
Abstract
Background
Active illicit drug use can present a barrier to the medical management of HIV infection by complicating adherence to antiretroviral therapy (ART). Plasma HIV-1 RNA viral load (VL) rebound, defined as a period of detectable HIV VL following ART and VL suppression, can lead to the generation of viral resistance and potential treatment failure. We sought to investigate the contribution of substance use patterns on rates of VL rebound.
Methods
We used data from the ACCESS study, a long-running community-recruited prospective cohort of HIV-positive people who use illicit drugs in Vancouver, Canada, a setting of universal no-cost HIV treatment. We analysed time to VL rebound (that is, two consecutive observations ≥1,000 copies/ml) after ART initiation and sustained viral suppression (that is, two consecutive observations <50 copies/ml) using extended Cox regression models with a recurrent events framework.
Results
Between May 1996 and November 2013, 564 ART-exposed participants achieved at least one instance of VL suppression and contributed 1,893.8 person-years of observation. Over follow-up, 198 (35.1%) participants experienced ≥ one instance of VL rebound. In adjusted analyses, VL rebound was associated with younger age (adjusted hazard ratio [AHR] =0.97, 95% CI: 0.95, 0.98), heroin injection (≥ daily versus < daily, AHR =1.52, 95% CI: 1.01, 2.30), crack use (≥ daily versus < daily, AHR = 1.73, 95% CI: 1.08, 1.92) and heavy alcohol use (≥ four versus < four drinks/day, AHR =1.97, 95% CI: 1.17, 3.31).
Conclusions
The present study suggests that in addition to heavy alcohol use, high-intensity illicit drug use, particularly ≥ daily heroin injection and ≥ daily crack smoking are risk factors for VL rebound. In addition to the impact of high-intensity drug use on health-care engagement and ART adherence, some evidence exists on the direct impact of psychoactive substances on ART metabolism and the natural progression of HIV disease. At-risk individuals should be provided additional supports to preserve virological control and maintain the benefits of ART.
Introduction
People who inject drugs (PWID) are disproportionately impacted by the HIV/AIDS pandemic, accounting for nearly one-third of new HIV infections outside of sub-Saharan Africa [1]. According to a survey of 74 countries by the Joint United Nations Programme on HIV/ AIDS in 2014, PWID were 28x more likely to be living with HIV than the general adult population [2].
The advent of combination antiretroviral therapy (ART) has not only led to dramatic improvements in morbidity and mortality among those living with HIV but recent findings confirm it is highly efficacious at minimizing onward transmission of HIV [3–5]. Ongoing initiatives to control the HIV pandemic are focused, in part, on scaling up access and long-term adherence to ART in order to promote sustained viral load (VL) suppression [1,6]. Unfortunately, studies among HIV-positive PWID commonly report high rates of suboptimal access and adherence to ART [7–9]. There remains a need to further elucidate the longitudinal patterns of HIV VL over time and identify risk factors for loss of virological control in this population.
To date, studies have described elevated rates of VL rebound, commonly defined as two consecutive observations ≥1,000 copies/ml following sustained virological suppression, among people who use illicit drugs [10–12]. However, the relative impact of different drug types and routes of administration on VL rebound remains unclear. In Vancouver, Canada, poly-substance use (for example, injection heroin, injection cocaine, crack cocaine smoking, crystal methamphetamine use and alcohol consumption) is common among illicit drug users living with HIV. This setting also features a combination HIV prevention and treatment initiative, including HIV treatment guidelines which recommend immediate initiation of ART upon diagnosis, as well as universal no-cost ART. Thus, this study aims to examine substance use patterns and their longitudinal impacts on VL rebound among ART-experienced PWID in Vancouver, Canada.
Methods
For these analyses, we used data collected as part of the AIDS Care Cohort to evaluate Exposure to Survival Services (ACCESS), an observational prospective cohort of HIV-positive illicit drug users in Vancouver, Canada. The study has been described in detail previously [13–15]. Briefly, community-based strategies, including snowball sampling and extensive street outreach, were used to recruit HIV-positive illicit drug users in the city's Downtown Eastside (DTES) neighbourhood, an area with high levels of illicit drug use, poverty, homelessness and rates of blood-borne pathogens, including HIV and HCV. Individuals were eligible for inclusion if they were HIV-seropositive as demonstrated by serology, aged ≥18 years, and used illicit drugs other than or in addition to cannabis in the 30 days prior to the baseline interview. The ACCESS study has been approved by the University of British Columbia/Providence Healthcare Research Ethics Board. All participants provide written informed consent.
