
Abstract
In this review, we consider recent advances in the discovery and development of antiviral agents for respiratory syncytial virus (RSV) infections. A background to the various manifestations of human RSV infection and current treatments is provided. The technical, clinical and commercial issues surrounding the development of such antiviral agents are discussed.
Introduction
The aim of this review is to provide a broad overview of the clinical problems associated with respiratory syncytial virus (RSV) infection in different patient populations and the options currently available for dealing with them. There are a number of recent reviews dealing with specialized aspects of this field to which the reader is referred [1,2]; our focus will be the current and future options for the use of antiviral drugs. We hope this approach will provide a rapid but thorough introduction to those new to the field.
Target patient populations
RSV is a ubiquitous infection of humans of all ages across the globe [3–5]. The manifestation of infection and the consequent requirement for therapeutic interventions is very different in the various populations at risk of infection with the virus. The fragmented nature of the potential market for antiviral therapies has been an impediment to investment by pharmaceutical companies in novel agents. The various patient groups are best considered by age and underlying medical conditions.
Healthy adults
We are constantly exposed to RSV infection throughout life. For a normal healthy adult, RSV infection does not require treatment [5]. Intervention would be required very early and at such a low cost that the development of either antiviral drugs or a vaccine is likely to be impractical. Prophylaxis of healthy adults to avoid viral spread during seasonal epidemics may be worthwhile, particularly for those employed in institutional environments, such as care homes, nurseries or educational establishments with vulnerable inmates.
Immune compromised adults
In adults who have undergone stem cell transplants or who have other forms of immune suppression RSV can present a lethal challenge. In the most extreme examples both morbidity and mortality can be very high [6]. In light of the potentially serious nature of such infections and the extensive treatment such patients have already received, the cost of both prophylaxis and therapy are supportable. Long acting, infrequently dosed therapies are ideal in such patients as their suppressed immune systems are likely to make vaccination problematic. Seasonal chemo-prophylaxis may be a successful strategy depending on the geography (RSV infections occur in epidemics during the winter months in both northern and southern hemispheres, but all year around in the tropical areas [7]). Improved methods for the rapid diagnosis of RSV infection will have a major impact on treatment modalities.
Adults with underlying respiratory disease
The epidemic of chronic obstructive pulmonary disease and the introduction of effective maintenance therapy for such patients have created a pool of adults whose lungs are compromised by the disease and can be further and severely damaged by RSV infection. This group of patients are generally exposed to RSV from family contacts and are suitable for prophylaxis with either small molecule or biological approaches. Again, a long-acting infrequently dosed therapy would be ideal. Such therapies need to be suitable for use in what is predominately an elderly population. Improved diagnostic methods are again likely to be critical given the low level of virus replication in this population.
Children
Most children have been exposed to RSV infection by the age of 24 months [8,9]. For children over 12 months in age, such infections are usually mild and of low morbidity. Virus replication is less extensive than in the younger cohorts, although a very small number of children may have more serious disease (for example, in native American children) [10]. The principle reason to treat these older children would be to lessen the impact of disease in a family setting where there are very tiny babies or older children or adults with underlying disease issues.
Babies and infants
This patient group suffers the most significant replication of RSV with associated pathology and is thus by far the most studied. Viral replication is extensive in the newborn respiratory tract and virus titres in nasal exudates reach extremely high levels and remain high for an extended period. RSV bronchiolitis is responsible for a huge influx of infants into neonatal and paediatric intensive care units during the winter months in both hemispheres [11,12]. The early detection (largely by symptoms), long duration of virus replication and severity of disease make this an ideal opportunity for therapy as well as prophylaxis.
Approaches to prophylaxis
The most common approach to prophylaxis of viral disease is the use of vaccines, RSV is unique in that passive immunization with polyclonal and monoclonal antibodies has been the more successful approach. In the future, the availability of a variety of new small molecules will enable alternatives to be offered to each of the therapeutic niches discussed in the preceding section.
