
Abstract
Background
Methods
Results
Conclusions
Introduction
HBV infection is one of the most important public health problems in the world. An estimated 240 million people are chronically infected with HBV with a varying prevalence geographically in the world, the highest in Africa and Asia [1]. In China, a meta-analysis showed that hepatitis B surface antigen (HBsAg)-positive rate was 5.7% in the general population aged 1–59 years in 2007–2016 [2], and there were considerable numbers of patients with chronic HBV (CHB) infection due to the large population in China. Guangzhou, as the capital city of Guangdong Province, is one of the most economically developed cities in Southeast China. A community-based study showed the prevalence of positive HBsAg was 8.76% in Guangdong Province in 2014–2015 [3], higher than the national level. Chronically infected individuals are at increased risk of developing hepatic decompensation, cirrhosis and hepatocellular carcinoma (HCC) [4]. These complications substantially reduce the quality of life and life expectancy, as well as imposing great demands on health-care resources [5]. Thus, prevention or delay of disease progression would improve the prognosis and save medical resources [6].
Antiviral treatment can achieve sustained suppression of HBV DNA replication, and then prevent further disease progression [7]. It has been recommended by multiple international guidelines of prevention and treatment for CHB [8–11]. Currently, there are seven agents widely used to treat patients with CHB infection in China, including conventional alpha-interferon (IFN-α), pegylated interferon-alpha-2a (alpha-2b; PEG-IFN-α2a [α2b]), lamivudine (LAM), adefovir dipivoxil (ADV), entecavir (ETV), telbivudine (LdT) and tenofovir (TDF). Several clinical trials have confirmed that the recommended first-line antiviral agents such as ETV and TDF have a potent antiviral effect, low incidence of drug resistance and good safety [12–14]. However, use of the antiviral drugs are impacted by factors like their costs, coverage of reimbursement and others [15,16].
Persistent and normative antiviral therapy will bring a substantial financial burden for HBV-related patients. In this study, we assessed the utilization and costs of antiviral drugs and their affecting factors, which will help optimize standardized protocols for therapy and follow-up management for the patients with HBV infection.
Methods
Data source and study population
We used the electronic medical record databases from the hospital information system of the Guangzhou Eighth People's Hospital and constructed separate retrospective cohorts for outpatients and inpatients with CHB infection. The hospital is the largest specialized infection hospital in Guangdong Province, China.
The target populations of this study were adult inpatients and outpatients with CHB infection and related complications for the period from 1 January 2008 to 31 December 2015. These patients were classified into three disease stages: CHB, cirrhosis (including compensated and decompensated cirrhosis) and HCC. All the patients were identified through clinical diagnosis according to the International Classification of Disease, 10th Revision (ICD-10). Patients coinfected with hepatitis A, hepatitis C, hepatitis D, hepatitis E, HIV infection or cytomegalovirus (CMV) infection were excluded from this study. Patients admitted to the hospital due to pregnancy or diseases including glomerulonephritis, uraemia, metabolic syndrome, tumour and severe cardiovascular diseases were excluded. The details of sampling and data collection are shown in Figure 1.

Flowchart of records selection
Study variables
Demographic characteristics, treatment of CHB infection and associated costs were extracted from electronic medical records for all the patients. The demographic information of patients such as age, gender, payment mode, admission (or visit) date and disease stage were included in our analysis datasets. Payment mode was categorized into four groups: self-payment, medical insurance, free medical service and other insurance. Antiviral treatment was defined as a patient prescribed at least one kind of antiviral drugs in the year of clinic visit or hospital admission. According to the frequencies of the drug use, we combined IFN with PEG-IFN-α2a and separated the made-in-China adefovir dipivoxil (ADV_C). The subjects prescribed any of the seven antiviral drugs (IFN, ETV, ADV, LAM, LdT, TDF and ADV_C) were considered as users of antiviral drugs. The proportion of utilization of each of seven antiviral drugs was computed as the number of patients treated for a particular antiviral drug divided by the total number of patients in a year for the study period. A user of hepato-protective drugs and traditional Chinese drugs was defined as a patient who was prescribed at least one kind of the drugs in the year of visit/admission. The types of hepato-protective and traditional Chinese medicines included were determined after consulting with senior clinicians. Annual direct medical costs and annual costs for antiviral drugs were calculated by accumulating the expenses of all hospital admissions (or clinic visits) during the year. In this study, the direct medical costs included items of laboratory tests and imaging examinations, antiviral drugs and other medicines including liver protector or traditional Chinese medicine, bed and nursing (only for inpatients), registration and consultation (only for outpatients), radiation therapy, anaesthesia, surgery and blood transfusion (only for inpatients). The cost of each antiviral drug used was estimated separately and annual expected cost of each antiviral drug was also estimated based on the price published on the Chinese medicine price network [17], assuming that patients were given standardized treatment. There are multiple specifications and dosages for each type of antiviral drugs, and the Chinese medicine price network lists a range of unit price for each drug. An interval for the annual expected costs for each drug was provided based on this range of unit price. All costs were expressed in RMB in the year of 2015 and were adjusted by a discount rate of 5% per year [18,19].
