
Abstract
Background
Methods
Results
Conclusions
Introduction
With recent advances in antiretroviral therapy (ART), HIV-1 infection can be considered a treatable chronic illness [1], and individuals with HIV-1 with high levels of adherence to highly effective ART have a life expectancy approaching that of HIV-negative individuals [2]. However, there remain several challenges to ensuring that individuals with HIV are able to achieve and maintain viral suppression, including treatment adherence and ART resistance, as well as factors that limit treatment such as stigma, delayed diagnosis, discrimination and lack of access to health care [3]. Socioeconomic disadvantages include unemployment, attempting to immigrate to another country, language barriers and mental health challenges such as depression [4]. These factors are interrelated, as a lack of resources can negatively affect adherence [5], and poor adherence can lead to development of HIV drug resistance mutations (DRMs), which may also lead to the transmission of drug resistance to a newly infected individual [6].
Current treatment guidelines recommend 2 nucleoside reverse transcriptase inhibitors (NRTIs) in combination with a third drug from the non-nucleoside reverse transcriptase inhibitor (NNRTI), integrase strand transfer inhibitor (INSTI) or protease inhibitor (PI) drug classes [7–9]. In the US Department of Health and Human Services and European AIDS Clinical Society guidelines, the 2-drug regimen (2DR) of the INSTI dolutegravir (DTG) plus the NRTI lamivudine (3TC) is an alternative option as initial ART for individuals when a preferred option is not available [7,8]. Individuals with HIV-1 infection with viral suppression may wish to switch therapy to a more simplified regimen or to manage comorbidities or drug–drug interactions [7–9]. For these individuals, 2DRs, such as DTG plus the NNRTI rilpivirine (RPV), DTG plus 3TC, or a boosted PI with 3TC, are recommended options [7–9]. In treatment-experienced adults with HIV-1 infection and drug resistance, guidelines recommend a new regimen of two or three fully active agents [7–9]. As a result of a high barrier to resistance with second-generation INSTIs and boosted PIs [10,11], DRMs are more likely to limit the effectiveness of the treatment regimen through decreased sensitivity to the NRTI or NNRTI component, particularly in 2DRs consisting of DTG in combination with either 3TC or RPV. To assess the risk of NRTI and NNRTI resistance in treatment-naive individuals in the general population who may be treated with a 2DR, it is important to determine the prevalence of pretreatment DRMs in individuals infected with HIV-1 who have had no ART exposure.
There have been many reports that have included data on pretreatment and acquired DRM rates from different geographic locations and varied populations. Thus, there are a large number of reports that can be analysed to provide a comprehensive review of global and regional prevalence rates for DRMs. The objective of this review was to use a systematic search of published literature reporting data on DRM prevalence to determine the prevalence of important pretreatment and acquired mutations conferring resistance to NRTIs and NNRTIs, specifically 3TC and RPV, as these are components of DTG-based 2DRs.
Methods
Search strategy and selection criteria
We conducted a systematic literature search in PubMed through 6 July 2018, using keywords related to geographic regions, specific DRMs and HIV. The geographic regions included in the analysis were Africa, Latin America, Middle East and North Africa, Europe, North America, Southeast Asia and Asia Pacific. Keywords for specific DRMs were selected to identify mutations associated with resistance to 3TC or RPV at the following codons: K65, K70, Q151 and M184 for 3TC resistance and L100, K101, E138, V179, Y181, Y188, G190 and M230 for RPV resistance. The DRMs with resistance to 3TC also have resistance to emtricitabine (FTC) and are referred to as 3TC/FTC-resistant DRMs in this manuscript. The specific DRMs included in the search were M184I, M184V, K65R, K65E, K65N, Q151M, K70E, L100I, K101E, K101P, E138A, E138G, E138K, E138Q, E138R, V179L, Y181C, Y181I, Y181V, Y188L, G190E and M230L [12]. A full list of keywords included in the search are included in Supplemental Table 1 in Additional file 1. Identified articles were manually searched for relevance and the prevalence rates within specific countries, which excluded most clinical trials and multinational cohorts.