Vaccines (not covered in detail in this review)
With the success enjoyed by vaccines to other para-myxoviruses like mumps and measles virus, it is perhaps surprising that progress on RSV vaccines has been very slow. This is for several reasons. First, the development of an inactivated virus vaccine in the 1960s led to more severe disease in vaccinated children [13]. Consequently there has been a great emphasis on the safety of any proposed vaccine. Second, RSV vaccines to protect newborn infants will require immunization of pregnant mothers - again requiring a high safety margin. Third, our immune response to natural RSV infection is very short-lived allowing annual infection and even multiple infections in a single season [14]. It will be a very severe challenge for any vaccine to improve on this situation. Last, with live attenuated vaccines it has proved difficult to get the right balance between virus replication and a lack of symptoms [15].
Current research on vaccines is aimed at using other viruses as vectors for RSV antigen delivery [16]. The most advanced of these approaches is in Phase II clinical trials. Earlier programmes to develop subunit vaccines for RSV appear to have been abandoned [16]. For recent, detailed reviews of RSV vaccines please see articles by Habibi et al. [17] and Groothuis et al. [16,18].
Antibodies
The advent of monoclonal antibodies brought optimism that virus infection could be prevented with cheap and easily produced antibodies. In most cases, such optimism was short-lived as it proved difficult to find antibodies that produced effective results at reasonable cost. The unique situation of RSV infection in premature infants lent itself to prophylactic antibody development for a number of reasons. First, it had already been shown that polyclonal antibodies could protect against RSV infections in animal models and in clinical trials in infants [19]. Second, the amount of antibody required to protect a small infant could be manufactured at a reasonable cost [19]. Third, there was a large susceptible population of premature infants who were readily identifiable as candidates for the antibody [20]. Last, the predictable season-ality of the virus infection [7] lent itself to prevention by dosing through half a year rather than a longer period.
Paluvizimab (Synagis®) is a monoclonal antibody developed by MedImmune, Inc. (now a subsidiary of Astra-Zeneca). For a full discussion of its development see the review by Pollack and Groothuis [21]). Initially the antibody was identified as having moderate neutralizing antibody activity against RSV through binding to the F protein [22]. The antibody was shown to have suitable characteristics for development as a prophylactic, namely a long half-life in vivo, a good preclinical safety profile, a suitable manufacturing route and adequate potency [21].
Clinical trials demonstrated that the antibody could prevent RSV infection in about 50% of those infants receiving a full course covering 6 months of the relevant winter season [23]. A further clinical trial in children with congenital heart defects showed a similar benefit [24].
A major problem with using such sophisticated biological molecules in prevention is cost. This has prevented uptake of the antibody in some countries for premature infants and in most countries for full-term infants where the cost-benefit ratio is not so obviously in favour of the antibody (for a debate on this issue see Stewart [25]).
MedImmune, Inc. was recently refused a marketing authorization requests for a new antibody (Motavizumab), which has been engineered to improve on the potency of Paluvizimab by in vitro evolution methods [26]. The antibody was found to cause a small but significant increase in inflammatory side effects in comparison to Paluvizimab and, because the clinical trials had been designed to show only equivalence with its forerunner, there was no reason for regulators to accept this risk [27].
This development failure will significantly hinder the replacement of Paluvizimab with better antibodies. It will require investors or companies with courage to undertake the very large clinical trials required to show significant improvement over Paluvizimab in potency and no increase in inflammatory side effects, which occur at low frequency. Astra-Zeneca recently announced that it was stopping the development of Motavizumab.
The failure of the Astra-Zeneca molecule will increase the incentives to the developers of generic copies of Paluvizimab, but the regulatory hurdles faced by such molecules are somewhat unclear. Various other anti-RSV antibodies are reported to be in development including those from Merus, Trellis and Symphogen.
Small molecules
For some of the patient groups, which are targets for RSV prophylaxis, small molecules may be even more attractive than antibodies on the grounds of cost and oral dosing (as opposed to painful injections). Such small molecules will need to be potent, have pharmacokinetic properties consistent with at most once a day dosing and be compatible with other medicines these patients are likely to encounter.
Although no currently licensed medication is suitable for such use, there are molecules in mid-stage development that have suitable properties. The patient groups that may be appropriate targets for small molecule prophylaxis are the recipients of stem cell transplants, elderly adults with chronic obstructive pulmonary disease and residents of nursing homes.
