
Abstract
Background
In patients treated for HCV infection, potential drug–drug interactions (DDIs) can occur among direct-acting antiviral drugs (DAAs) and comedications used. The real-life effectiveness and safety of elbasvir/grazoprevir (ELB/GZR) among co-medicated HCV patients was evaluated.
Methods
We prospectively evaluated consecutive patients from 15 clinical centres participating in PITER who were treated with ELB/GZR and had been followed for at least 12 weeks after treatment. Data were prospectively collected on the use of comedications (including discontinuation, dose modification and addition of drugs) and potential DDIs with DAAs.
Results
Of the 356 patients with at least 12-week post-treatment follow-up (median age 67, range 50–88 years), 338 (95%) achieved sustained virological response. Of these, 219 (60%) had at least one comorbidity (median 2, range 1–6); information on comedication was available for 212 of them. Of 190 comedications used, 15 (8%) drugs were modified during ELB/GZR therapy, specifically in 9 (4%) patients they were interrupted, in 2 (1%) of whom, the comedication was interrupted before the DAA therapy because of potential DDI (that is, patients treated with carbamazepine); in 12 (6%) patients the comedications were modified in terms of dosage. In 29 (14%) patients, the comedications required monitoring when used with ELB/GZR, as well as with all available DAAs. Of the 190 drugs, 27 (14%) used in 67% of patients were free of DDIs when used with ELB/GZR, whereas they required monitoring if used with other DAA regimens.
Conclusions
The results of this prospective study support findings that ELB/GZR is effective and safe in most treated patients.
Introduction
The development of second-generation direct-acting antivirals (DAA) represents a historical breakthrough, in that these drugs have been shown to eradicate HCV in more than 95% of patients, regardless of HCV genotype, baseline HCV RNA levels, race, HIV status or severity of hepatic fibrosis [1,2]. For adults chronically infected with HCV genotypes 1 and 4, elbasvir/ grazoprevir (ELB/GZR) represents an effective option, even for a number of difficult-to-treat populations. Furthermore, the dosage does not need to be adjusted in patients with any degree of renal impairment or in patients with mild hepatic impairment (Child–Pugh A cirrhosis) [3–7].
However, none of the DAAs is completely free of drug–drug interactions (DDI), which can significantly alter the drugs’ exposures and thus their efficacy and toxicity. Studies on interactions between DAAs and some key drugs have been performed in the development of all DAAs, yet mainly among healthy volunteers, whereas participants in clinical trials usually have shown few comorbidities and thus are prescribed limited concomitant medications [8]. There is limited data that prospectively address DDIs in patients with chronic HCV infection who are on DAA therapy. In a previous work we reported the real-life efficacy and the potential DDIs of DAAs (sofosbuvir-based therapies and ombitasvir, paritaprevir and dasabuvir regimens) with co-medications used in outpatients with mild and severe liver disease due to HCV chronic infection, as part of the PITER Cohort Study (Italian Platform for the Study of Therapies for Chronic Viral Hepatitis) [9,10]. In the present study, we prospectively evaluated the outcomes of treatment with the ELB/GZR combination, in terms of effectiveness and safety, which included a prospective evaluation of DDIs during this DAA therapy.
Methods
Patients
The study was prospective in design and was conducted among patients attending 15 clinical centres involved in PITER [9]. For the present study, we retrieved data from all consecutive patients treated with ELB/GZR since its first use in Italy (January 2017). Data during the follow-up after the 12-week post-treatment was evaluated until December 2018. Each patient's data included an evaluation of the efficacy of ELB/GZR and a prospective evaluation of the comedication profile from the onset of ELB/GZR treatment, during treatment and at 12 weeks from the end of treatment.