Following study recruitment, all ACCESS participants complete an interviewer-administered survey, which elicits information on lifetime and recent characteristics, behaviours and exposures. They also undergo an examination by a study nurse, including the provision of a blood sample for analysis. At recruitment, individuals provide their personal health number, a unique and persistent identifier issued for medical billing and tracking purposes to all residents of the province of British Columbia. Using this identifier, study staff established a confidential linkage with the British Columbia Centre for Excellence in HIV/AIDS (BCCfE) Drug Treatment Programme (DTP). Through the DTP, the BCCfE provides HIV treatment and care including all medications and clinical monitoring to all individuals living with HIV in the province through the no-cost universal medical system. A complete retrospective and prospective clinical profile is available for all ACCESS participants through this linkage. This profile includes all VL observations and CD4+ T-cell counts conducted through the study or as a part of ongoing clinical care, if any. In addition, this linkage contains records from the DTP's pharmacy, the province's sole source of ART, including data on antiretroviral agent, dose and date dispensed.
In this study, we included all individuals who were exposed to ART at baseline or who initiated ART over the study period; had at least one observation of CD4+ T-cell count and VL within 12 months of recruitment; and had at least two consecutive measurements indicating non-detectable VL following ART initiation prior to the end of the study period. Because the sensitivity of the VL assays changed over the study period, we defined suppression as any measurement below 500 copies/mm3 before 1 April 1999 and any measurement below 50 copies/mm3 after 1 April 1999. For all individuals included in these analyses, time zero was defined as the date of the first interview following the second measurement indicating virological suppression. The primary outcome of interest was confirmed VL rebound, defined as the date of the first of two consecutive measurements of VL above 1,000 copies/ml. This approach was consistent with a previous study on social and structural-level predictors of VL rebound from our setting [10].
Our primary explanatory variables of interest detailed specific patterns of substance use common in this setting: injection heroin use (≥ daily versus < daily); injection cocaine use (≥ daily versus < daily); injection crystal methamphetamine (≥ daily versus < daily); non-injection crack cocaine use (≥ daily versus < daily); and heavy alcohol use (defined as ≥ four drinks/day on average in the last 6 months versus < four drinks). We also considered a number of secondary explanatory variables including: self-reported gender (male versus non-male); self-reported ancestry (White versus non-White); age at baseline (per year older); education (high school completion or higher versus < high school); living in unstable housing (defined as living on the streets or with no fixed address, a shelter, a treatment centre or single-room occupancy hotel room versus an apartment or house); CD4+ T-cell count (per 100 cells/ml); experience of the participant's HIV physician, defined as in previous analyses [16] as the number of individuals their physician had previously initiated on ART, dichotomized at < six versus ≥ six patients; and ART adherence, dichotomized as ≥95% versus <95%. This validated measure of ART adherence is based on pharmacy refill records using data accessed from the DTP, as described above. For each observation period, we calculated the numerator as the number of days between the date of interview and the date of ART initiation, capped at 180. The numerator was the number of days within that period in which pharmacy records indicate ART was dispensed. We dichotomized the resulting proportion at >95% versus ≤95%. For each 6-month study period, we defined the CD4+ T-cell count as the mean of all observations in the period; or, if none, we used the most recent observation.
As a first step, we compared all participants by the explanatory variables at baseline stratified by whether they experienced an HIV VL rebound over follow-up using Pearson's χ 2 test (for categorical variables) and Wilcoxon rank-sum test (for continuous variables). Next, we built extended Cox models to estimate the relative hazard of VL rebound associated with each explanatory variable. As a final step, we fit a multivariable extended Cox model using an a priori model-building procedure based on backwards selection guided by Akaike Information Criterion (AIC) values. All Cox models incorporated a recurrent events framework in which observations were censored from the first of two VL measurements defining the event to the next period of VL non-detectability.
A sensitivity analysis was performed to evaluate whether substance use, irrespective of frequency (that is, any versus none) was associated with time to VL rebound. Univariate analysis comparing each substance and the outcome variable, enabled assessment of their possible confounding effect. In addition, we performed a sensitivity analysis to estimate the relationships between ≥ daily substance use patterns and HIV VL rebound including ART adherence, as defined above.
Results
Between May 1996 and November 2013, we recruited 1,086 participants into the study. A total of 857 (79%) were ART-exposed prior to the end of the study period. Of these, 564 individuals (66%) had two consecutive VL observations indicating suppression following recruitment into the study and thus were included in the analyses. Over the study period, the 564 individuals contributed 1,893.8 person-years of follow-up with a median follow-up time of 34.2 months (IQR 17.0-54.8) per participant. 198 participants (35.1%) experienced at least one instance of VL rebound over the follow-up period.
Table 1 presents baseline characteristics of participants, stratified by viral rebound over the study period. Of note, participants who were younger in age, with less than a high school education and who reported ≥ daily heroin injection at baseline, were more likely to experience VL rebound over the follow-up.
Baseline characteristics of 564 HIV-positive illicit drug users stratified by HIV-1 RNA VL rebound over follow-up in Vancouver, Canada

Values are mean (IQR) or n (%) unless otherwise indicated.