Approaches to treatment
Antibodies
The sole use of antibodies to date has been to prevent RSV infection in small infants. Studies are underway to determine if antibodies have a role in the treatment of ongoing RSV infection. At first glance it might be thought that antibodies would be unlikely to have an effect on RSV once infection is well-established. Access to the infected cell by a large antibody molecule would not be possible. If an extracellular stage, however, is involved in the transition of RSV infection from the upper to the lower respiratory tract then an antibody may be able to prevent this transition. Thus diagnosis during the earliest stages of disease would allow the initiation of treatment and prevention of a lower respiratory tract infection.
A current clinical trial, based on an earlier small Phase II study, is examining the effect of Motavizumab on treatment of older children with RSV infection. If this trial was successful it might influence future studies in this and other patient groups.
Small molecules
Entry, including fusion, inhibitors
Inhibition of viral cell entry is a well-established antiviral approach. In the case of RSV, a limited number of small molecule chemotypes have been identified but there is little evidence of any progressing beyond clinical Phase I.
The most established work in the field has been carried out by the Bristol-Myers Squibb group. Building on the benzimidazole template a series of highly potent compounds have been identified, culminating in BMS-433771 (Figure 1). No new information about the clinical development of this compound has been released although it is assumed to have been halted. The early published work has been reviewed in our previous publication [28], but recent results have expanded the structure-activity relationship (SAR). In one publication, Yu et al. [29] illustrate how replacement of the benzimi-dazolone with aza-benzimidazolones (particularly 6-aza substitution as found in BMS-433771) reduces the electron density and increases the polarity of this ring system, having