The fibrosis stage was defined based on liver transient elastometry data, which were considered validated if the patient had at least 10 valid stiffness measurements, with a success rate of at least 80%, an interquartile range of less than 30% of the median stiffness score and a body mass index (BMI) <30 kg/m2. Liver fibrosis staging with combination of APRI and FIB-4 scoring systems in chronic hepatitis C were used as an alternative to transient elastography in patients with BMI ≥30 kg/m2. The severity of liver disease was classified as ‘mild’ if the stiffness score was equal to or lower than 10 kPa and as ‘moderate-to-severe’ if it was higher or if there were signs of liver cirrhosis (signs of portal hypertension). The correlation of stiffness value with Metavir fibrosis stage was based on cutoff values for fibrosis stage assessment, previously reported [11]. Patients with severe liver disease (Child-Pugh B and C) were excluded, in that treatment with ELB/GZR is not indicated in these patients [12,13].
Outcomes
Virological response was defined as undetectable HCV RNA (limit of detection ≤15 IU/ml) and was determined at the end of treatment and at week 12 (SVR12) post-treatment. Virological failure was defined as detectable HCV RNA at any time during treatment or post-treatment follow-up. Aminotransferase and bilirubin, as well as stiffness values, were assessed at baseline at week 8 and at week 12 during treatment, and at week 12 after the end of treatment. Serious adverse advents were defined as any life-threatening event or an event that led to hospitalization, prolonged an existing hospital stay or resulted in death, or those that were considered serious based on a physician's professional opinion.
Assessment of Comedications and the Potential Drug-Drug Interactions
The potential DDIs of drugs that were recorded on the treated patients and drugs that were added to or removed from the comedication list during antiviral therapy were assessed and classified based on information available in the HEP Drug Interactions website. Specifically, the potential DDIs for the ELB/GZR regimen and of each drug used as comedication were assigned to four different risk categories: category 0 -classification not possible due to lack of information; category 1 - no clinical interaction possible; category 2 - may require dose adjustment/closer monitoring; category 3 - co-administration not recommended or contraindicated.
The profiles of the comedications that were added or removed were evaluated according to the risk categories, in order to define if the changes were required due to a specific risk category. If changes were due to a potential DDI, the information was also recorded on the electronic case report form (eCRF).
Statistical Analysis
Statistical analyses were performed using the SAS statistical package, version 9.4 (SAS Institute Inc., Cary, NC, USA). Differences among the proportions were evaluated by χ 2 or Fisher's test, as appropriate, whereas the Student's test was used for continuous variables. A P-value of less than 0.05 was considered as significant.
The crude odds ratios (OR) that links HCV treatment failure to potential risk factors (that is, age, gender, fibrosis stage, HCV RNA genotype, previous interferon [IFN]-based treatment, presence of cirrhosis versus other fibrosis stages, ribavirin use [yes/no] and comedication use [yes/no] during antiviral therapy) were calculated by univariate analysis. Adjusted ORs were calculated by multiple logistic regression analysis to identify variables that were independently associated with the failure. The reference category for OR estimates was that of the most favourable levels of exposure.
Ethics
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and the principles of good clinical practice. The study protocol was approved by the Ethics Committee of the Istituto Superiore di Sanità (Italian National Institute of Public Health) and by the local ethics committees of each clinical centre. The patients’ data were evaluated through an anonymous analysis, adopting codes generated by the eCRFs. Informed consent had been obtained from each patient upon enrolment in this study.
Results
Virological Response Evaluation
From January 2017 to December 2018, 365 patients with chronic HCV infection, consecutively enrolled in PITER, underwent treatment with ELB/GZR, with or without ribavirin. Of these patients, 298 (81.6%) had HCV RNA genotype lb, 39 (10.7%) genotype la and 28 (7.7%) genotype 4. Demographic characteristics, previous treatment experience, ribavirin use and the SVR12 according to the fibrosis stage are reported in Table 1. The liver fibrosis stage was distributed as follows; 193 (53%) patients had F0-F1 fibrosis stage, 75 (20%) F2 fibrosis stage, 43 (12%) F3 fibrosis stage and 54 (15%) F4/Child A cirrhosis. Data from 356 patients (median age: 67; range 50-88 years), who reached the 12-week evaluation after the end of treatment, were considered for the sustained virological outcome. Of these patients, 338 (95%) reached the SVR12 and 18 (5%) failed.
