
Abstract
Background
In China, the optimal management of individuals living with chronic HBV infection (CHB) remains an unmet need. The EVOLVE Study was a 5-year prospective, longitudinal, observational study that compared the clinical outcomes in treatment-naive CHB patients receiving entecavir (ETV) or lamivudine (LAM)-based therapies.
Methods
Males or females aged ≥18 years, diagnosed with CHB regardless of cirrhosis or hepatitis B e antigen (HBeAg) status were enrolled from tier 2 city hospitals (between 2012–2014). The choice of initial therapy and subsequent treatment modifications was at the discretion of treating physicians. Key outcomes included treatment modifications, virological response (HBV DNA <300 copies/ml) and HBV disease progression.
Results
Of the 3,408 patients enrolled, 1,807 and 628 received ETV and LAM-based therapy, respectively. The mean age was 39.5 years, 74% were male and 22.9% had cirrhosis. The rate of treatment modification was higher in the LAM-based versus ETV group (25.9% versus 13.7%); viral breakthrough was the most common reason in the LAM-based group versus financial reasons in the ETV group. At week 240, the virological response rate was 73% in both treatment groups. Compared with LAM-based therapy, ETV was associated with a significantly lower incidence of viral breakthrough (12.6% versus 2.1%) and genotypic resistance (10.1% versus 1.2%; P<0.0001 for both); significantly lower risk of HBV disease progression (14.0% versus 10.7%; P=0.0113); and lower rates of progression to decompensated cirrhosis (9.6% versus 6.4%) and hepatocellular carcinoma (1.9% versus 0.8%).
Conclusions
This real-world, longitudinal study demonstrated a significantly lower risk of HBV-related disease progression, viral breakthrough and resistance with ETV versus LAM-based therapy. ClinicalTrials.gov NCT01726439.
Introduction
China has the largest burden of HBV infection worldwide, affecting more than 70 million people and accounting for 27% of the global prevalence [1,2]. While the childhood HBV vaccination programme in China has reduced the incidence of HBV infection in children <5 years old by 97% [3], reducing progressive liver disease in those already living with chronic HBV infection remains a challenge [1].
Maintaining suppression of HBV DNA levels with nucleoside/nucleotide analogue (NA) therapy has been strongly associated with reduced risk of disease progression and long-term adverse outcomes of chronic HBV infection [4,5]. NA therapies with a high barrier to HBV resistance such as entecavir (ETV) or tenofovir (TDF) are preferred options in treatment-naive patients with chronic hepatitis B (CHB) [6], whereas therapies with a lower barrier to HBV resistance, such as lamivudine (LAM), adefovir dipivoxil (ADV) and telbivudine (LdT) are not recommended as a first-line therapy. In particular, ETV therapy has been shown to provide high rates of virological response, normalization of alanine aminotransferase (ALT) levels and histological improvements in patients with CHB [7,8]. Furthermore, the current Asian Pacific Association for the Study of the Liver guidelines do not recommend de novo combination of two NA therapies with the same resistance patterns [6]. Despite the major guidelines, including the Chinese clinical treatment guidelines, recommending the use of ETV or TDF or interferon as first-line therapy, until recent years many LAM-based therapies had been widely used in clinical practice especially in low-tier cities due to their affordability. Data from the China Registry of Hepatitis B (CR-HepB) showed that in 2012 ETV, ADV, LAM, LdT and TDF accounted for 29.0%, 33.3%, 27.6%, 9.7% and 0.4% of the NA therapy, respectively, in patients with CHB [9]. In 2016, the corresponding rates were 51.2%, 16.1%, 18.8%, 12.5% and 1.4%, respectively [10].
The World Health Organization has set the goal of eliminating hepatitis B as a public health threat by 2030 by reducing new infections by 90% and mortality by 65%, as well as increasing the diagnosis to 90% of infected people and antiviral treatment of 80% of eligible patients [1]. Currently, there are significant gaps in achieving the target CHB-related mortality reduction due to under-diagnosis and under-treatment of patients with chronic HBV infection. In an epidemiological survey in north-eastern China, only 16.5% of patients reported as hepatitis B surface antigen (HBsAg)-positive had previously been diagnosed [11]. Furthermore, a modelling study estimated that only 11% of about 32 million treatment-eligible patients with chronic HBV infection in China receive treatment [12]. Therefore, there is high unmet need for improving the diagnosis and treatment rates of chronic HBV infection. Data on treatment patterns and long-term effectiveness of different NA therapies would inform clinicians about the effective management of CHB and provide guidance on optimizing the treatment of patients with CHB in China.