Prevalence estimates were manually determined from the references. When possible, prevalence was included as reported by authors. If only absolute numbers or percentages were reported, the unreported values were calculated. If data were only presented in a graphical format, visual estimates were used to determine missing values. Estimates were recorded as not applicable (NA) when it could not be ascertained from the Methods section that the screening method included the particular DRM or when it could not be ascertained that all DRMs screened were reported in the Results section (for example, studies reporting most frequently observed DRMs). In cases in which multiple individual mutations with resistance to either 3TC/FTC or RPV were reported, but resistance to NRTIs or NNRTIs as a class were not reported, the class estimates were recorded as NA. Regional prevalence estimates were calculated as percentages using n values corresponding to all studies that assessed the mutation in question (that is, excluding n values from studies with NA values for that mutation). Results were reported as global and regional prevalence of substitutions identified at the codons associated with DRMs resistant to 3TC/FTC or RPV by codon, as well as codons where DRMs associated with resistance to NRTIs or NNRTIs as a class occur. Mutations resistant to the NRTI or NNRTI classes were reported in this review as described in the source publications and may have included mutations with resistance to NRTIs/ NNRTIs other than 3TC/FTC and RPV. Prevalence of pretreatment or acquired mutations were reported separately. Pretreatment mutations referred to mutations that occurred in articles that described the individuals as ART-naive. Acquired mutations referred to those that occurred after virological failure.