Baseline characteristics of patients treated with ELB/GZR in PITER cohort from January 2017 to December 2018

ELB, elbasvir; GZR, grazoprevir.
According to the logistic regression analysis, female gender and previous IFN-based treatment were independent factors of failure (Table 2). Of 18 patients who failed, 13 (72%) were female (median age 69; range 45–82 years).
Univariate and logistic analysis linking failure with independent variables
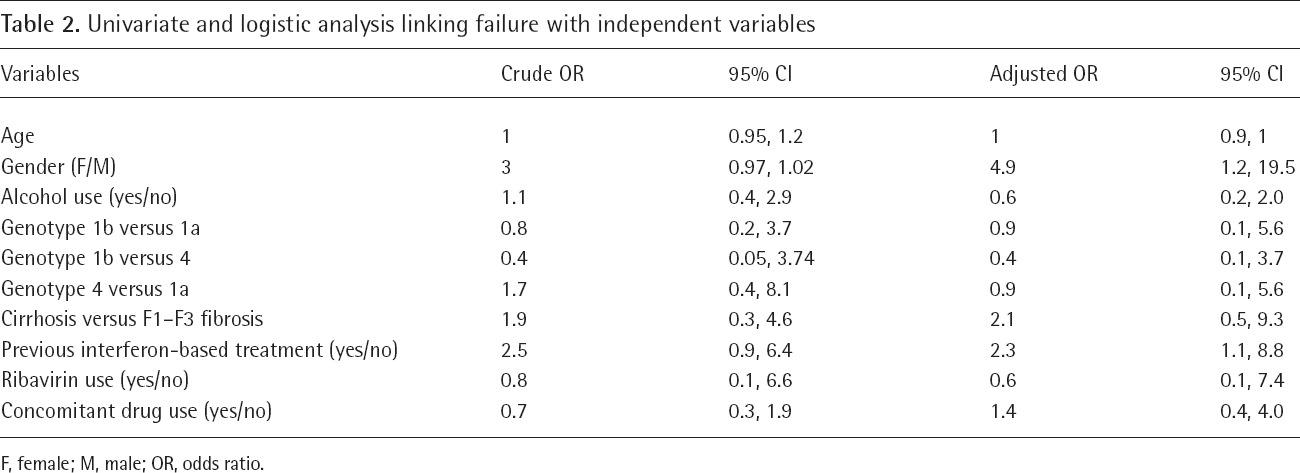
F, female; M, male; OR, odds ratio.
Clinical Evaluation
Two (4%) of these patients died after reaching SVR, due to causes not related to liver disease or antiviral treatment, one due to respiratory failure and the other due to acute myocardial infarction, both events reported to not be correlated to the DAA therapy. No hospitalization or other severe events were recorded during the use of DAA therapy. None of patients developed de novo hepatocellular carcinoma (HCC) during and after antiviral treatment independent of whether they achieved viral eradication or not.