a beneficial effect on susceptibility to metabolism. Combination with a cyclopropyl substituent provides the best combination of antiviral activity, metabolic stability and membrane permeability (BMS-433771; Figure 1) to allow evaluation in the BALB/c mouse model. The compound demonstrated activity at 50 mg/kg daily dosing. The work was extended to cover substitution of the benzimidazole ring system [30]. C5-aminomethyl substitution yielded examples (Compound
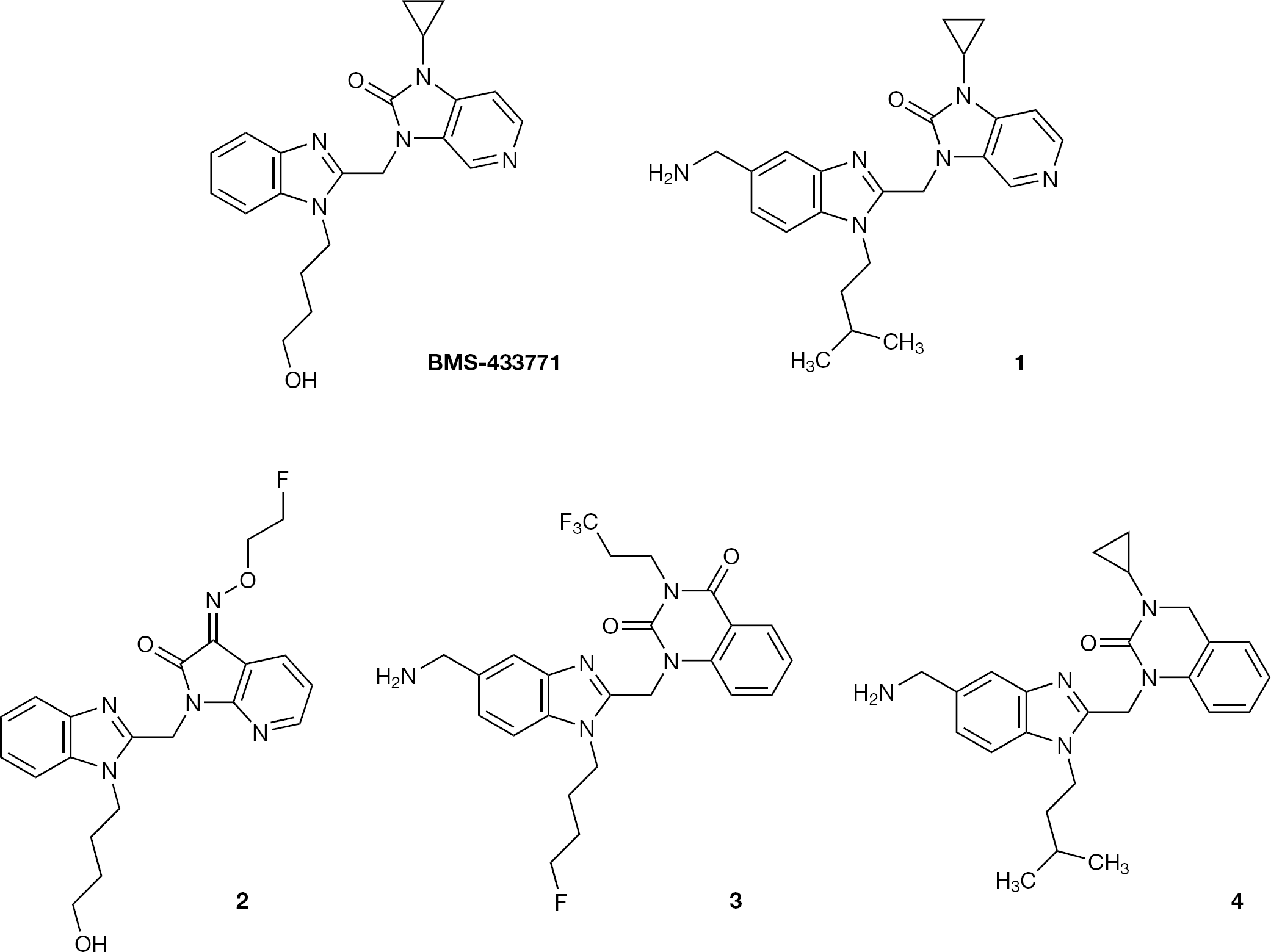
Progression of the Bristol-Myers Squibb benzimidazole series
A related set of compounds from AstraZeneca are the subject of a patent application [33] although limited data is presented. In this case the patent focuses on 6,6 quinazolinones and the most potent compounds are sub-nanomolar in antiviral activity and extensive crystal form data is presented for one particular analogue (Compound 4; Figure 1). The status of this programme has not been disclosed.
A recent publication from Tibotec (Bonfanti et al. [34]) described the evolution of another series of benzimidazole compounds. Starting with JNJ-2408068 (Figure 2), which was identified to have extended tissue retention time, the amino piperidine moiety was modified to the morpholinopropyl substituent and a 10-fold improvement in tissue half-life was achieved. Antiviral potency was returned to the template by combining this modification with C4 substitution to yield TMC353121 (Figure 2). The compound had good activity against a range of RSV strains (50% effective concentrations [EC50] 500 nM-30 pM) and a plasma half life between 4 and 24 h but still possessed a large volume of distribution (79 l) and poor oral availability. When dosed at 10 mg/kg in the cotton rat model it showed 0.4 log reduction of virus load orally and 1.2 log reduction via the intravenous route.
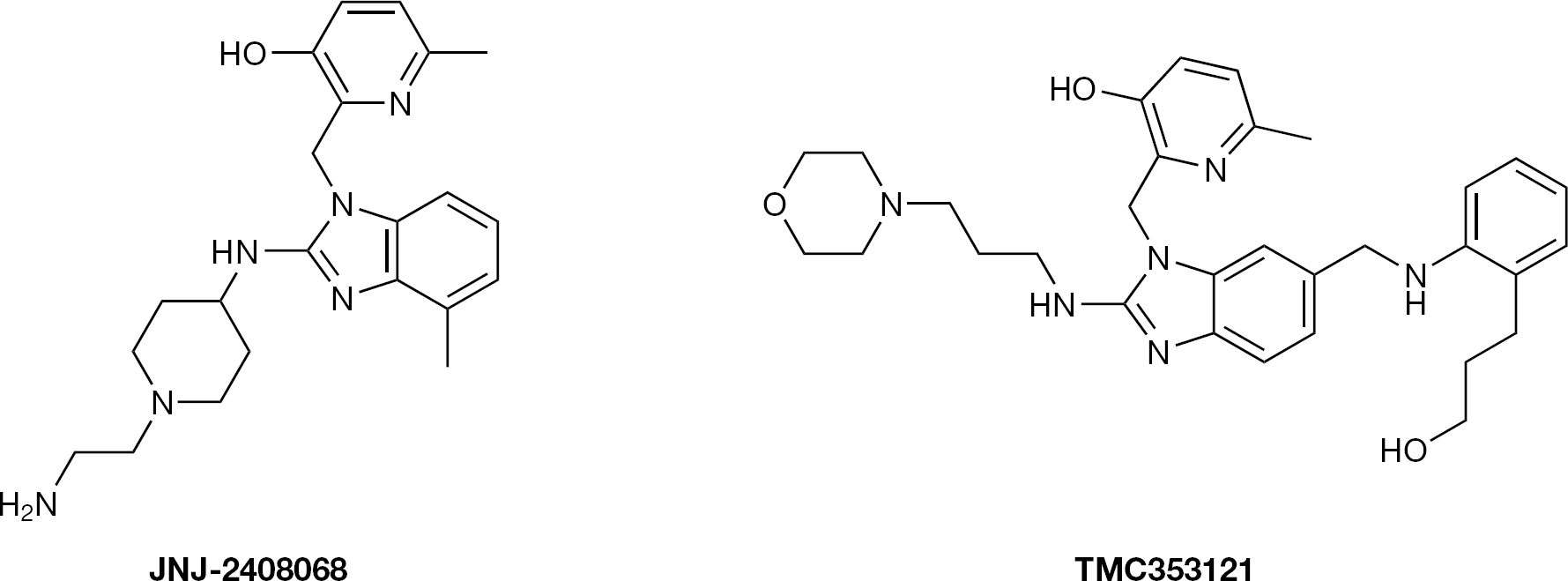
Progression of the Johnson & Johnson series
