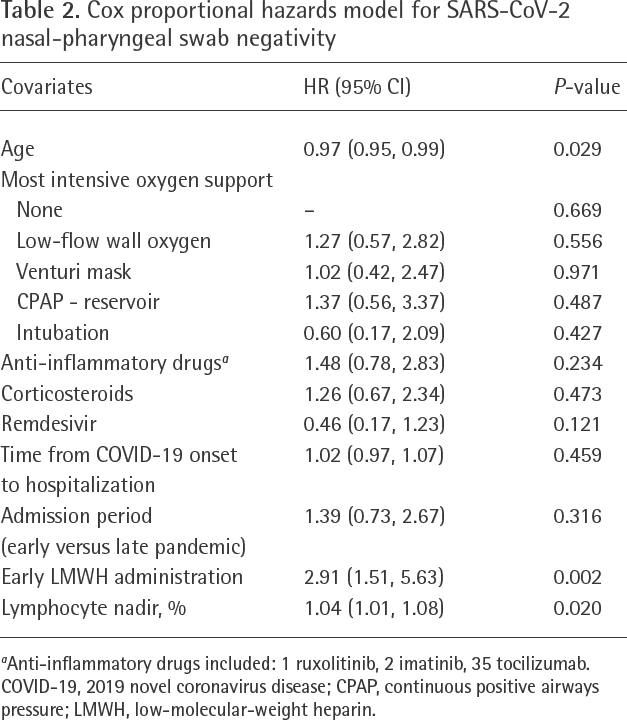
Anti-inflammatory drugs included: 1 ruxolitinib, 2 imatinib, 35 tocilizumab. COVID-19, 2019 novel coronavirus disease; CPAP, continuous positive airways pressure; LMWH, low-molecular-weight heparin.
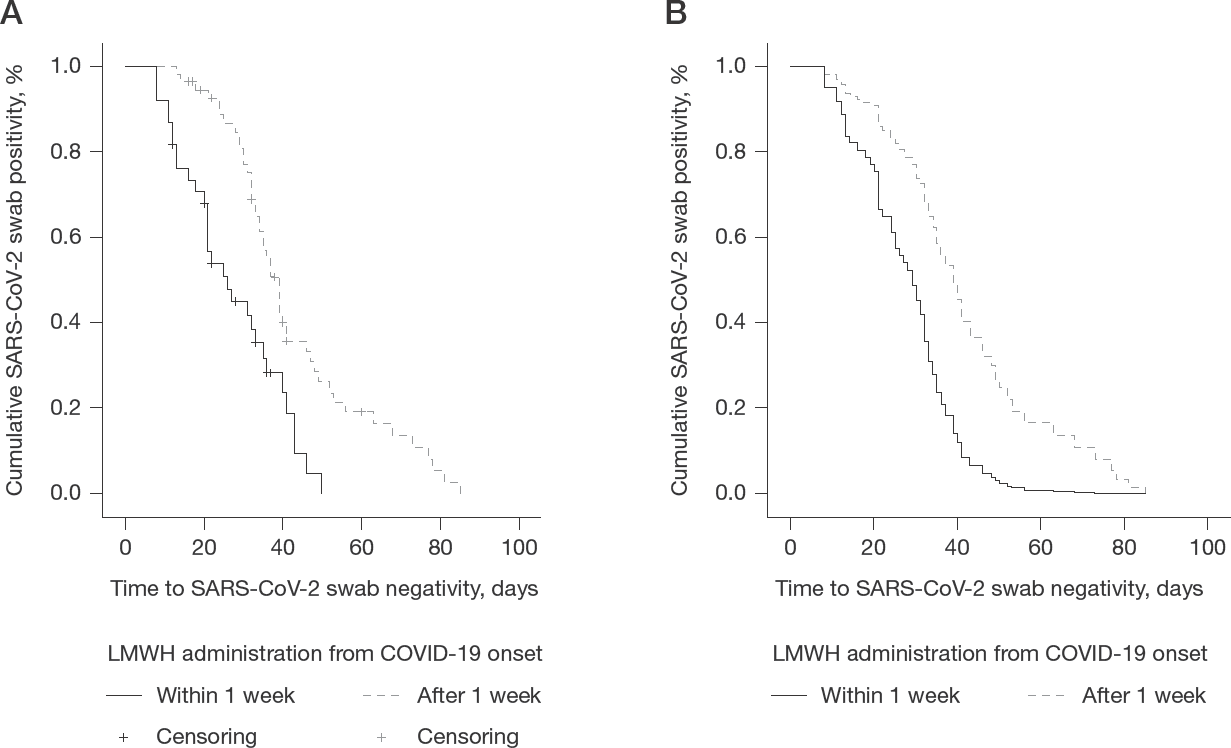
Difference in time to SARS-CoV-2 negativity at nasal-pharyngeal swab between early and delayed low-molecular-weight heparin group
Discussion
We observed a significant shorter time to in SARS-CoV-2 swab negativity (15 days) among patients starting prophylactic doses of LMWH within 7 days from COVID-19 onset compared with those starting LMWH later during the disease course, with about 5 and 3 times more confirmative negative NPs in EH compared with DH at week 2 and 4, respectively. Even after accounting for other determinants potentially able to affect viral shedding from the upper respiratory airways, SARS-CoV-2 NPs were almost 3 times more likely to become negative among patients that started LMWH within the first week from COVID-19 onset compared with those that received LMWH later on.