Only one patient was non-adherent to treatment because she stopped treatment at the first month for anxiety. Of the treated patients, 8 (2%) patients were lost at follow-up (they started treatment and were all end-of-treatment responders, then were not presented at the same clinical centre for the SVR12 evaluation until the end of the study period). Overall, in 110 patients for whom the stiffness evaluation was available at baseline and at the end of follow-up (the median follow-up of 12.7 months from the end of treatment; range: 5–18 months), significant decreases in the stiffness values were observed in F2 to F4 fibrosis stage (Table 3). In the 18 patients who did not achieve SVR12, during a mean follow-up of 7.1 months (
Pre- and post-treatment stiffness values in patients a who achieved SVR12
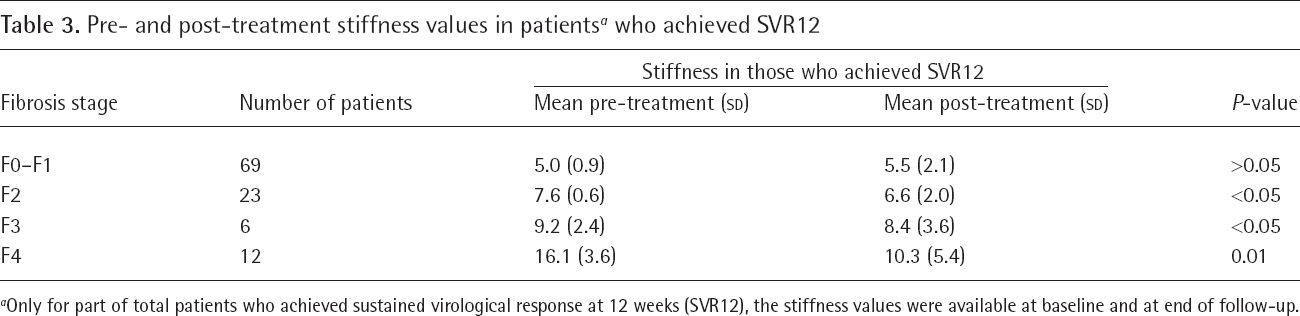
Only for part of total patients who achieved sustained virological response at 12 weeks (SVR12), the stiffness values were available at baseline and at end of follow-up.
Normal transaminase levels were observed in all but two patients who achieved SVR12. The mean alanine aminotransferase (ALT) values were 55 (
The mean bilirubin level was 0.8 (
Comorbidity and Comedication Profile
Of the 365 patients, 219 (60%) had at least one diagnosed comorbidity and of the 343 patients for whom comedications were recorded on the eCRF 212 (62%) reported having taken at least one drug during antiviral therapy. The number of comorbidities and comedications according to the fibrosis stage are reported in Table 4.
Number of comorbidities and comedications according to the fibrosis stage
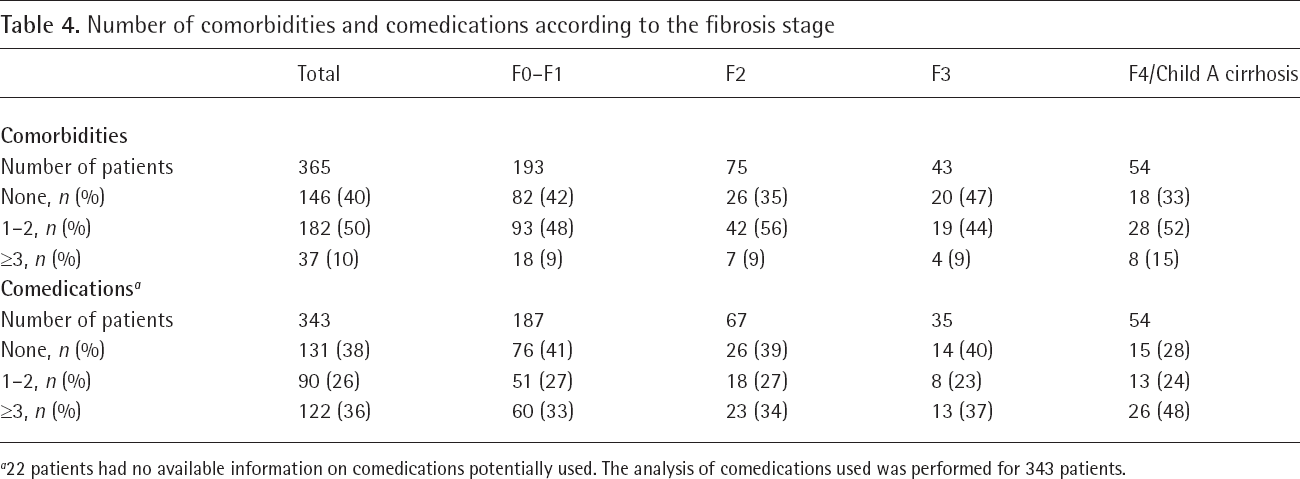
22 patients had no available information on comedications potentially used. The analysis of comedications used was performed for 343 patients.