Based on current status.
Measured at baseline.
Time-updated referring to the last 6 months.
Statistically significant P<0.05. ART, antiretroviral therapy; MA, methamphetamine; VL, viral load.
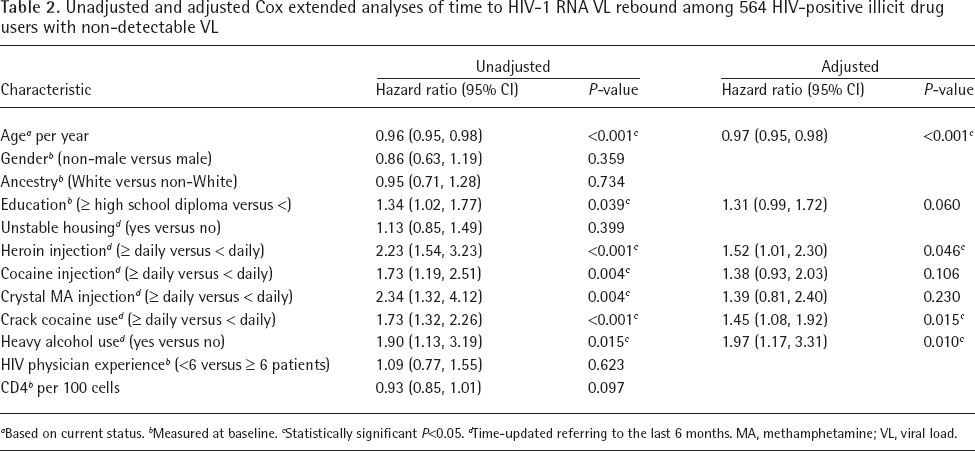
Table 2 presents the results of bivariate and multivariate extended Cox regression analyses. In multivariate analysis, factors that were positively associated with time to VL rebound included: ≥ daily injection heroin use (adjusted hazard ratio [AHR] = 1.52; 95% CI = 1.01, 2.30); ≥ daily non-injection crack use (AHR = 1.45; 95% CI: 1.08, 1.92); and heavy alcohol use (AHR = 2.49; 95% CI: 1.17, 3.31). Conversely, age was the only factor negatively associated with time to VL rebound (AHR = 0.97; 95% CI: 0.95, 0.98). Of note, ≥ daily use of injection cocaine and ≥ daily crystal methamphetamine injection were not associated with time to VL rebound in the adjusted analysis.
Unadjusted and adjusted Cox extended analyses of time to HIV-1 RNA VL rebound among 564 HIV-positive illicit drug users with non-detectable VL
Based on current status.
Measured at baseline.
Statistically significant P<0.05.
Time-updated referring to the last 6 months. MA, methamphetamine; VL, viral load.
In the first sensitivity analysis (Additional file 1), we repeated our analyses with different measures of substance use frequency. In these analyses, heroin injection in the last 6 months (any versus none) was associated with swifter time to viral rebound in both crude (HR = 1.40, 95% CI: 1.12, 1.75) analyses and a multivariable model (AHR = 1.38, 95% CI: 1.11, 1.72) also adjusted for baseline age and baseline CD4+ T-cell count. No other measure of substance use (that is, cocaine injection [any versus none in the last 6 months]; methamphetamine injection [any versus none in the last 6 months]; crack smoking [any versus none in the last 6 months]; and alcohol use [any versus none in the last 6 months]) were associated with time to viral rebound in crude analyses nor were they included in the multivariable model.
To test the relationship between substance use, ART adherence and viral rebound, we built a second multivariable model including the term for ART adherence. In this model (Additional file 2), we observed ART adherence was crudely associated with longer time to rebound (HR = 0.23, 95% CI: 0.18, 0.29). In a multivariable model including ART adherence, age (AHR = 0.97, 95% CI: 0.96, 0.99) and ART adherence remained negatively associated with time to VL rebound while ≥ daily heroin injection (AHR = 1.65, 95% CI: 1.16, 2.36) was associated with shorter time to rebound. CD4+ T-cell count, ≥ daily cocaine injection and ≥ crystal methamphetamine injection were not associated with time to VL rebound.
Discussion
In this study, we observed that loss of virological control following suppression was common, with just over one-third (35.1%) of study participants experiencing at least one episode of VL rebound over an average of approximately 3 years of observation. We also detailed the contribution of different types of drugs and routes of administration on rates of rebound. Specifically, we showed an increased likelihood of treatment failure among individuals who reported high-intensity use of crack cocaine, alcohol or heroin via injection.