Results
Search results
The literature search retrieved 529 articles, 402 of which were removed. Reasons for removal included full text not available, data not relevant or not reported numerically and small n values. This left 127 articles to be included in the global and regional analyses. The identified articles included study periods from 1995 to 2017 and included >60,000 participants worldwide for analysis of pretreatment resistance mutations and >30,000 participants worldwide for analysis of acquired resistance mutations. Africa had the highest number of articles identified in the search of any region (n=30) [13–42]. However, the European region had the highest number of participants for analysis of pretreatment resistance mutations (n=33,957 for NRTI-associated mutations; n=34,201 for NNRTI-associated mutations) [43–60], and Southeast Asia had the highest number of participants for analysis of acquired resistance mutations (n=26,772 for NRTI-associated mutations; 26,568 for NNRTI-associated mutations) [61–69].
Global prevalence estimates
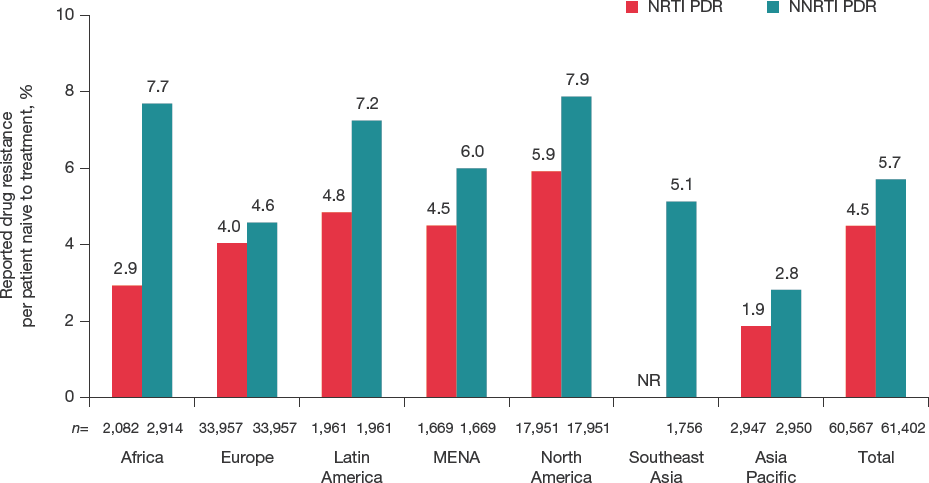
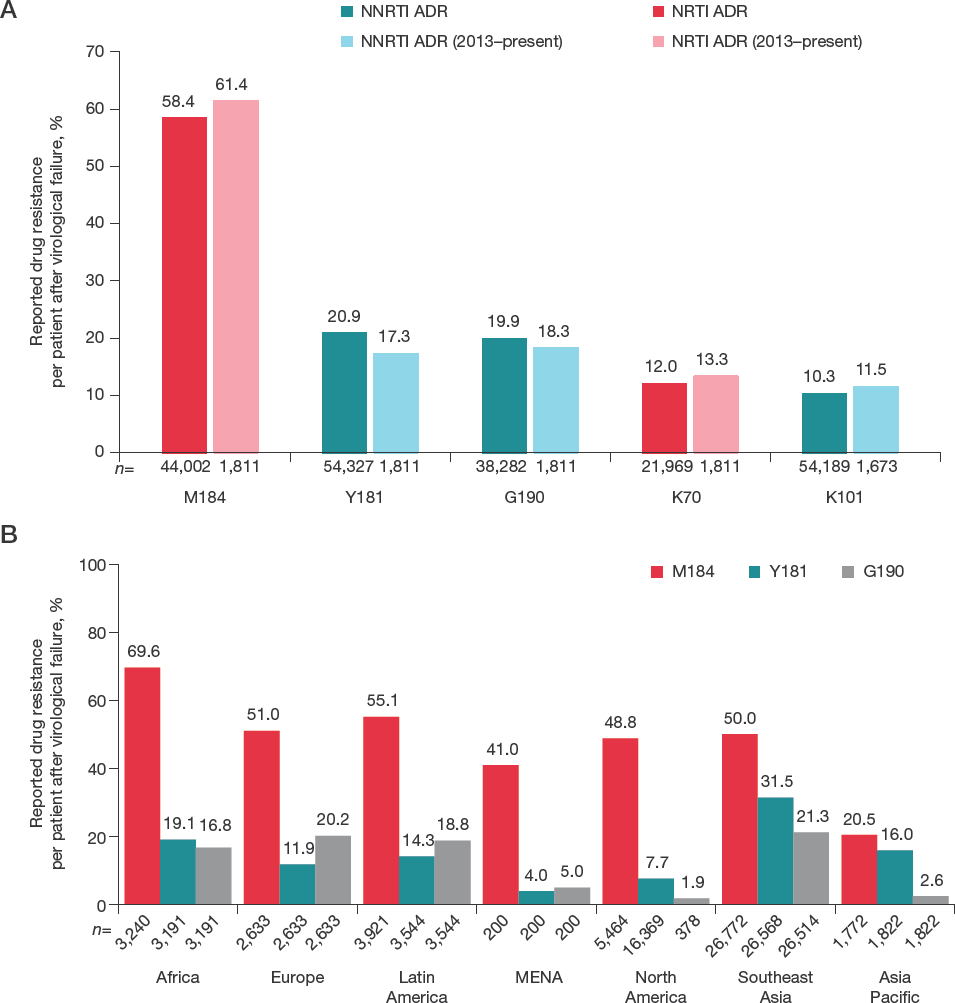
The estimated global prevalence of pretreatment DRMs was 4% (n=2,719/60,567; range, 2% [Asia Pacific] to 6% [North America]) for those associated with NRTI resistance [16,18,25,28,30–32,35–38,40,43,44,46,48,49,51–60,70–111] and 6% (n=3,605/61,402; range, 3% [Asia Pacific] to 8% [Africa and North America]) for those associated with resistance to any NNRTI (Figure 1) [16,18,25,28,30–39,41,70–85,99,100,102,104,106–120]. The only pretreatment DRMs estimated to occur in >1% of the global population were 3TC/FTC-associated DRMs at position M184 (1%), and RPV-associated DRMs at positions E138 (4%) and V179 (1%; Figure 2A).