The following comorbidities were present: cardiovascular disease in 145 (39.7%) patients, diabetes in 37 (10.1%) patients, neuropsychiatric disease in 35 (9.6%) patients, tumours in 23 (6.3%) patients, dyslipidaemic disorders in 20 (5.5%) patients, autoimmune disease in 18 (4.9%) patients, renal disease in 15 (4.1%) patients, osteoarticular disease in 12 (3.3%) patients, haematological disease in 9 (2.5%) patients and other comorbidities in 24 (6.6%) patients. The presence of comorbidities was similarly distributed in each fibrosis stage, whereas the presence of more than three comorbidities was more common among patients with fibrosis stage F4 (15%) compared with the other stages (9–10% for stages F0 to F3), though the difference was not significant (P=0.6). Regarding comedications, 754 comedications were reported to have been used by 212 patients (9 patients were relapsers and 203 were patients who achieved the SVR12); these comedications belonged to 190 single drugs. Of the 54 patients with fibrosis F4/cirrhosis, 39 (72%) received comedications, compared with 173 (60%) of the 289 patients with fibrosis stages F0–F3 (P=0.006). The use of 1–2 comedications was similarly (23–27%) distributed among patients with fibrosis stages F0–F3, whereas the use of more than 3 comedications (up to 15) was more frequently observed in patients with F4/cirrhosis (48%; P=0.03). Of the 190 drugs used, 20 (10%) were added as new drugs during antiviral therapy (Table 5). Of these drugs, all were classified as category 1 (no interaction), with the exception of atorvastatin and simvastatin, which were added during therapy in 4 (1%) patients and defined as category 2 (requiring monitoring by HEP Drug Interactions due to potential interactions with hepatitis C drugs). The daily dose of atorvastatin and simvastatin was 20 mg/day, co-administered with ELB/GZR. No changes were recorded for statins, which were used at the lowest dosage recommended during DAA therapy. Overall, 15 drugs were modified or interrupted during ELB/GZR therapy, specifically 9 (4%) patients were interrupted, 2 (1%) of whom had comedication interrupted before DAA therapy because of a DDI (that is, patients treated with carbamazepine). In 12 (6%) patients, the comedications used were only modified in terms of dosage or pharmaceutical form. Overall, 29 (14%) patients, all of whom achieved the SVR12, used drugs that required monitoring in concomitant use with ELB/GZR, and required monitoring or were contraindicated also if used with other DAA regimens. Specifically, 10 (5%) patients used statins: atorvastatin, simvastatin and rosuvastatin; 14 (7%) used antiplatelets and anticoagulants: rivaroxaban, dabigatran and warfarin; 3 (1%) used drugs for symptoms of an enlarged prostate: silodosin, 1 (0.5%) used drug to prevent gout attack: colchicine and 1 (0.5%) used a central nervous system drug (quetiapine). In none of patients who relapsed, potential DDIs were reported by HEP Drug Interactions website and none of the comedications were changed during the antiviral therapy.
Comedications changed (added or removed) during the ELB/GZR therapy

Atorvastatin and simvastatin were the only drugs that required monitoring during elbasvir (ELB)/grazoprevir (GZR) therapy. Carbamazepine was interrupted before starting the ELB/GZR therapy because contraindicated as concomitant use with all direct-acting antiviral regimens.
Of the 212 patients that used comedications, 141 (67%) used drugs (27 single drugs; 14%) that are considered as category 1 (no interaction) when concomitantly used with ELB/GZR but that are considered as category 2 (monitoring/reduce dosage) or category 3 (contraindicated) when used with other DAA regimens (data not shown).