Our findings are in line with previous research which has described the deleterious impact of substance use on health-care engagement, ART adherence and HIV disease progression. The use of crack cocaine among HIV-positive individuals has gained substantial attention over the years as an independent predictor of AIDS-related mortality, HIV progression and development of AIDS-defining illnesses, independent of ART adherence [17,18]. Compared to non-users, Cook et al. [19] found women who use crack cocaine to be 3.6x more likely to die from AIDS-related causes when controlling for self-reported ART adherence and other forms of substance use, including heroin, cocaine and alcohol. Similarly, Duncan et al. [20] found increased crack cocaine use or urinary cocaine levels to be associated with lower CD4+ T-cell counts for a given HIV VL. The differential impact of crack cocaine relative to other drugs has been explained in both in vitro and animal-based studies wherein crack cocaine was found to be a potent immunosuppressant, inhibiting neutrophil and macrophage function [21], while at the same time, promoting HIV replication [22]. The consequential acceleration of disease progression has obvious implications in terms of both clinical management and minimizing viral transmission. As no effective pharmacotherapy exists for individuals with stimulant use disorder, our findings reinforce the need for additional social and clinical supports for HIV-positive people who use cocaine.
By contrast, the specific impact of heroin on HIV progression is less well-understood [22,23]. Much of the investigation of heroin's effects are derived from studies of morphine, of which it is a pro-drug. These studies have demonstrated promotion of HIV-1 growth in cell cultures [24,25], induced lymphocyte apoptosis [26] and increased expression of HIV-1 entry co-receptor with increased HIV replication [27,28]. However, animal and human studies have been inconsistent in their findings on the impact of heroin use [29–34]. More studies are needed to better understand heroin's role on HIV disease progression.
Alcohol use disorders are highly prevalent and intrinsically tied to the HIV pandemic. Though few participants in our study (4.4%) endorsed excessive alcohol use (defined as >4 drinks/day during the last 6 months) it was an independent predictor of VL rebound. Prior studies looking at the spectrum of alcohol use and its implications have noted adverse associations between alcohol use and medication adherence [35], optimal health-care utilization [36] and risk behaviours for HIV acquisition [37,38]. For people living with HIV, the direct immunological effects of alcohol use are hypothesized to lead to a lower CD4+ T-cell count, particularly among those who report concurrent crack cocaine use [39]. The indirect effects are typically described in terms of the sequelae of alcohol use, such as cirrhosis/liver disease leading to inadequate plasma drug concentrations and ineffective drug therapy [40], immunoincompetence related to liver disease, and micronutrient deficiencies leading to accelerated HIV progression [41].
The findings of this study should be viewed in the context of its limitations. First, our sample was not randomly selected and thus cannot be generalized to HIV-positive people who use illicit drugs in the rest of Vancouver or elsewhere. However, we did employ community-based methods such as snowball sampling in an effort to minimize selection bias. Second, as this is an observational study it is possible that the observed relationships are under the influence of confounding variables that were unaccounted for. We have sought to address this bias with multivariate adjustment of the covariate estimates and the selection of a set of possible socio-demographic, behavioural, social and clinical confounders. Also, the substance use data presented here was generated through participant self-report and therefore, there is no way to verify the veracity of substance use. As such, it is possible that individuals under-reported their usage, thereby attenuating the effect seen.
In summary, we assessed the impact of high-intensity substance use on VL rebound among HIV-positive individuals who had achieved VL suppression. Daily use of injection heroin, crack cocaine smoking and heavy alcohol use were each found to be predictors of VL rebound in this population. Given the current focus on promoting access and adherence to ART, the multiple deleterious impacts of substance use on ART treatment outcomes mean more attention must be paid to support HIV-positive individuals with co-occurring substance use disorders to reach the United Nations’ 90-90-90 efforts to end the HIV pandemic.
Footnotes
M-JM's institution has received unstructured funding from NG Biomed, Ltd, a private firm seeking a government license to produce medical cannabis, to support him. JM has also received financial support from the International AIDS Society, United Nations AIDS Program, World Health Organization, National Institutes of Health Research-Office of AIDS Research, National Institute of Allergy & Infectious Diseases, The United States President's Emergency Plan for AIDS Relief (PEPfAR), UNICEF, the University of British Columbia, Simon Fraser University, Providence Health Care and Vancouver Coastal Health Authority. The remaining authors declare no competing interests.
Acknowledgements
The authors thank the study participants for their contributions to the research, as well as current and past researchers and staff.
The study is supported by the US National Institutes of Health (R01-DA021525). The funders had no role in the design and conduct of this study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript. This work was supported in part by a Tier 1 Canada Research Chair in Inner-City Medicine awarded to EW. M-JM is supported by a New Investigator award from the Canadian Institutes of Health Research, a Scholar Award from the Michael Smith Foundation for Health Research and the US National Institutes of Health (R01-DA021525.) JM is supported by the British Columbia Ministry of Health and through an Avant-Garde Award (No. 1DP1DA026182) from the National Institute of Drug Abuse (NIDA), at the US National Institutes of Health.