Frequency of TDRs to any NRTI or NNRTI by region

Frequency of TDRs at codons associated with RPV and 3TC/FTC resistance
In a subset of studies that exclusively enrolled participants in the past 5 years (2013–present), the rates of the most frequent pretreatment DRMs were mostly consistent with the full data set (Figure 2A). One exception was V179, which had a prevalence rate of 4.2% (n=21/500) in studies enrolling participants from 2013 to present compared with 1.3% (n=283/21,969) in all studies. In this subset of studies, pretreatment NRTI DRMs were observed in 2.5% (n=17/672) and pretreatment NNRTI resistance DRMs were observed in 10.3% (n=144/1,391) of study participants, compared with 4.5% (n=2,719/60,567) and 5.7% (n=3,605/63,158), respectively, in all studies.
The most frequent pretreatment DRMs by region are shown in Figure 2B; mutations at position V179 were the most frequent DRMs in Southeast Asia (5.6%), Latin America (5.2%) and Africa (1.9%); mutations at position E138 were the most frequent DRMs in Europe (6.8%) and North America (1.6%); and mutations at position M184 were the most frequent DRMs in Asia Pacific (1.6%) and the Middle East and North Africa (1.1%). Drug resistance mutations at position M184 are associated with resistance to 3TC/FTC, while those at positions E138 and V179 are often associated with resistance to RPV [121].
Global estimated prevalence of acquired DRMs was 58% (n=17,073/29,218) for resistance to any NRTI and 67% (n=20,834/31,016) for resistance to any NNRTI in patients following virological failure (Figure 3) [13–29,44,45,47,50,60–69,77,80,81,85,91,101,103,104,109,122–134]. The highest rates of acquired DRMs for both NRTIs and NNRTIs were reported in Africa (NRTIs, 77% [n=702/917]; NNRTIs, 80% [n=730/908]), and the lowest were reported in North America (NRTIs, 23% [n=86/378]; NNRTIs, 19% [n=70/378]). In the subset of studies that enrolled patients only in the past 5 years (2013–present), global estimates of acquired DRMs were consistent with the full data set (Figure 4A). Acquired NRTI DRMs were observed in 59% (n=281/475) of participants and acquired NNRTI DRMs were observed in 60% (n=284/475) of participants. Across all regions, the most frequently acquired DRMs were the 3TC/FTC-associated mutations at position M184 (range, 20% [Asia Pacific] to 70% [Africa]; Figure 4B).

Frequency of ADRs to any NRTI or NNRTI by region
Frequency of ADRs at codons associated with RPV and 3TC/FTC resistance
Regional Prevalence Estimates: Africa
In the African region, DRM data were available from 3,995 individuals for pretreatment NRTI-associated DRMs and 4,013 individuals for pretreatment NNRTI-associated DRMs (Supplemental Tables 2 and 3 in Additional file 1) [16,18,25,28,30–41]. Among studies that reported DRMs by drug class, 3% (n=61/2,082) had NRTI-associated DRMs and 8% (n=224/2,914) had NNRTI-associated DRMs. The most frequently observed pretreatment 3TC/FTC DRMs in Africa were at position M184 (1%; n=54/3,968); the most frequent pretreatment RPV DRMs were at positions V179 (2%; n=16/851) and E138 (2%; n=11/731). Data on acquired DRMs were reported for 3,240 individuals for NRTI-associated DRMs and 3,191 individuals for NNRTI-associated DRMs (Supplemental Tables 4 and 5 in Additional file 1) [13–29,42]. Among reports with available data, 77% (n=702/917) and 80% (n=730/908) had acquired DRMs conferring resistance to the NRTI and NNRTI classes, respectively. The most frequent acquired 3TC/FTC DRMs were at position M184 (70%; n=2,255/3,240); the most frequent acquired RPV DRMs were at position Y181 (19%; n=611/3,191).