Statistical analyses
The distributions of person-years (based on calendar year) were described according to demographic characteristics of inpatients and outpatients including age, gender, payment mode, year of visit/admission and disease stage. Meanwhile, expenditure data of antiviral therapy were typically right-skewed and zero-inflated because many patients did not use antiviral drugs and ordinary least squares estimation is usually biased and inefficient because of this. We used a two-part model approach [20] to simultaneously model the probability of antiviral utilization and costs of antiviral therapy [21,22]. In the first part, a logistic regression model was used to estimate the probability of antiviral drug utilization. The ORs and their 95% CIs were used to describe the association of relevant factors with antiviral drug utilization. The second part estimated the nonzero antiviral expenditures for the antiviral drug users using a generalized linear model with a gamma distribution and a log link. The cost ratios (CR) and their 95% CIs were used to analyse the difference in antiviral drug expenditures among patients with different characteristics. The method of maximum likelihood estimation was used to estimate the ORs and the CRs in two-part models. In addition, we also described average annual costs for antiviral drugs and the proportion in direct medical costs for patients by different disease stages. The cost of each antiviral drug and the expected cost of normative treatment based on the Chinese medicine price network [17] were also compared. All statistical analysis was conducted separately for outpatients and inpatients using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and P<0.05 was considered statistically significant.
Results
Descriptive characteristics
A total of 14,920 records from 12,433 inpatients and 143,658 records from 22,802 outpatients were involved in the analysis. Among the inpatients, the mean age was 42.1 ±14.6 years old, and 11,405 (76.44%) were male and 3,515 (23.56%) were female. There were 105,195 (73.25%) male and 38,410 (26.75%) female outpatients with mean age of 38.1 ±13.0 years. Self-payment and medical insurance were the main payment modes. Approximately 53% inpatients and 86% outpatients visited/admitted to hospital due to CHB. Table 1 shows the distribution of person-years (based on calendar year) according to the study variables. The median number of visits/admissions per case per year was 1 for inpatients and 3 for outpatients.
Distribution of PY (based on calendar year) according to the characteristics of patients

Including commercial insurance and cooperative medical service, etc. CHB, chronic hepatitis B; HCC, hepatocellular carcinoma; PY, person-years.
Antiviral drug utilization and expenditures using two-part model
The overall annual antiviral drug utilization for inpatient and outpatients were 56.99% and 45.65%, respectively. The annual proportion of antiviral drug utilization increased from 45.61% in 2008 to 62.60% in 2015 for inpatients, and from 29.44% to 53.99% for outpatients. More than half of inpatients with CHB (54.63%, 4,308/7,886), 64.03% (2,896/4,523) of inpatients with cirrhosis and 56.31% (1,414/2,511) of HCC inpatients had received antiviral treatment. For outpatients, antiviral drugs were taken by 43.44% (53,358/122,841) for CHB, 60.14% (11,641/19,357) for cirrhosis and 39.66% (579/1,460) for HCC.
Tables 2 and 3 present the results from the two-part models for inpatients and outpatients, respectively. Table 2 shows the annual proportion of antiviral drug utilization in the first part of the model. A higher probability of antiviral drug utilization was observed in male and older inpatients. Inpatients with medical insurance and free medical service were more likely to use antiviral drugs than self-payment inpatients, with the ORs (95% CI) being 1.11 (1.03, 1.19) and 1.24 (1.13, 1.36), respectively. As compared with inpatients with CHB, cirrhosis inpatients were more likely to use antiviral drugs (OR=1.18, 95% CI: 1.06, 1.30). Inpatients receiving traditional Chinese medication had a higher proportion of antiviral drug use than those who did not (OR=2.00, 95% CI: 1.83, 2.18). The second part was used to estimate the annual average expenditures of antiviral drug treatment among inpatients prescribed antiviral drugs. Women and young inpatients had higher antiviral drug expenditures than men and old inpatients. Inpatients with free medical service had a 1.32-fold higher expenditure than inpatients with self-payment. However, inpatients with medical insurance had a lower expenditure than those with self-payment (OR=0.79; 95% CI: 0.75, 0.84). Inpatients receiving traditional Chinese medicine and hepato-protective drugs had a 1.30-fold and 1.14-fold higher antiviral drug expenditure than inpatients who did not. Annual average antiviral drug costs for inpatients increased first and then decreased for the period from 2008 to 2015.