TMC353121 has been successfully crystallized with a truncated construct of the RSV F-protein [35]. It was shown to induce a distorted form of the fusion protein trimer with TMC353121 sandwiched between the heptad repeats. It is speculated that the compound serves to prevent the natural closure of the heptad repeats during the fusion process by stabilizing an unnatural and non-productive conformation of the F-protein. The compound is currently under early clinical investigation by Johnson & Johnson and its exact status is unknown.
Pharmacokinetic-pharmacodynamic data in the cotton rat model of viral infection has been published for TMC353121 [36]. The compound, when dosed either via the subcutaneous or intranasal routes, reduced viral titres in a dose-dependant manner. Using model data, the maximum viral load reduction was predicted to be 1.5 log at 200 ng/ml, although the authors comment that the relationship between the plasma drug levels required to achieve significant antiviral activity in the cotton rat and in different clinical situations still needs to be evaluated (see Future avenues of RSV research).
No new publications from the Biota group have emerged, although the joint development programme for BTA-9881 with AstraZeneca was terminated in 2009.
In a recent publication Lundin et al. [37] report the screening of the ChemBioNet diversity collection (16,671 compounds) in a whole-virus assay. Two compounds with good antiviral potency were identified (compound
Screening hits from the Chem BioNet diversity collection
Recently MicroDose Therapeutx disclosed reformulation work on MDT-637 (formerly VP 14637; Figure 4). Its clinical development as an aerosol was previously stopped due to excessive organic solvent content (etha-nol/propylene glycol) and has now been re-formulated as a dry powder for aerosol inhalation, using the MicroDose inhaler. Delivery of the compound to both the upper and lower respiratory tracts via this technology was successfully demonstrated during a few seconds of simulated infant passive breathing [39]. Gilead and MicroDose Therapeutx announced their collaboration on this programme and are planning to initiate clinical Phase I before the end of 2011.