To the best of our knowledge, this finding may represent the first in vivo evidence of a potential antiviral and/or immune-modulating activity of LMWH in COVID-19. However, this putative effect warrants further validation against an untreated control group. Moreover, much has been affirmed and then retracted about this infection. Firstly, we have not taken into account the amount of viral load at the diagnostic swab so that we were not able to adjust our results for viral kinetics. Age has been linked to the amount of virus in the upper respiratory airways and was therefore included in our model to partially and indirectly adjust for this factor [10]. Secondly, corticosteroid type, specific doses and administration timing were extremely heterogeneous during the first COVID-19 wave and not taken into account in our analysis as well as possible delays in other drug administration; all of these factors may affect viral shedding dynamics [11–13]; further studies are required to provide data on how to interpret the effect of steroids upon SARS-CoV-2 kinetics. Furthermore, serology was available in 45 patients only, all belonging to the later phase of the pandemic. Analyses including serological data were performed to assess possible confounding, but the lower IgG titres among EH highlights the clinically driven timing of this test, differently from the scheduled NPs, so that, while our preliminary results may point towards a potential positive effect of LMWH also upon anti-SARS-CoV-2 neutralizing antibodies development, tailored prospective studies should address the phenomenon.
An extensive and deeper knowledge in SARS-CoV-2 life cycle and immunity, as well as in treatment-, laboratory- and host-related factors able to affect NPs results are required to confirm the validity of our model firstly and eventually of our observation.
The implications and confirmation of our preliminary results could potentially help at reaching a consensus on several unanswered questions regarding the management of new COVID-19 patients while waiting for the results of several ongoing randomized clinical trials. First, balancing benefits and risks, home LMWH prescription could reduce infectivity and transmission within households, one of the settings at the highest risk of SARS-CoV-2 transmission [13,14], and could potentially prevent clinical deteriorations regardless of antithrombotic effects among SARS-CoV-2-positive patients not requiring hospitalization [15,16]. However, infectivity of patients after about 10 days from the onset of mild to moderate COVID-19 has been recently questioned [17,18], leaving uncertain the possible favourable impact of LMWH on the transmission containment. Whether viral inoculum predict disease severity is also a matter of current debate [19,20]. If this association was definitively confirmed and LMWH proved to accelerate viral load decay from the upper respiratory airways, LMWH use could impact on both disease transmissibility and severity among secondary cases. On the other hand, LMWH continuation could be indicated for hospital-discharged patients with still positive NPs. Secondly, our data could add further evidence in favour of switching to heparins from oral anticoagulants [21]. Thirdly, pharmacology research should be urged to design new heparin-derived molecules with expanded proportions of low-affinity chains, which most likely contribute to the alternative properties of heparins [7]. Lastly, considering that antiviral and immune-modulating mechanisms of LMWH potentially may act transversely across the Coronaviridae family [1,4,8], further confirmations to our preliminary data may guide clinical and public health decision making in the current pandemic and in its recrudescence, as well as in outbreaks of future emerging coronaviruses.
In conclusion, early prophylactic doses of LMWH in COVID-19 patients in a sub-intensive ward associated with a significantly shorter time to NPs viral undetectability compared with delayed administration; other exploratory benefits of early LMWH administration were observed but need to be con-firmed prospectively.
Footnotes
Acknowledgements
This work was supported by internal funding. We are grateful to the patients and their family as well as all the professionals working at our Infectious Diseases Clinic, Amedeo di Savoia Hospital (Turin, Italy) for having faced these hard times with strength and unity.
The authors declare no competing interests.