Utilization of antiviral drugs and corresponding annual antiviral drugs costs and associated factors for inpatients

n, the number of antiviral drug use. b Description: RMB (yuan). CHB, chronic hepatitis B; HCC, hepatocellular carcinoma; OR, odds ratio.
Utilization of antiviral drugs and corresponding annual antiviral drugs costs and associated factors for outpatients

n, the number of antiviral drug use.
Description: RMB (yuan). CHB, chronic hepatitis B; HCC, hepatocellular carcinoma; OR, odds ratio.
Table 3 showed male and older outpatients had a higher probability of antiviral drug utilization. It was also seen that outpatients with medical insurance were more likely to use antiviral drugs than self-payment outpatients (OR=1.66, 95% CI: 1.59, 1.73). Outpatients who used hepato-protective drugs had a lower proportion of antiviral use than those who did not (36.00% versus 51.30%; OR=0.44, 95% CI: 0.42, 0.46). As compared with outpatients with CHB, outpatients with cirrhosis were more likely to use antiviral drugs (OR=1.58, 95% CI: 1.53, 1.63). Among outpatients with antiviral drug expenditure, men had higher antiviral drug expenditures than women. As compared with outpatients with self-payment, outpatients with medical insurance had a 1.07-fold higher antiviral drug expenditure. Furthermore, outpatients receiving traditional Chinese medicine had a higher antiviral drug expenditure but those receiving hepato-protective drugs had a lower antiviral drug expenditure than outpatients who did not, respectively. Outpatients with more hospital visits had a higher probability of antiviral drug use and higher antiviral drug costs.
Proportion of utilization and annual expenditure for each antiviral drug
As shown in Figure 2, IFN, ETV, LAM and ADV_C were the primary antiviral drugs for inpatients and outpatients. From 2008 to 2015, the annual proportion of utilization for IFN dropped from 57.16% to 8.71% for inpatients and from 24.77% to 3.25% for outpatients, whereas the proportion for ETV gradually increased from 11.08% to 70.26% for inpatients and from 11.05% to 49.35% for outpatients, respectively. In addition, the proportion of ADV_C utilization increased initially from 10.14% in 2008 to 19.35% in 2011 and then decreased gradually to 9.24% in 2015. For outpatients, however, it remained at a higher level from 2008 to 2015. The proportion of LAM utilization increased from 2008 to 2011 and then gradually decreased for both in- and outpatients.

Utilization prevalence of antiviral drugs for inpatients and outpatients using antiviral drugs from 2008 to 2015
Figure 3 showed annual average actual costs for inpatients and outpatients using various antiviral drugs during the 8-year period and the corresponding annual expected costs when normative antiviral therapy was assumed. Annual expected costs range from 11,260 to 13,766 RMB for ETV and 5,292 to 6,474 RMB for TDF. However, actual annual costs were about 5,000 RMB for outpatients using ETV and about 5,500 RMB for TDF (only the years of 2013, 2014 and 2015, because this drug was launched in 2013) from 2008 to 2015. The actual costs were far less than the annual expected costs for outpatients who received ETV treatment. Less than 40% of patients whose annual actual antiviral costs achieved the expected costs of normative therapy were found in outpatients (Table 4).