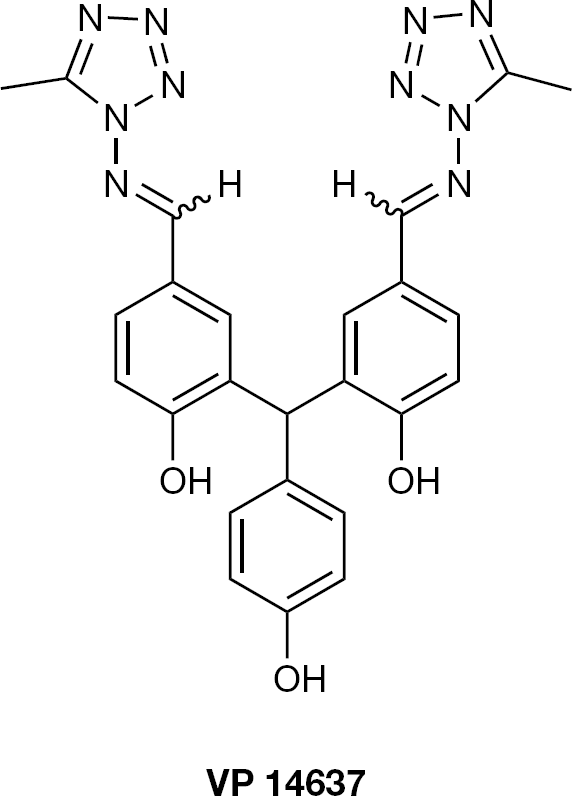
MDT-637, formerly VP14637
A collection of publications relating to the use of peptides as inhibitors of RSV fusion has appeared over the past 4 years [40–44]. Perhaps the most interesting is the report by Harrison et al. [45] that relates to the discovery of short, water-stable α-helices as potential anti-infectives. Mimicking F483-V495 of the RSV fusion protein heptad repeat, a short 12-residue peptide was synthesized with two 5-residue lactams via K-D linkages. The resultant peptide was shown to have much α-helical content by CD and NMR and was stable in water and plasma. When assessed in an RSV F-protein induced cell-cell fusion assay, it had picomolar activity (IC50 ∼120 pM). No antiviral activity was presented.
Sulfated sialyl lipids have demonstrated antiviral activity against several DNA and RNA viruses including RSV. The best characterized of these compounds, NMSO3, has submicromolar potency in plaque reduction assay [46]. Mutant viruses in the presence of the drug were isolated to help clarify the mode of action of the compound. Sequence analysis of the F and G coding regions of the generated variants narrowed the resistance to the conserved region of the G protein [47], yet a direct interaction with the target has not been reported.
Replication inhibitors
The RSV genome is encapsidated by the nucleocapsid (N) protein, which forms a helical structure and protects the RNA from ribonucleases. The N-protein is highly conserved within RSV strains and is associated with the viral polymerase (L), M2–1 and the phospho-protein (P), forming the transcriptase complex that is essential for viral replication. Compounds that bind to or are able to interfere with the formation of this complex are therefore likely to inhibit viral growth.
There is no easy biochemical screening approach that targets this complex. Cell-based assays have been until now the best option available. Recently, however, a new replicon system [48] has been optimized and has the potential to be of great use in finding and validating RSV inhibitors.
Replication inhibitors: N-protein interacting compounds
A series of 1,4-benzodiazepine derivatives were described [49] by Arrow Therapeutics, which inhibit viral replication and have been shown to give rise to mutations in the N-protein. Initial library screening in a full virus assay led to the identification of the acetamide (compound
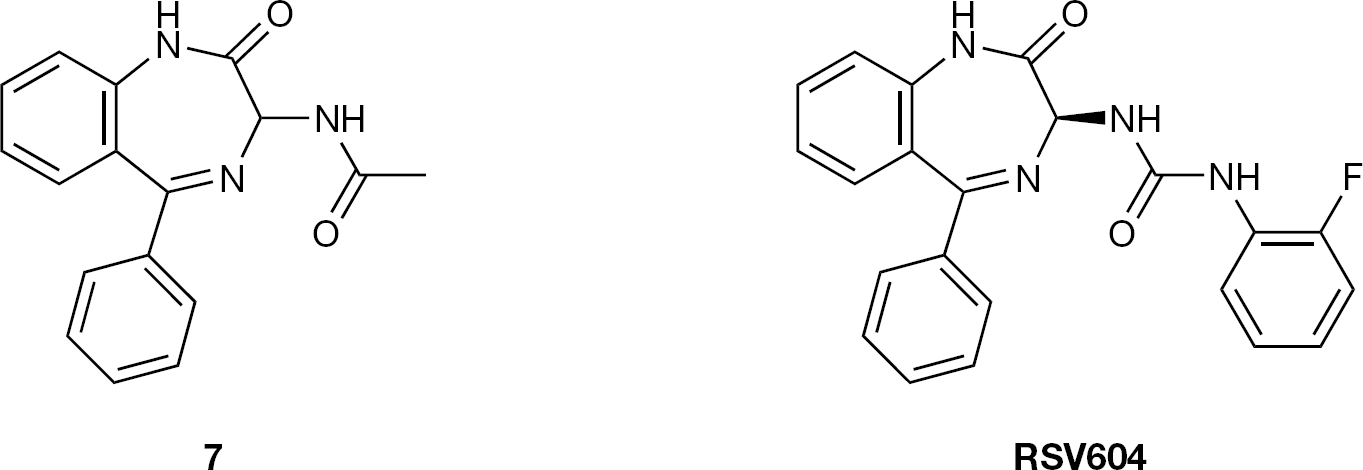
Progression of the Arrow Therapeutic replication inhibitor series
Generation of mutant viruses, using excess compound during viral replication, produced isolates that were 40-fold less sensitive to RSV604 compared with wild-type virus. The amino acid changes in the viral genome isolate showed three non-conserved mutations (K107N, I129L and L139I), all in the N-gene of the mutant virus. The generation, by reverse mutagenesis, of the individual changes using the wild-type virus background recapitulated the lower sensitivity to the drug of the reverse mutants carrying L139I alone or I129L and L139I [50].