We therefore conducted the EVOLVE study, a multicentre, prospective, longitudinal, observational study of treatment-naive patients with CHB receiving ETV or LAM-based treatment regimens (LAM mono-therapy, LAM+ADV, de novo or sequential combination therapy) in 63 tier 2 city hospitals in China. We previously reported 52-week results, which showed a significantly higher rate of virological response for ETV therapy compared with LAM-based therapy (77.0% versus 61.4%; P<0.0001) [13]. Here we present data on treatment patterns, virological response, resistance and clinical outcomes for ETV and LAM-based treatment regimens from the 5-year follow-up of the EVOLVE study.
Methods
Participants and Study Design
The study design has been published previously [13]. Briefly, the EVOLVE study was a prospective observational study with a 5-year follow-up of antiviral treatment-naive patients with CHB enrolled from tier 2 city hospitals in China (63 centres participated in the 2-year study and 48 centres participated in the 3-year extension). Eligible patients were males or females aged ≥18 years, diagnosed with CHB with or without compensated cirrhosis (defined by current Chinese guidelines: Child-Turcotte-Pugh [CTP] A, evidence of hepatocellular dysfunction or portal hypertension or histologically consistent with diagnosis of cirrhosis but without esophagogastric variceal bleeding [EGVB], ascites or hepatic encephalopathy), HBeAg-positive or negative, and NA treatment-naive (based on patient self-reporting). Key exclusion criteria included coinfection with HCV, decompensated cirrhosis, liver failure, hepatocellular carcinoma, any other type of malignancy, interferon-based therapy within 6 months prior to screening or confirmed pregnancy. No additional restrictions for inclusion or exclusion were employed to ensure that the enrolled patients are representative of the real-world population in China. All enrolled patients provided written informed consent for participation in the study.
There was no protocol-driven treatment of enrolled patients; the choice of initial NA therapy and subsequent treatment modifications were at the treating physician's discretion. Patients were enrolled between 2012 and 2014; at that time, four NA therapies were available in China: ETV, LAM, ADV and LdT. The primary objective of this study was to compare the long-term clinical outcomes with ETV monotherapy and LAM-based regimens (LAM monotherapy, LAM and ADV combination at treatment initiation or addition within 48 weeks) in treatment-naive patients with CHB.
Study visits and assessment schedules followed local clinical practice guidelines for CHB. For treatment-naive patients, Chinese guidelines recommend a monthly follow-up during the first 3 months after treatment initiation, followed by quarterly visits based upon the patient's clinical condition. Clinic visits were scheduled at weeks 24, 48, 72, 96, 144, 192 and 240. Additionally, three telephone follow-ups were scheduled at weeks 120, 168 and 216. Assessments at each site visit included: HBV DNA, HBeAg, anti-HBeAg, HBsAg, anti-HBsAg, HBV-related complications, treatment modifications (termination of NA treatment, reasons for termination, addition or switching of NA therapy) and compliance [14]. The following data were collected at each telephone follow-up: EQ-5D responses, treatment modifications and clinical outcomes. Abdominal ultrasounds, liver biopsy or liver stiffness measurements (Fibroscan) were performed every 6–12 months. HBV DNA testing was performed at a central laboratory at baseline, and weeks 48 and 96 (Roche COBAS; lower limit of detection: 20 IU/ml). At all other site visits, HBV DNA levels were tested at the participating hospitals.
Patients who experienced virological breakthrough (increase in HBV DNA serum levels of 1-log10 [10-fold] above the nadir of the virology response while on continuous treatment) and/or suboptimal response (reduction in HBV DNA level by ≥2 log10 IU/ml from baseline, but detectable levels of HBV DNA) during the study period were tested for HBV genotypic mutations in the central laboratory at the treating physician's discretion.
All adverse events (AEs) and serious AEs (SAEs) were documented and causality with study treatment was assessed by the treating physician.
The study was conducted in accordance with the International Society for Pharmacoepidemiology Guidelines for Good Epidemiology Practices and applicable regulatory requirements. Institutional Review Board approval was obtained prior to study initiation.