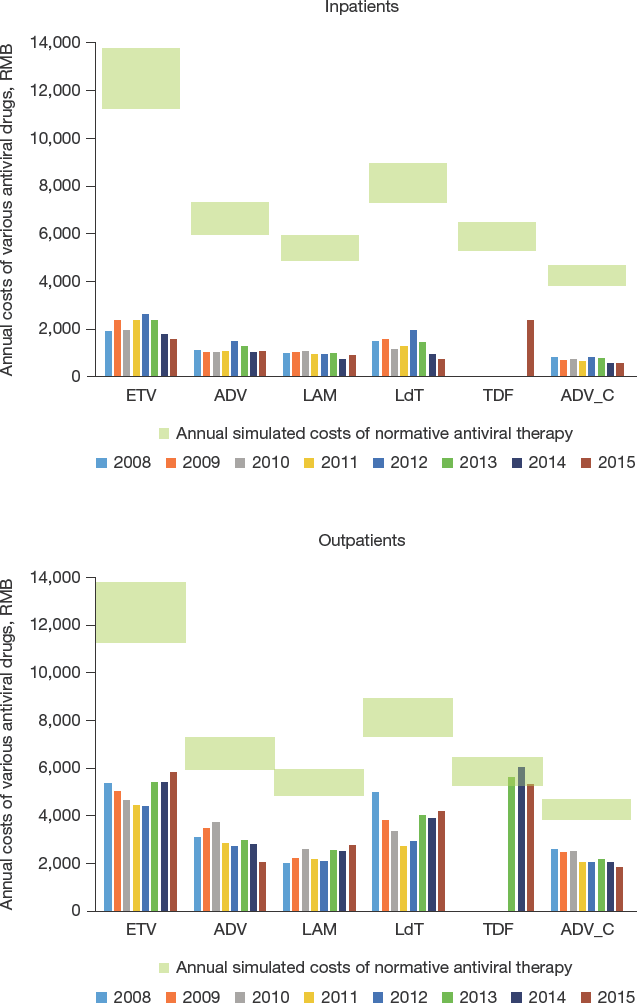
Annual average costs of various antiviral drugs for inpatients and outpatients from 2008 to 2015 and annual expected costs of normative antiviral therapy
The proportion of outpatients whose annual actual antiviral costs achieved the annual expected antiviral costs of normative therapy from 2008 to 2015 (%)

ADV, adefovir dipivoxil; ADV_C, made-in-China adefovir dipivoxil; ETV, entecavir; LAM, lamivudine; LdT, telbivudine; TDF, tenofovir disoproxil fumarate.
The proportion of annual antiviral drug costs in average annual direct medical costs
Figure 4 summarized annual average direct medical costs and the proportion of annual average antiviral drug costs for patients in different disease stages for the period from 2008 to 2015. The annual direct medical costs for inpatients and outpatients were as follows: CHB: 16,439.84 and 6,800.56 RMB; cirrhosis: 25,379.39 and 8,156.47 RMB; HCC: 33,371.09 and 6,831.00 RMB, respectively. Among them, antiviral drug costs represented 13.91% and 71.29% of direct medical costs for inpatients and outpatients with CHB, respectively. And with the progress of disease, this proportion decreased to 4.07% for HCC inpatients and 49.29% for HCC outpatients.

The annual average direct medical costs and the proportion of antiviral drugs costs in direct medical costs for inpatients and outpatients by different disease stages
Discussion
In the present study, using electronic medical data from the largest specialized infection hospital in Guangdong, China, antiviral drug utilization for 14,920 inpatients and 143,658 outpatients with CHB infection were analysed for the period from 2008 to 2015. Nearly half of the infected patients did not receive antiviral treatment in Guangzhou. The overall proportion of antiviral drug utilization was 56.99% for inpatients and 45.65% for outpatients. However, the proportion of antiviral drug utilization increased every year, including ETV and TDF, as the first-line antiviral drugs [8–11].
Antiviral treatment can achieve sustained suppression of HBV DNA replication, and slow disease progression. The WHO Global Health Sector Strategy on Viral Hepatitis with the purpose of an elimination of HBV in 2030, targets to provide antiviral treatment for 80% of those diagnosed and eligible for treatment [23]. China has the largest number of patients with hepatitis B infections in the world. However, a large number of the patients did not receive antiviral treatment in this country. Research form Beijing You'an Hospital in 2008–2012 and from 10 hospitals in western China in 2011 also demonstrated a low proportion of using antiviral drugs [24,25]. This phenomenon was also observed in some Western countries. A study of electronic health records in the United States found that antiviral therapy was received by 57.90% of HBV-infected patients [26]. It was even lower (25%) in Belgium [27]. One possible explanation was that there were increased numbers of patients with HBV infection who did not meet antiviral indications in areas with a low prevalence. It was a concern that only 5% of individuals eligible for treatment actually received antiviral therapy globally, and this rate was about 11% in China [28].