A more physiological in vitro approach, mimicking the epithelial infection observed in the lung, was used to evaluate the potency of this molecule. The compound was dosed to an epithelial airway culture system [51]. It was potent against RSV spread as demonstrated when dosed to the medium surrounding the basolateral region of the pseudostratified epithelium. This was true for compound dosed before, at the same time or after the virus was inoculated onto the apical, ciliated surface.
The physico-chemical characteristics of RSV604 were favourable for its clinical testing [52]. During Phase I trials, RSV604 was well-tolerated in all dosing regimens and no serious adverse events were reported. Plasma concentrations of RSV604 above the in vitro IC90 values were achieved. Subjects given a loading dose of 600 mg RSV604 followed by 6 days at 450 mg exhibited trough concentrations above the in vitro IC90 at the end of day 1 and were ≥4×IC50 and ≥2×IC90 for the following 6 days. RSV604 was licensed to Novartis in 2006. To date, no further clinical or research data has been released to the public domain.
Crystallization of known targets, particularly in the presence of inhibitors, is a well-established route for potency optimization of lead molecules. Until recently, the structure of the N-protein had proved elusive but was recently resolved [53]. The N-protein crystallizes in a decameric ribonucleoprotein ring complex and Tawar et al. [53] postulate that the RNA molecule wraps around the protein ring. In this pattern, each protein subunit spans seven nucleotides in alternative rows of four and three such that they are exposed and buried, respectively. The availability of such detailed structural information may aid the identification of new drug target sites on the N-protein.
Replication inhibitors: Ribavirin analogues
Ribavirin is a nucleoside analogue that was characterized as a broad-spectrum antiviral more than 30 years ago [54] yet its mechanism of action still remains a source of debate. Ribavirin has been described as an inhibitor of the polymerase of a number of viruses. Its 5′ triphosphate has been shown to block GTP-dependent viral messenger RNA capping via the inhibition of the guanyl transferase and the monophosphate has been shown to inhibit ino-sine monophosphate dehydrogenase (IMPDH) [55]. The compound is potentially teratogenic and of limited efficacy, characteristics that severely limit its use in infant RSV infection [56]
Although several efforts to find ribavirin analogues have been undertaken, there has been very little success progressing similar drugs through clinical evaluation against other viruses, including RSV. Perhaps the greatest advance has been achieved with viramidine, an ammoniated prodrug of ribavirin that is still in clinical trials [57].