Ethical approval: all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Outcomes
The primary study end point was the proportion of patients who achieved virological response (HBV DNA <300 copies/ml) with ETV monotherapy compared with LAM-based therapy after 48 weeks of treatment (reported elsewhere) [13]. Here we report long-term data at 5-year follow-up for the following outcomes by treatment group: treatment modifications; virological response; mean HBV DNA reductions; HBeAg and HBsAg clearance rates; HBeAg and HBsAg seroconversion rates; viral breakthrough and genotypic resistance; liver-related events of HBV disease progression (defined as changes from baseline disease diagnosis: from CHB to compensated cirrhosis, from CHB to decompensated cirrhosis, from compensated cirrhosis to decompensated cirrhosis, and incidence of hepatocellular carcinoma, hepatic failure or liver-related death). For the assessment of HBV disease progression, CTP scores (for patients with cirrhosis) were collected at each follow-up site visits, and abdominal ultrasounds, liver biopsy or liver stiffness measurements (Fibroscan) were performed every 6-12 months during the follow-up.
Statistical analysis
The full analysis set (FAS) comprised patients who received ≥1 dose of NA therapy and had data post-enrolment. The FAS was used for baseline clinical characteristics and all efficacy assessments except virological response, which was assessed in the efficacy analysis set (EAS). The EAS included enrolled patients who received ≥1 dose of NA therapy and had HBV DNA data within +6 weeks of the final visit. For the EAS, if a patient missed the week 44 visit and HBV DNA was undetectable at weeks 20 and 68, the patient was regarded as HBV-DNA-negative at week 44. Patients who received any type of treatment modification remained in their initial treatment group for outcome analyses. The safety set included enrolled patients who received ≥1 post-baseline dose of NA treatment.
HBV DNA and the virological response were compared between treatment groups using linear and logistic (respectively) regression models to adjust for potential influencing factors in the study population. The probabilities of HBV disease progression, virological breakthrough and genotypic resistance were analysed using the Kaplan-Meier method; cumulative rates were compared using the log-rank test.
Categorical data were compared using χ 2 or Fisher exact tests. Continuous variables with normal distributions were compared using the Student's t-test or analysis of variance. Continuous variables without normal distribution were compared using non-parametric tests. Significance was defined as P<0.05 for all two-tailed tests. Multivariate logistic regression analysis was conducted to identify independent predictors of virological response; estimates of the odds ratio, P-values and two-sided 95% confidence interval were calculated.
Results
Patient disposition and baseline clinical characteristics
A total of 3,434 patients were enrolled in the study. Of these, 3,408 were included in the FAS population: ETV (n=1,807), LAM-based (n=628), LdT (n=791), ADV (n=157) and other de novo combinations (n=25). 2,562 patients completed the 2-year study and 1,597 patients were enrolled in the 3-year extension phase. The EAS population (patients with HBV DNA data at baseline and week 240) included 709 patients (Figure 1). A total of 2,561 (75.1%) patients completed treatment; among patients who did not complete the study treatment (n=847; 24.9%) the most common reasons for treatment discontinuation were lost to follow-up, 342 (40.4%); withdrawal of informed consent, 254 (30%); AEs, 37 (4.4%); migration, 19 (2.2%); protocol deviation, 16 (1.9%); and lack of efficacy, 1 (0.1%).

Patient disposition during the study
Baseline clinical characteristics are summarized in Table 1. The mean (standard deviation) age was 39.5 (11.7) years and 2,515 (73.8%) were male. Most patients (77.1%) presented with a diagnosis of CHB without cirrhosis and 22.9% had cirrhosis. The mean duration of CHB was ≤6 years in 1,592 (46.7%) of patients and 2,057 (60.4%) presented as HBeAg-positive; 4.6% of patients had received prior interferon therapy. In general, baseline characteristics were comparable across the different treatment groups.
Baseline demographic and disease characteristics

Data are n (%) or mean ±
Values are non-cirrhosis subgroup from Child-Turcotte-Pugh score group. ADV, adefovir; ALT, alanine aminotransferase; BMI, body mass index; CHB, chronic hepatitis B; ETV, entecavir; FAS, full analysis set; HBeAg, hepatitis B e antigen; LAM, lamivudine; LdT, telbivudine; ULN, upper limit of normal.