Discussion
The results of this study confirm the efficacy and safety of ELB/GZR in a heterogeneous adult and elderly population with chronic HCV infection, mainly with HCV genotype 1b, which is the prevalent genotype in Italian patients. The overall failure rate of ELB/GZR in our study patients, who were not of a young age and had a significant number of comorbidities [9], was 5%, which is similar to the rates reported by clinical trials and real-life studies in other geographical areas. These data confirm that the efficacy of ELB/GZR (as measured by SVR12 rates) is generally not affected to any meaningful degree by factors such as age, gender, HIV status or cirrhosis status [5,14–19]. In this study, ELB/GZR showed the same levels of efficacy and safety when comparing patients with Child A cirrhosis to those with mild liver fibrosis. These findings confirm data from clinical trials and differently from previous reports, do not show a negative impact of severe liver fibrosis and cirrhosis on the DAA response rate [4,5,20,21]. Patients that were lost to follow-up or were not adherent to treatment were not counted as non-responders in that this is not an intention-to-treat study. This is a real-life cohort study and it could be expected that a few patients could be lost to follow-up and this could have some impact in the results of the study. Female gender and previous IFN-based therapy were independent factors related to failure. Regarding female gender, previous studies have reported a lower efficacy of IFN-based therapy in women compared with men, yet, to date, there have been no reports of lower efficacy among women using the DAA-based regimens. The mechanisms underlying the more frequent failure of efficacy among women are not clear. However, in the PITER cohort, the prevalence of cirrhosis was found to have been higher among women of menopausal age, compared with same-age men [22–25]. Of note is the fact that the mean age of treated women in this study was 64 ±18 years, suggesting that menopausal age should be taken into consideration in interpreting our results, though other studies that evaluated the same or other DAA regimens would need to be performed to confirm this data. Previous treatment with IFN-based therapy is one of the known predictors of potential DAA failure and the HCV treatment guidelines include specific recommendations for this group of patients [12,13]. In our study, the rate of failure was very similar to that reported in clinical trials on ELB/GZR in patients who had shown null response following treatment with pegylated IFN and ribavirin (7.7% versus 7.5%) [3]. Data on the presence of baseline NS5A resistance-associated substitutions (RAS) were not available in this study because, in accordance with the most recent EASL guidelines, routine testing for RAS is not required in Italy [12]. However, HCV RNA genotype 1a was not an independent factor of failure in this cohort.
Regarding the effectiveness following the SVR, very good results were observed in terms of improvement of liver inflammation markers. Significant decreases in transaminase levels and liver stiffness levels were observed in all patients, independent of age, gender and pre-treatment fibrosis stage. This indicates that if viral eradication has been achieved prior to a severe cirrhosis stage, liver inflammation and fibrosis improve significantly, in accordance with previous reports [26]. On the contrary, and as previously reported by PITER data, the effectiveness of DAAs was not as high in patients with very severe stages of liver disease, independently of the DAA regimen used [27].
In only two patients, transaminase levels were slightly higher than normal at the end of treatment. In clinical trials on ELB/GZR, regardless of treatment duration, 1% of patients experienced elevated ALT levels, reaching levels that were 5x higher than the upper normal levels. These increases were typically asymptomatic, and they resolved with ongoing therapy or after its completion [16]. The frequency of late ALT increases has been reported to be higher in patients with higher GZR plasma concentrations, which could in part be due to the DDIs with one or more concomitant drugs [28,29]. In our study, no DDIs with ELB/GZR were reported in patients with increased ALT levels during antiviral treatment.
As mentioned, Italian patients with chronic HCV infection are not young, due to a known cohort effect of HCV chronic infection in Italy [30,31]. In light of this cohort effect, it is not surprising that patients with chronic HCV infection are of adult or elderly age and often have comorbidities and take several drugs as comedications during DAA treatment, conditions not present in patients included in clinical trials [32]. The current guidelines on HCV treatment included recommendations on potential DDIs, particularly for NS3/4A protease inhibitors and NS5A-NS5B polymerase inhibitors, with particular regard to patients with severe liver damage or chronic kidney damage [12,33–35]. However, the severity of liver disease is only one of the factors related to potential DDIs. The pharmacokinetic profiles and how they impact DDIs need to be carefully addressed before and following DAA treatment in clinical practice in patients with mild liver disease [34,36–40].