Given the importance of antiviral therapy in patients with CHB infection, it is imperative to identify the influencing factors of antiviral therapy. From the perspective of macro-management, reimbursement policy is the most critical positive factor. In this study, the antiviral utilization increased in inpatients with medical insurance more than those with self-payment. A study by Liaw [7] revealed that lack of reimbursement for treatment is an obstacle to the proper management of HBV disease. Another study from South Korea also showed that the number of patients receiving oral antiviral therapy for HBV precipitously increased since life-long reimbursement of oral antiviral agents was approved [29]. Since 2008, health insurance policy has experienced a series of changes in Guangzhou. The Outpatient Medical Insurance Fund Policy was implemented in Guangzhou on 1 August 2008 that provided a monthly quota payment for patients. Until 1 October 2013, both urban and rural residents were paid with CHB patients receiving 100 RMB per month by this Fund. The payment increased to 400 RMB per month on 1 January 2015. In this study, the effect of reimbursement policy on the proportion of antiviral drug use tended to increase with time, especially for first-line treatment drug ETV. IFN and NAs (ETV, ADV, LAM and LdT) have been listed on the National Reimbursement Catalog of Drugs for Basic Medical Insurance since 1 July 2011, which increases the affordability as well as allows patients to use more expensive drugs such as first-line treatment drug ETV, which offered better therapeutic efficacy, and fewer side effects and drug resistance [5,30]. Therefore, medical insurance optimized the availability of antiviral drugs. Additionally, in May 2016, TDF was included in the National Medical Insurance, which would significantly increase the use of first-line antiviral drugs, which needs to be further evaluated. In addition to the effect of reimbursement policy, our results showed that outpatients receiving hepato-protective drugs were less likely to use antiviral drugs than outpatients who did not receive hepato-protective drugs.
WHO estimated that the most important part of the total costs was hepatitis screening fees and antivirus treatment costs for CHB in low and middle-income countries [31]. In this study, the costs of antiviral therapy were an important part of the economic burden, especially in the early stage of disease progression. Annual average antiviral drug costs for outpatients with CHB was 4,848.03 RMB, and it accounted for 71.29% of annual direct medical costs. When the disease progresses to HCC, the hospitalization risk increases and the medical costs also increase substantially [32–34]. The annual direct medical cost for HCC inpatients was 3,3371.09 RMB, but the antiviral drugs accounted for only 4.07%. Normative antiviral therapy in early stage of disease progression slows down the disease progression, improves the quality of life and reduces other medical expenses caused by disease progression. However, we found that the actual annual antiviral drug costs were significantly lower than normative treatment costs based on the Chinese medicine price network [17]. Taking TDF as an example, less than 40% of outpatients with antiviral drug treatment achieved the expected costs of normative therapy. This may be related to poor persistence and adherence of patients. A large-scale study of patient adherence with antiviral therapy for CHB infection reported a persistence rate of 85.5% in the United States [35]. In China, the adherence rate to antiviral therapy in China is far from optimistic [36]. Non-adherence can result in poor virology suppression, breakthrough resistance and progression of disease [37].
This study included a large study population from 8-year retrospective inpatient and outpatient cohorts and used novel two-part model methodology. However, there are some limitations. First, there were possible selection biases in our study, owing to study individuals coming from one hospital. However, the Guangzhou Eighth People's Hospital is the largest specialized infection hospital in Guangdong Province, and most patients with HBV-related diseases would usually seek their medical care services from large hospitals rather than county-level hospitals and community clinics [38]. Our study population had a similar distribution of demographic characteristics of subjects as compared with others [16,32,34]. Second, there was a lack of information on other influencing factors at the individual level, such as education, household income and lifestyle. Third, we were not able to distinguish between treatment-naive patients (patients who had not received antiviral therapy before the study) and treatment-experienced patients (patients who had received antiviral therapy before the study), thus initiation, switch or add-on treatments were not considered and compared with established guidelines in this study. Fourth, HCC patients were likely to be underrepresented since it is not a cancer hospital.
In conclusion, nearly half of the patients with CHB infection received antiviral treatment from 2008 to 2015 in Guangzhou, China. The proportion of antiviral drug utilization increased annually, especially ETV and TDF as first-line treatment drugs. Reimbursement policy was the most important factor affecting antiviral treatment. The costs of antiviral therapy were an important part of the direct medical costs, especially in the early stage of disease progression. However, the actual annual average costs of antiviral drugs were lower than expected, suggesting that the dosage of antiviral drugs might not be enough for patients with antiviral therapy.
Footnotes
Acknowledgements
Funding: this study was supported by the National Natural Science Foundation of China (No.71573059); and The Medical Scientific Research Foundation of Guangdong Province, China (No. A2017036).
No conflict of interest exits in the submission of this manuscript, and manuscript is approved by all authors for publication.