Regional Prevalence Estimates: Europe
In European studies, there were 33,957 people with data related to pretreatment NRTI-associated DRMs and 34,201 people with data on NNRTI-associated DRMs (Supplemental Tables 6 and 7 in Additional file 1) [43–60]. Pretreatment DRMs with NRTI resistance were observed in 4% (n=1,371/33,957) of individuals with HIV in the tested population, and pretreatment DRMs with NNRTI resistance were observed in 5% (n=1,553/33,957). The most frequently observed pretreatment 3TC/FTC DRMs were at position M184 (1%; n=67/11,700); the most frequent RPV DRMs were at positions E138 (7%; n=624/9,112) and V179 (1%; n=53/8,579). Data related to acquired DRMs with resistance to NRTIs and NNRTIs were available for 2,633 individuals (Supplemental Tables 8 and 9 in Additional file 1) [44,45,47,50,60]. Resistance to NRTIs was observed in 70% (n=1,846/2,633), whereas resistance to NNRTIs was observed in 52% (n=1,382/2,633). The most common acquired 3TC/ FTC DRMs in Europe were at position M184 (51%; n=1,344/2,633); the most common acquired RPV DRMs were at position G190 (20%; n=532/2,633).
Regional Prevalence Estimates: Latin America
In reports from Latin America, 3,295 individuals with HIV had data available for analysis of pretreatment DRMs (Supplemental Tables 10 and 11 in Additional file 1) [70–80]. Out of individuals with available data, pretreatment NRTI-associated DRMs were reported in 5% (n=95/1,961), and pretreatment NNRTI-associated DRMs were reported in 7% (n=142/1,961). The most common pretreatment 3TC/FTC DRMs were at position M184 (1%; n=18/3,295); the most common pretreatment RPV DRMs were at positions V179 (5%; n=122/2,338) and E138 (3%; n=65/2,338). Acquired DRM data were available for 3,921 individuals in Latin America (Supplemental Tables 12 and 13 in Additional file 1) [77,80,122–124]. Mutations resistant to the NRTI class were seen in 76% (n=344/450) of individuals, whereas DRMs resistant to the NNRTI class were observed in 58% (n=261/450). The most frequently observed acquired 3TC/FTC DRMs were at position M184 (55%; n=2,162/3,921); the most frequent acquired RPV DRMs were at position G190 (19%; n=668/3,544).
Regional Prevalence Estimates: Middle East and North Africa
Although there were relatively few studies (n=5) reporting on pretreatment DRMs from the Middle East and North Africa, 1,669 individuals with HIV had DRM data available from the identified reports (Supplemental Tables 14 and 15 in Additional file 1) [81–85]. Pretreatment DRMs with resistance to the NRTI and NNRTI classes were reported in 4% (n=75/1,669) and 6% (n=100/1,669) of the population, respectively. The most common 3TC/ FTC DRMs were at position M184 (1%; n=18/1,669); no DRMs associated with RPV resistance were reported in ≥1% of individuals. Data on acquired DRMs were available from 200 individuals, with 47% (n=70/149) and 30% (n=45/149) reported to have DRMs with resistance to the NRTI and NNRTI classes, respectively (Supplemental Tables 16 and 17 in Additional file 1) [81,85,125–127]. The most common acquired 3TC/FTC DRMs were at position M184 (41%; n=82/200) and the most common acquired RPV DRMs were at position E138 (6%; n=11/200).
Regional Prevalence Estimates: North America
In North America, data were available for pretreatment DRMs from 19,563 individuals with HIV (Supplemental Tables 18 and 19 in Additional file 1) [52,86–99]; 6% (n=1,062/17,951) and 8% (n=1,413/17,951) had mutations resistant to the NRTI and NNRTI classes, respectively. The most frequent pretreatment 3TC/FTC DRMs were at position M184 (1%; n=216/15,401); the most frequent pretreatment RPV DRMs were at positions E138 (2%; n=5/317) and V179 (1%; n=43/6,380). Data on acquired DRMs were available for 5,464 and 21,455 individuals to determine DRMs associated with 3TC/FTC and RPV, respectively; only 378 individuals had available data to assess resistance to the NRTI and NNRTI classes as a whole (Supplemental Tables 20 and 21 in Additional file 1) [91,128–130]. Acquired DRMs associated with resistance to the NRTI and NNRTI classes occurred in 23% (n=86/378) and 19% (n=70/378), respectively, of individuals with available data. The most common acquired 3TC/FTC DRMs were at position M184 (49%; n=2,668/5,464); the most common acquired RPV DRMs were at position Y181 (8%; n=1,259/16,369).