Treatment modifications and compliance
A total of 648 patients (19.0%) reported ≥1 treatment modification, with a higher proportion in the LAM-based group versus the ETV group (25.9% versus 13.7%; Supplementary Table 1 in Additional file 1). The most common type of treatment modification in patients who started with ETV was to switch to another treatment (137/247; 55.5%); the main reason cited was financial means (68.0%) whereas viral breakthrough accounted for 6.3% of treatment modifications. Patients treated with LAM monotherapy were equally likely to switch (39/131; 29.8%) or have treatment add-on (39/131; 29.8%); the primary reason was viral breakthrough (55.2%).
For patients starting with LAM+ADV combination therapy, about half of the treatment modifications involved switching to another treatment (15/32; 47%); financial means and viral breakthrough accounted for treatment modification in 38% and 17% of patients, respectively (Supplementary Table 1 in Additional file 1). In the LdT group, 25.4% (n=201) of patients had at least one treatment modification and the primary reason was viral breakthrough (71/201; 42%).
A total of 221 patients reported at least one episode of non-compliance (missing 10% dosing per month), including 106 patients (5.8%) in the ETV group, 40 (6.3%) in the LAM-based group, 66 (8.3%) in the LdT group, 8 (5.0%) in the ADV group and 1 (4.0%) in other de novo combination group.
Virological response
A significantly higher proportion of patients in the ETV group achieved the primary end point (virological response at week 48) compared with the LAM-based group (925/1,190 [77.7%] versus 252/400 [63.0%]; P<0.001; Supplementary Table 2 in Additional file 1). A significant difference between treatment groups was maintained at week 96 (1,064/1,258 [84.6%] versus 277/426 [65.0%]; P<0.001). At week 240, the virological response rate was 73% in both the ETV (276/380) and LAM-based (101/139) groups (P= not significant; Table 2). Similar results were observed for the LdT group, with virological response rate of 73% at week 240. The analysis at week 240 is based on a subset of patients with HBV DNA data available at baseline and at week 240 and who did not have antiviral resistance.
Summary of treatment effectiveness at week 240

Virological response (defined as HBV DNA <300 copies/ml) was analysed in the efficacy analysis set (EAS) population, which comprised patients who received ≥1 dose of nucleoside/nucleotide analogue (NA) therapy and had HBV DNA data at baseline and at week 240. All other efficacy outcomes were analysed in the full analysis set (FAS) population, which comprised patients who received ≥1 dose of NA therapy and had data post-enrolment. ADV, adefovir; ETV, entecavir; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; LAM, lamivudine; LdT, telbivudine.