We previously evaluated the potential DDIs of sofosbuvir-based regimens (sofosbuvir and ledipasvir, sofosbuvir and daclatasvir) and ombitasvir + paritaprevir + dasabuvir. In the real-life use of these DAA regimens, category 2 DDIs were less frequent in patients with chronic hepatitis infection (31%), compared with those with moderate-to-severe liver damage (56%) [10]. In the present study, the analysis was based on the prospective profile of comedications used, in terms of their interruption, change or dosage modification and their potential impact on the efficacy of ELB/GZR. The comedication profile, evaluated for 190 drugs taken by 212 patients (overall, 754 comedications), did not show any significant DDI concerns, and only 14% of patients who achieved SVR12 used drugs that required monitoring (category 2), specifically, antiplatelets, anticoagulants and statins. These drugs are assigned to category 2 when used with any of the available DAA regimens [12]. Regarding parvastatin, which was used in this study, there were no potential DDIs in its use with ELB/GZR, though this drug is considered as category 2 when used with other DAA regimens [12]. The dosages of the statins used were the lowest ones, and no interruption or safety issues were raised for these patients throughout treatment. None of the drugs added or interrupted during antiviral therapy had a potential DDI. We prospectively collected data of the changes of the drugs used prior to the antiviral therapy at the time and during the ELB/GZR treatment with the aim to evaluate what happened to these patients during a careful evaluation of potential DDI before antiviral therapy. The very good DDI profile of ELB/GZR could be possible also because patients were specifically assigned to ELB/ GZR if no anticipated DDI was present. However, the drugs used before the ELB/GZR treatment were almost the same as those reported in our previous paper that evaluate the DDI profile used with other DAA regimens [10]. Proton pump inhibitors (PPI; omeprazole, pantoprazole, esomeprazole, rabeprazole) were the most frequently reported comedications in our study. They were used in 25% of patients, which is in accordance with our previous data in patients treated with other DAA regimens [10]. Although ELB/GZR therapy is not influenced by the use of PPIs [41], it is important to be aware of the recommendations concerning the co-administration of antacids, H2-receptor antagonists and PPIs. The potential DDIs between PPIs and DAAs has recently been emphasized, given that gastric pH could affect DAA bioavailability due to increased or decreased pharmacokinetics. However, this has not been confirmed by real-life studies as a predictor of lower DAA efficacy [42,43]. The solubility of velpatasvir decreases as pH increases and for most patients PPIs should be avoided or administered at a dose that does not exceed that of omeprazole 20 mg during sofosbuvir/velpatasvir and sofosbuvir/ velpatasvir/voxilaprevir treatment. Sofosbuvir/velpatasvir/voxilaprevir should be given with food and taken 4 h before the PPIs; for ELB/GZR, as for other DAA regimens, no indications on food taken are necessary [12].
Of the 190 drugs used in this study, 27 (14%) used in 67% of our patients, are free of potential DDIs with ELB/GZR, whereas they are considered as category 2 when used with other sofosbuvir based regimens and/or glecaprevir/pibrentasvir [12]. The key message of this finding is that careful evaluation of each comedication profile is necessary prior to selecting the specific DAA regimen.
In conclusion, the results of this study indicate that ELB/GZR has a high efficacy and very good effectiveness observed beyond the SVR, regardless of comorbidity status, comedications used and liver disease fibrosis stage. The potential DDIs between ELB/GZR and other medications are relatively low; thus, this regimen could be safely used in the majority of patients with chronic HCV infection, independent of age, comorbidity and comedications used.
Footnotes
Acknowledgements
Authors would like to thank PITER collaborating group and all clinical centres (Additional file 1) which are involved in the study on a voluntary basis. Authors would also like to thank Giampaolo La Terza (Medisoft Informatic Services, Rome, Italy) for database maintenance and implementation.
The potential DDIs were assessed and classified based on information available in the HEP Drug Interactions website.
This study was funded by Italian Ministry of Health, Grant number RF-2016-02364053.
The authors declare no competing interests.