Regional Prevalence Estimates: Southeast Asia
In the subset of countries in Southeast Asia, 2,021 individuals had data on pretreatment DRMs (Supplemental Table 22 in Additional file 1) [112–118]. None of the reports included data on NRTI-associated DRMs; 5% of individuals had pretreatment NNRTI-associated DRMs (n=90/1,756). These DRMs included those at positions V179 (6%; n=21/377), E138 (2%; n=9/377) and Y181 (1%; n=22/1,974); the rest were <1%. Data were available for 26,772 and 26,568 individuals in Southeast Asia for 3TC/FTC- and RPV-associated acquired DRMs, respectively (Supplemental Tables 23 and 24 in Additional file 1) [61–69]. There were NRTI-resistant DRMs in 57% (n=13,976/24,602) of individuals and NNRTI-resistant DRMs in 69% (n=18,287/26,409). The most common acquired 3TC/FTC DRMs were at position M184 (50%; n=13,397/26,772); the most common acquired RPV DRMs were at positions Y181 (32%; n=8,369/26,568) and G190 (21%; n=5,650/26,514).
Regional Prevalence Estimates: Asia Pacific
In studies from countries in the Asia Pacific region, 4,179 and 4,088 individuals had data for DRMs associated with NRTIs and NNRTIs, respectively (Supplemental Tables 25 and 26 in Additional file 1) [100–111,119,120]. Pre-treatment DRMs with resistance to NRTIs and NNRTIs as a class were observed in 2% (n=55/2,947) and 3% (n=83/2,950) of individuals, respectively. The most frequently observed pretreatment 3TC/FTC DRMs were at position M184 (2%; n=65/4,179); the most frequent pretreatment RPV DRMs were at position V179 (2%; n=27/1,775). Acquired DRM data were reported for 1,772 and 1,822 individuals for NRTI- and NNRTI-associated DRMs, respectively (Supplemental Tables 27 and 28 in Additional file 1). Resistance to the NRTI and NNRTI classes were reported for 55% (n=49/89) and 66% (n=59/89), respectively, among individuals with available data [101,103,104,109,131–134]. The most common acquired 3TC/FTC DRMs were at position M184 (20%; n=363/1,772); the most common acquired RPV DRMs were at positions Y181 (16%; n=292/1,822), K101 (12%; n=220/1,822) and G190 (12%; n=217/1,822).
Discussion
In this review of 127 publications that reported data on the prevalence of pretreatment and acquired DRMs, a low estimated prevalence of pretreatment DRMs was observed. Acquired DRMs were observed in the majority of individuals following virological failure. In the subset of studies that did not enrol any participants prior to 2013 (5 years prior to the search date), a higher rate of mutations with resistance to any NNRTI and mutations at position V179 were observed compared with the full data set. Across regions, DRM rates were broadly similar, with the highest rates of pretreatment NRTI resistance in North America (6%) and pretreatment NNRTI resistance in Africa and North America (8%). Africa had the highest observed rates of acquired DRMs to any NRTI (77%) or NNRTI (80%). Of note, a relatively low rate of acquired NRTI and NNRTI DRMs were observed in North America (23% and 19%, respectively) compared with the global findings (58% and 67%, respectively). However, this difference should be interpreted with caution because class-level data on NRTI and NNRTI DRMs were only available from 378 individuals, 329 of whom were from a single report of incarcerated individuals in North Carolina [91]. Resource and monitoring limitations across regions may affect levels of pretreatment drug resistance. Recommendations from the World Health Organization (WHO) and the International Antiviral Society-USA call for routine surveillance of pretreatment drug resistance in people initiating ART and for closing gaps in services in resource-limited regions as means of reducing drug resistance [135,136].