In a multivariate logistic regression analysis, the age group ≥40 and <50 years (versus <40) was a negative predictor and total bilirubin of >1 and ≤3xULN (versus ≤ULN) was a positive predictor of virological response at week 240 (Supplementary Table 3 in Additional file 1).
Summary for liver-related events of HBV disease progression before week 240 a
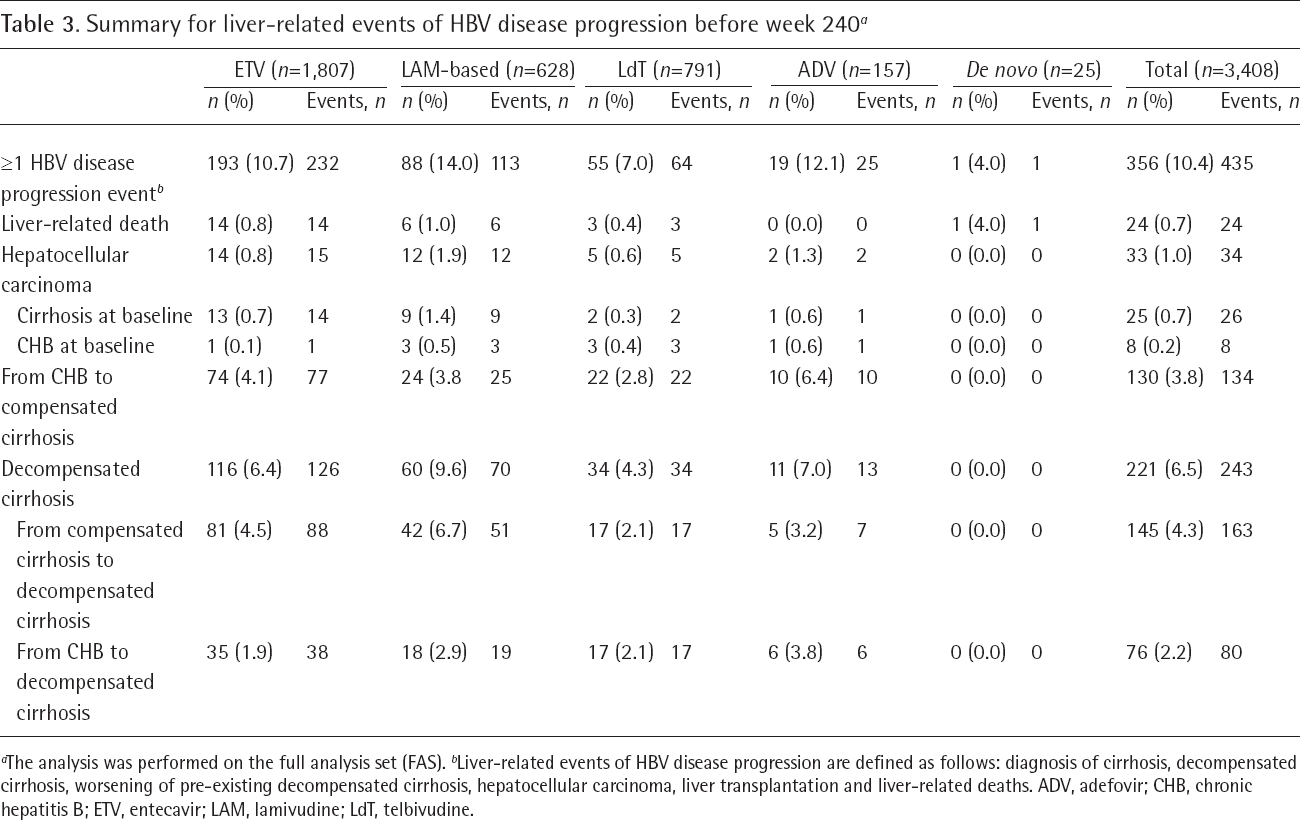
The analysis was performed on the full analysis set (FAS).
Liver-related events of HBV disease progression are defined as follows: diagnosis of cirrhosis, decompensated cirrhosis, worsening of pre-existing decompensated cirrhosis, hepatocellular carcinoma, liver transplantation and liver-related deaths. ADV, adefovir; CHB, chronic hepatitis B; ETV, entecavir; LAM, lamivudine; LdT, telbivudine.
Mean HBV DNA reductions
At week 48, the mean HBV DNA reduction was -4.86 log10 copies/ml in the ETV group and -4.24 log10 copies/ml in the LAM-based group (Supplementary Table 4 in Additional file 1). HBV DNA reductions were maintained at week 96 in the ETV and LAM-based treatment groups (-4.96 versus -4.38 log10 copies/ml, respectively). Similar results were observed in the LdT group, with mean HBV DNA reductions of -4.8 and -4.7 log10 copies/ml at weeks 48 and 96, respectively.
Serological response
Among patients who were HBeAg-positive at baseline, 482/1,051 (45.9%) patients in the ETV group and 193/370 (52.2%) in the LAM-based therapy group achieved HBeAg clearance during the study period. A total of 263/1,051 (25.0%) in the ETV group and 84/370 (22.7%) in the LAM-based group achieved HBeAg seroconversion during the study. In a multivariate logistic regression analysis, treatment modifications for financial reasons (versus no modifications) and higher baseline HBV DNA levels were negatively associated with HBeAg clearance or seroconversion at week 240 (Supplementary Table 5 in Additional file 1).
Overall, 29 (1.6%) and 16 (2.6%) patients in the ETV and LAM-based groups, respectively, achieved HBsAg clearance during the study period. HBsAg seroconversion was achieved in 20 and 11 patients in the ETV and LAM-based therapy, respectively, during the follow-up. At week 240, serological response was comparable between the treatment groups and is presented in Table 2.
For the LdT group, 281/562 (50.0%) achieved HBeAg clearance and 178/562 achieved HBeAg seroconversion during the study period. The corresponding rates for HBsAg clearance and seroconversion were 16 (2.0%) and 12 (1.5%) patients, respectively.
Viral breakthrough and genetic resistance
The cumulative incidence of viral breakthrough was significantly lower in the ETV group compared with the LAM-based (2.1% versus 12.6%; P<0.0001) and LdT groups (10.9%; P<0.0001; Supplementary Figure 1 and Supplementary Table 6 in Additional file 1). Similarly, the cumulative incidence of genotypic resistance was significantly lower in the ETV group compared with LAM-based (1.2% versus 10.1%; P<0.0001) and LdT groups (8.4%; P=0.0002; Supplementary Figure 2 and Supplementary Table 6 in Additional file 1).

