
Abstract
We read with interest the review by Adinolf et al. [1] highlighting the need to evaluate all persons with HCV infection for diabetes, in view of extrahepatic benefits of viral eradication, the reduced risk of diabetic complications and improved glyco-metabolic control in HCV-infected patients. Previous studies have shown that HCV impairs glucose metabolism directly via viral proteins and indirectly by altering pro-inflammatory cytokine levels [2–4]; thus, in turn, HCV clearance may positively impact on glucose metabolism, as evidenced by decreased mean haemoglobin A1c (HbA1c) and fasting plasma glucose (FPG) levels [5,6] in diabetic patients exposed to new direct-acting antiviral (DAA) agents that produce a sustained virological response (SVR) in nearly all cases. However, there are limited data on the effect of viral eradication with DAAs on established type 2 diabetes (T2DM) and whether the benefits are persistent [7,8].
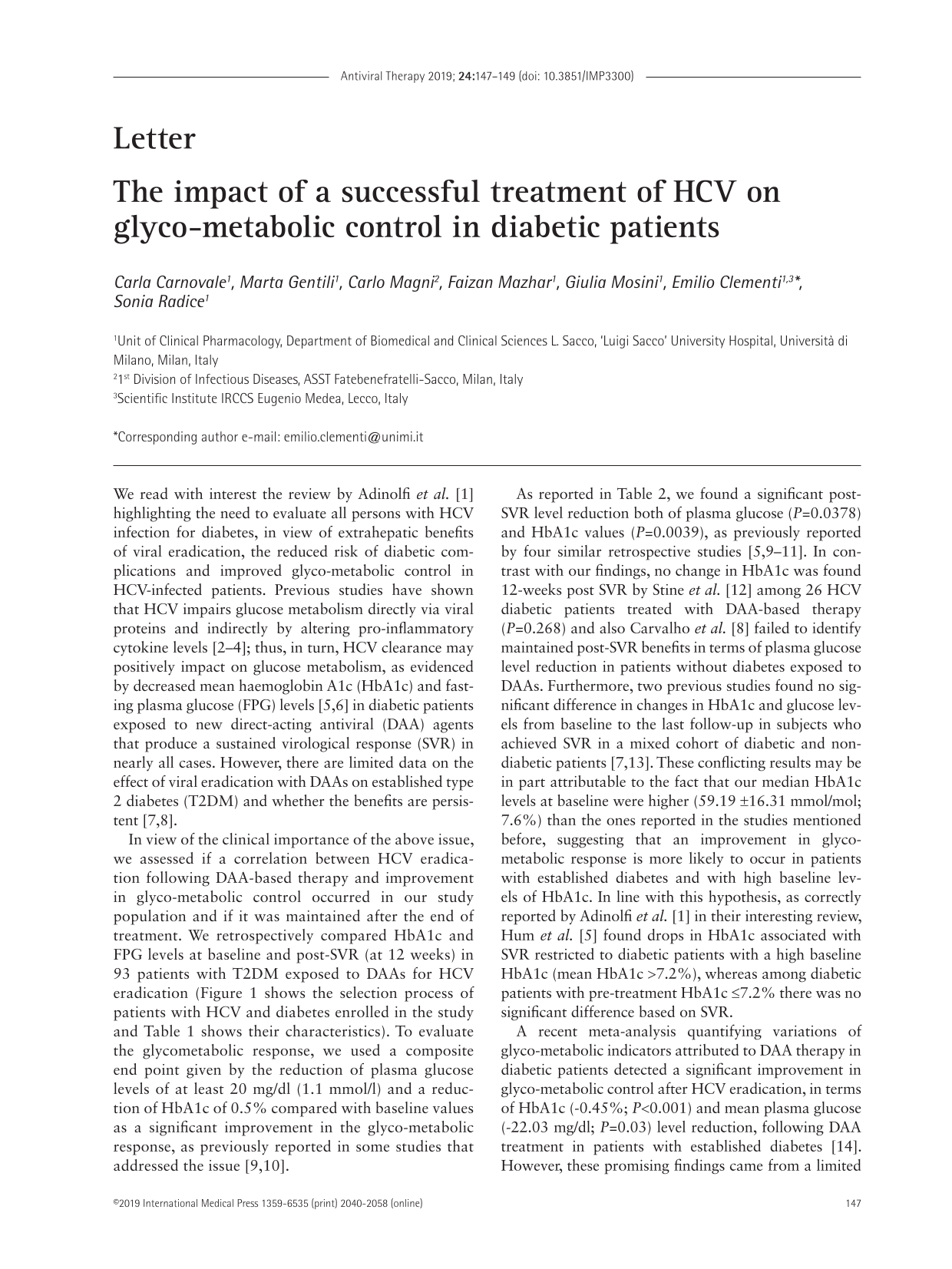
In view of the clinical importance of the above issue, we assessed if a correlation between HCV eradication following DAA-based therapy and improvement in glyco-metabolic control occurred in our study population and if it was maintained after the end of treatment. We retrospectively compared HbA1c and FPG levels at baseline and post-SVR (at 12 weeks) in 93 patients with T2DM exposed to DAAs for HCV eradication (Figure 1 shows the selection process of patients with HCV and diabetes enrolled in the study and Table 1 shows their characteristics). To evaluate the glycometabolic response, we used a composite end point given by the reduction of plasma glucose levels of at least 20 mg/dl (1.1 mmol/l) and a reduction of HbA1c of 0.5% compared with baseline values as a significant improvement in the glyco-metabolic response, as previously reported in some studies that addressed the issue [9,10].