For both pretreatment and acquired DRMs, resistance rates were higher for NNRTIs than for NRTIs overall. Pretreatment resistance to NNRTIs was substantially higher compared with NRTI resistance in both Africa (7.7% versus 2.9%) and Latin America (7.2% versus 4.8%). While the global and regional rates of pretreatment NRTI and NNRTI resistance were generally low (<10%), there are data to suggest that pretreatment resistance may be greater at the local level in some countries or communities. For example, while the overall rate of NNRTI DRMs in studies identified from Africa was 7.7%, there were individual reports showing rates >10%. These included a report in adult female sex workers in South Africa (27%) and one in immunocompetent children in Cameroon (41%) [16,32]. In addition, survey data from the WHO have shown pretreatment NNRTI resistance >10% in six countries: Argentina, Guatemala, Namibia, Nicaragua, Uganda and Zimbabwe [137]. The higher rates of NNRTI resistance observed in these reports support the WHO recommendation for non-NNRTI regimens in countries with high levels of pretreatment NNRTI resistance [135] and the inclusion of an antiretroviral with a high barrier to resistance (that is, INSTI or boosted PI) [10,138] in initial treatment regimens [7–9].
In this review, pretreatment DRMs in ≥1% of the population in the identified reports were at positions E138 (4%), V179 (1%) and M184 (1%); of these, M184 (51%) was among the most common positions for acquired DRMs as well. Mutations at M184 confer resistance to 3TC or FTC but reduce the fitness of the virus [139]. Therefore, in an individual with a transmitted M184 virus, the mutation may not be detected if genotyping occurred after high viral replication in the acute phase where wildtype subpopulations would outcompete the M184 virus. It is important to note that the effect of different mutations at a single codon can vary widely and that combinations of specific mutations can have synergistic effects on treatment resistance. For example, the effect of mutations at V179 on RPV susceptibility depends on the specific substitution. While V179L is listed as a DRM in the RPV package insert [121], V179T has minimal effects on RPV and minimal reductions of RPV sensitivity, and V179F appears to only affect RPV susceptibility in combination with Y181CF [12]. Mutations at codon E138, including E138K/A/Q/G/R, have been associated with a two- to fivefold reduction in susceptibility to RPV [12]. The E138K mutation alone reduces RPV sensitivity two-to threefold, while the combination of E138K and the NRTI DRM M184I can cause a fivefold reduction in sensitivity and virological failure. In addition, E138A is a polymorphic substitution that occurs more frequently in HIV-1 subtype C compared with other subtypes [140]. As a result, the baseline prevalence of the E138A substitution may be higher in regions known to have higher rates of HIV subtype C compared with other regions [12,140]. The M184V/I mutation alone can greatly reduce 3TC susceptibility (>100-fold), and M184V is often associated with 3TC virological failure [12].
One limitation of this review was using specific mutations and country or region names as keywords; doing so may have excluded multinational cohorts and some clinical trials. However, this review analysed >60,000 patients across 48 countries discussed in 127 publications, suggesting that the results and conclusions in this analysis are unlikely to be substantially altered if data from additional similar types of articles were included.
Overall, the rates of pretreatment DRMs were low across geographic regions for NRTIs and NNRTIs as classes and for substitutions at codons associated with resistance to 3TC/FTC and RPV specifically. These data suggest a low risk of resistance to ART regimens containing 3TC/FTC and RPV, supporting the use of 2DRs such as DTG and 3TC (in treatment-naive individuals) and DTG and RPV (in individuals who are virologically suppressed on a 3-drug regimen and are switching to a 2DR).
Footnotes
Acknowledgements
This study was funded by ViiV Healthcare. Literature search and analysis, medical writing and editorial assistance were provided under the direction of the authors by Jonathan Morgan and Diane Neer, ELS, MedThink SciCom (Cary, NC, USA), and funded by ViiV Healthcare.
Author disclosures are as follows: VV, LR, CH, JvW, DB, RQ, MSC, MU, JMG, AdR and MA are employees of ViiV Healthcare and own stock/stock options in GlaxoSmithKline; JD was an employee of ViiV Healthcare during the time of the study and owns stock/stock options in GlaxoSmithKline.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.