Cumulative incidence (Kaplan–Meier) of liver-related events of HBV disease progression by treatment group
Clinical outcomes
The cumulative incidences and survival analysis for liver-related events of HBV disease progression are shown in Table 3 and Figure 2, respectively. Over the 240-week study period, HBV disease progression was reported in 10.7% and 14.0% of patients in the ETV and LAM-based groups, respectively.
The incidence of HBV disease progression was 7.0%, 12.1% and 4.0% in the LdT, ADV and other de novo combination groups, respectively. In the time-to-event analysis, the risk of HBV disease progression was significantly lower in the ETV group compared with the LAM-based (P=0.0113) and LdT (P=0.0054) groups (Figure 2).
The progression to compensated or decompensated cirrhosis was the most frequent disease progression event. Progression to compensated cirrhosis was reported in 4.1% of patients in the ETV group and 3.8% of those in the LAM-based group. Decompensated cirrhosis was reported in 6.4% and 9.6% of patients in these groups, respectively.
Hepatocellular carcinoma incidence was 0.8% in ETV group versus 1.9% in the LAM-based group; corresponding rates of liver-related death were 0.8% and 1.0%, respectively. The cumulative probability of hepatocellular carcinoma incidence was significantly lower in the ETV group compared with the LAM-based group (P=0.0308; Supplementary Figure 3 in Additional file 1).
Safety
A total of 793 patients (23.1%) experienced 1,559 treatment-emergent AEs (TEAEs); of these, TEAEs led to treatment discontinuation in 44 (1.3%) patients (Table 4). The most common TEAEs leading to discontinuation were hepatic cancer in eight (0.4%) and other hepatobiliary disorders (hepatic cirrhosis, hepatic failure) in six (0.3%) patients.
Summary of TEAEs and SAEs

Treatment-emergent adverse events (TEAEs) are defined as adverse events (AEs) that present prior to receiving the first dose of study drug and subsequently worsened or not present prior to receiving the first dose of study drug but subsequently appeared. ADV, adefovir; ETV, entecavir; LAM, lamivudine; LdT, telbivudine; SAE, serious AE.
A total of 287 patients (8.4%) experienced 430 SAEs; of these, 20 events were reported as related to the study drug. SAEs were reported in 143 (7.9%) and 67 (10.6%) patients in the ETV and LAM-based groups, respectively. The most common SAEs were neoplasms (benign, malignant and unspecified, 2.5%) and hepatobiliary disorders (2.1%). 34 patients (1.0%) died; among these 15 (0.8%) were in the ETV group and 13 (2.06%) in the LAM-based group.
Discussion
This prospective, longitudinal observational study in treatment-naive CHB patients with or without compensated cirrhosis demonstrated a sustained virological response at 5-year follow-up with both ETV and LAM-based therapies; however, ETV therapy was associated with a significantly lower incidence of viral breakthrough, genetic resistance and HBV disease progression. The longitudinal follow-up data from a large sample size provided several insights into the real-world treatment patterns and outcomes in this patient population.
The baseline demographic and clinical characteristics of the study population were comparable with those reported in previous real-world prospective and retrospective studies in China [9,15–18]. The mean age of patients was approximately 40 years, 74% were male and 60.4% were HBeAg-positive; these were comparable to the NA-naive cohort of the REALM study (Randomized, Observational Study of Entecavir to Assess Long-term Outcomes Associated with Nucleoside/ Nucleotide Monotherapy for Patients with Chronic HBV Infection), as well as patients’ demographics from the China Registry of Hepatitis B (CR-HepB) [9,15,17,19]. However, the baseline HBV DNA levels (7.4 log10 IU/ml) were higher than those in the REALM study (6.78 log10 IU/ml), as was the proportion of patients with compensated cirrhosis (23% versus 10% in the REALM study and 16.3% in CR-HepB) [9,15].
A major consideration in selecting NA therapy for patients with CHB is the high barrier to resistance [6,20]. However, the present study demonstrated that a substantial proportion of patients in tier 2/3 city hospitals received LAM-based therapies as first-line treatment during the study period. The longitudinal analysis of treatment patterns showed that a higher proportion of patients who initiated LAM-based therapies required treatment modification compared with those who initiated ETV monotherapy (25.9% versus 13.7%). Notably, most treatment modifications for those receiving LAM-based therapies were triggered by viral breakthrough in contrast to financial reasons in the ETV group. This is in line with the well-established non-response and resistance profile of LAM-based therapies. A previous study in Chinese patients with CHB demonstrated viral breakthrough in 34.8% of patients receiving LAM therapy at 3 years’ follow-up [21]. The long-term studies have demonstrated resistance rates of up to 71% with LAM and up to 29% with ADV therapy [22,23].