Baseline demographics for HCV patients with diabetes
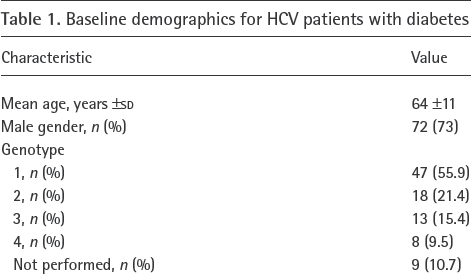
Selection process of patients with HCV and diabetes enrolled in the study
As reported in Table 2, we found a significant post-SVR level reduction both of plasma glucose (P=0.0378) and HbA1c values (P=0.0039), as previously reported by four similar retrospective studies [5,9–11]. In contrast with our findings, no change in HbA1c was found 12-weeks post SVR by Stine et al. [12] among 26 HCV diabetic patients treated with DAA-based therapy (P=0.268) and also Carvalho et al. [8] failed to identify maintained post-SVR benefits in terms of plasma glucose level reduction in patients without diabetes exposed to DAAs. Furthermore, two previous studies found no significant difference in changes in HbA1c and glucose levels from baseline to the last follow-up in subjects who achieved SVR in a mixed cohort of diabetic and non-diabetic patients [7,13]. These conflicting results may be in part attributable to the fact that our median HbA1c levels at baseline were higher (59.19 ±16.31 mmol/mol; 7.6%) than the ones reported in the studies mentioned before, suggesting that an improvement in glyco-metabolic response is more likely to occur in patients with established diabetes and with high baseline levels of HbA1c. In line with this hypothesis, as correctly reported by Adinolfi et al. [1] in their interesting review, Hum et al. [5] found drops in HbA1c associated with SVR restricted to diabetic patients with a high baseline HbA1c (mean HbA1c >7.2%), whereas among diabetic patients with pre-treatment HbA1c ≤7.2% there was no significant difference based on SVR.
Effect of treatment of HCV with DAAs on glyco-metabolic parameters

Statistical significance assessed by paired Student's t-test. P-values <0.05 were considered statistically significant (bold font). DAA, direct-acting antiviral.
A recent meta-analysis quantifying variations of glyco-metabolic indicators attributed to DAA therapy in diabetic patients detected a significant improvement in glyco-metabolic control after HCV eradication, in terms of HbA1c (−0.45%; P<0.001) and mean plasma glucose (−22.03 mg/dl; P=0.03) level reduction, following DAA treatment in patients with established diabetes [14]. However, these promising findings came from a limited number of studies performed in a wide variety of clinical settings and need to be confirmed.
In conclusion, an increasing amount of evidence seems to suggest that the eradication of HCV with DAA therapy may play a role in improving glycaemic control in patients with established T2DM, highlighting the need to explore the issue through more wide-ranging studies, with a more complete baseline assessment and a prolonged follow-up, with a view to a possible tapering of anti-diabetic drugs in order to avoid hypoglycaemic events.
Footnotes
Acknowledgment
This study was supported by the Agenzia Italiana del Farmaco (AIFA; to EC), by the Centre of Pharmacovigilance of Regione Lombardia (MEAP project, Monitoraggio degli Eventi Avversi nelle Popolazioni a Rischio, to EC).
The authors declare no competing interests.