Of note, the observed cumulative resistance rates in the LAM-based and LdT therapy groups were lower than previously reported. This can be explained by the study design feature which retained patients who underwent treatment modifications in the initial treatment group for outcome analysis. Hence, resistance rates observed in this study with LAM-based and LdT groups are an underestimate. The emergence of viral resistance negates the initial viral response and is associated with high incidence of hepatic fares, hepatic decompensation and HCC [24,25].
Considering the clinical impact of viral resistance, ETV therapy is not only more efficacious, but also cost-effective than LAM and ADV. Indeed, a cost-effectiveness study in China showed that LAM monotherapy or in combination with ADV is not cost-effective due the high frequency of genetic resistance which leads to higher costs over the course of disease. Conversely, first-line treatment with ETV was found to be the most cost-effective therapy due to its higher efficacy and low risk of resistance [26]. In 2017, the reimbursement schemes in China were updated to include ETV and tenofovir in the national basic medical insurance reimbursement list, which may reduce the cost burden on patients and increase the utilization of these NAs as preferred first-line therapies [1]. However, the local reimbursement policies and executions vary in different provinces and cities, especially in the tier 2/3 cities, and LAM-based regimen had been used until several years ago as first-line therapy for treatment-naive patients due to its availability and affordability as well as clinical inertia based on clinicians’ previous experience. The results of this study refected the realm of the treatment patterns for patients with CHB in the tier 2/3 cities.
ETV monotherapy was associated with significantly higher rates of virological response compared with LAM-based therapies at weeks 48 and 96. After 5 years of follow-up, the virological response was sustained in most patients with no significant difference between treatment groups (73% in both groups). However, the incidences of viral breakthrough and genotypic resistance were significantly lower in the ETV group compared with the LAM-based group (P<0.0001 for both). The long-term virological response rate with ETV therapy in our study was lower than that reported previously. In the 10-year follow-up of the REALM study China cohort, 85%, 90% and 90% of NA-naive patients achieved virological response at 5-, 7- and 10-year follow-up, respectively [17]. Another prospective observational study in treatment-naive CHB patients reported higher rates of virological response with ETV therapy at 5 and 7 years (98.7% at both time points) [27]; however, in this study patients received continuous ETV therapy.
The lower rates of virological response with ETV therapy in our study could be an underestimate, as patients who underwent treatment modifications were retained in the original treatment group for outcome analyses as per the study design. Consequently, patients who switched therapy from the ETV group, primarily due to financial reasons, may have influenced the overall virological response. On the other hand, this also suggests that the efficacy of LAM-based group may be an overestimate, as a higher number of patients switched therapy or had an add-on treatment due to lack of efficacy. In addition, higher baseline HBV DNA levels (≥8 log10 IU/ml) have been associated with lower rates of virological response [16,17], and in the current study, about 42% of patients had baseline HBV DNA levels ≥8 log10 IU/ml, which may partly explain the lower rates of virological response in the present study. Furthermore, medication compliance could be a key contributing factor in a real-world setting. In a retrospective study of patient records between 2010-2016 showed that only 55.5% patients had ≥80% compliance to antiviral treatment in clinical practice [18]. In the present study, medication non-compliance was reported in 5.8% and 6.3% of patients in ETV and LAM-based groups, respectively.
Furthermore, a slightly higher total bilirubin (>1 and ≤3xULN), but not severely high total bilirubin (>3xULN), was positively associated with virological response at week 240. The possible explanation for this could be that the patients with bilirubin levels >1 and ≤3xULN may have a higher immune response than those with normal bilirubin levels, which may contribute to the viral suppression by immune system. However, patients with bilirubin levels >3xULN may have more severe disease status which may affect virological response. In addition, non-hepatic causes for slight increase in total bilirubin levels cannot be excluded.
Overall, the cumulative serological response rates were high during the study; however, the HBeAg clearance and seroconversion rates at 5 years (13.2% and 6.3% with ETV and 14.3% and 5.7% with LAM-based) was lower than previously reported with ETV and LAM-based therapies [15,19,28]. In the NA-naive China cohort of the REALM study, the HBeAg clearance and seroconversion rates were 17% and 15%, respectively, with ETV therapy at 1 year [15]. A retrospective analysis of treatment-naive patients in the CR-HepB revealed an HBeAg clearance rate of 28.2% and seroconversion of 12.6% at 5 years with ETV therapy [19]. The HBeAg clearance and seroconversion are generally temporary events and their durability varies regardless of virological response [29].
Analysis of clinical outcomes showed a significantly lower risk of HBV disease progression with ETV compared with LAM-based therapy (P=0.0113). Compared with ETV therapy, patients receiving LAM-based therapy were more likely to have a progression to decompensated cirrhosis (6.4% versus 9.6%, respectively) and hepatocellular carcinoma (0.8% versus 1.9%). These results are in line with previous studies which demonstrated reduced risk of HBV disease progression and hepatocellular carcinoma with ETV therapy [5,30]. In addition, a 5-year study in Japanese patients with CHB showed that ETV was superior to LAM in reducing the risk of hepatocellular cancer, especially in patients with cirrhosis [5]. In the 10-year follow-up of the REALM study, there was no significant difference between ETV and non-ETV groups for the risk of liver-related HBV disease progression, malignant neoplasms and death [17]. However, the China sub-study showed significantly higher rates of virological response with ETV versus non-ETV therapy and that the virological response was associated with a significantly lower risk of liver-related HBV disease progression and hepatocellular carcinoma [17].
Interestingly, the current study showed a lower rate of HBV disease progression in the LdT versus ETV group (7% versus 10.7%), despite a higher incidence of virological breakthrough, genetic resistance and treatment modifications in the LdT group. These results can be explained by multiple factors – firstly, patients who underwent treatment modifications were retained in the original treatment group for the outcome analysis as per the study protocol. In the LdT group, 25.4% of patients reported ≥1 treatment change, which was much higher than the ETV group (13.7%), and a large number of these modifications were due to viral breakthrough. However, due to the study design, these patients were retained in the LdT group for the outcome analysis. Secondly, this was an observational study and the initial treatment regimen was decided by the investigator; hence, the baseline clinical characteristics of patients in each group were not comparable. For example, the proportion of patients with cirrhosis was higher in the ETV group versus LdT group (24.8% versus 13%), as were those with alcohol consumption (16.2% versus 10.9%) and longer (>15 years) disease duration (24.4% versus 14.7%). This suggests that patients who received ETV as first-line therapy were at high risk of disease progression. Taken together, these reasons may explain the higher incidence of liver-related events of HBV disease progression in the ETV group versus LdT group.
In line with prior reports, ETV treatment was found to be well tolerated, with no new safety signals determined. The incidence of TEAEs and SAEs leading to study discontinuation was lower in the ETV group compared with the LAM-based groups.
The strengths of the study are that the enrolment criteria refect the spectrum of patients encountered in clinical practice across China, as well as the non-interventional and multicentre nature. The limitations of the study include potential variations in reporting across the 63 centres included in the study, as well as high treatment discontinuation rates, lack of histological assessment and intent-to-treat analysis. Patients that had received therapy with generic drugs or who changed to a generic drug within the first 52 weeks were excluded. This may have introduced a bias to patients that have access to health care at tier 2 city hospitals or that can benefit from co-payment. During the first 52 weeks of the study, data was not blinded; this may have infuenced treatment decisions with regards to treatment modification. Furthermore, patients who underwent treatment modifications were retained in the original treatment group, which may have resulted in under- or overestimation of the treatment effects.
In conclusion, in this long-term real-world study in treatment-naive patients with CHB in China, ETV monotherapy was associated with a significantly lower risk of HBV-related disease progression compared with LAM-based therapies. The study results add to the existing evidence on high risk of viral breakthrough and genotypic resistance with LAM-based therapies and further supports ETV monotherapy as an optimal first-line treatment in line with the guideline recommendations. With the inclusion of ETV and TDF in the national list of reimbursable medicines, the use of optimal NA therapies will certainly improve in clinical practice.
Footnotes
Acknowledgements
This study is funded by Bristol Myers Squibb, China. J Jia reports the consultation and speakers fee from BMS, Gilead and GSK. S Zhu is an employee of Bristol Myers Squibb. All other authors have no conflict of interest to declare.