Replication inhibitors: PPAR-γ
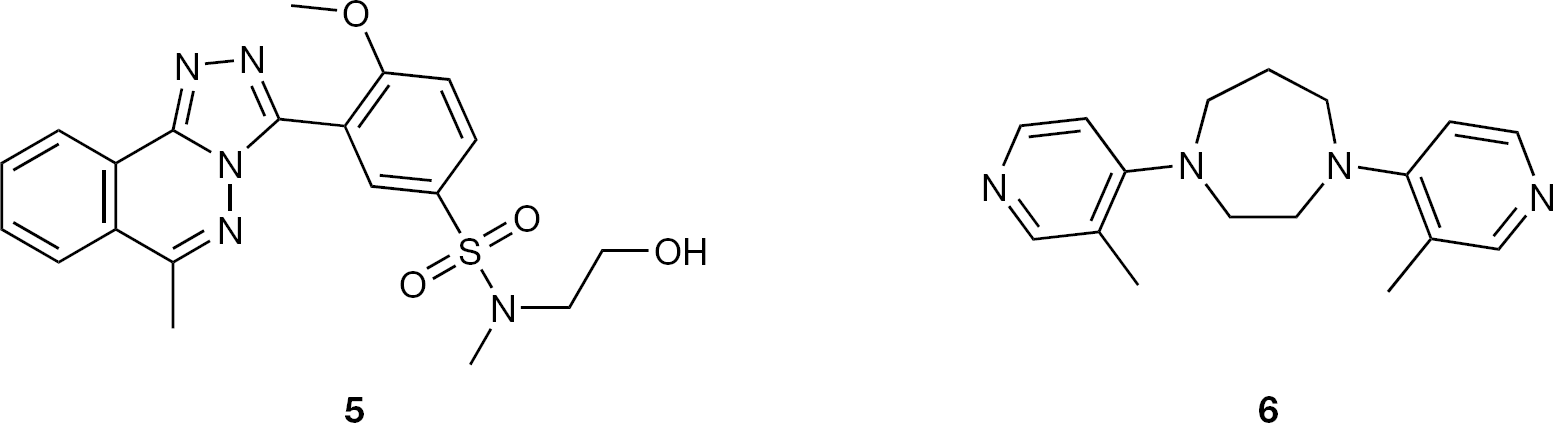
New compounds, previously described as acting through the peroxisome proliferator-activated receptor gamma (PPAR-γ), have been tested against RSV in vitro and shown to block syncytia formation in A549 and HEp-2 cells during RSV infection [58] (Figure 6). The antiviral effect of this compound class has been reported for other viruses. This suggests a more general viral mechanism in which some viruses exploit these ligand-activated transcription factors for their own benefit [59]. The antiviral effects were observed when the drugs were added prior to or following RSV infection. Further work is needed to progress these active structures into the clinic but the fact that PPAR-γ agonists possess anti-inflammatory capacity opens the possibility of a further beneficial effect from this approach during the course of RSV infection.
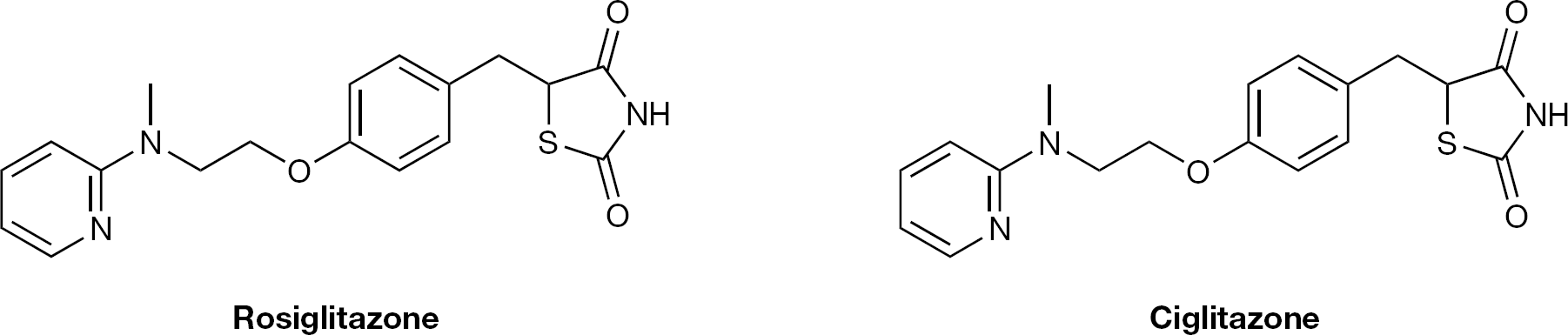
PPAR-γ inhibitors with antiviral activity
Replication inhibitors: Benzazepine inhibitors
Yamanouchi patents and publications have described a series of benzazepine thiophenes with submicromolar activity in plaque-reduction assays against RSV [60]. One of the most potent compounds, YM53403 (Figure 7), had an EC50 of 200 nM with a selectivity index of over 400.
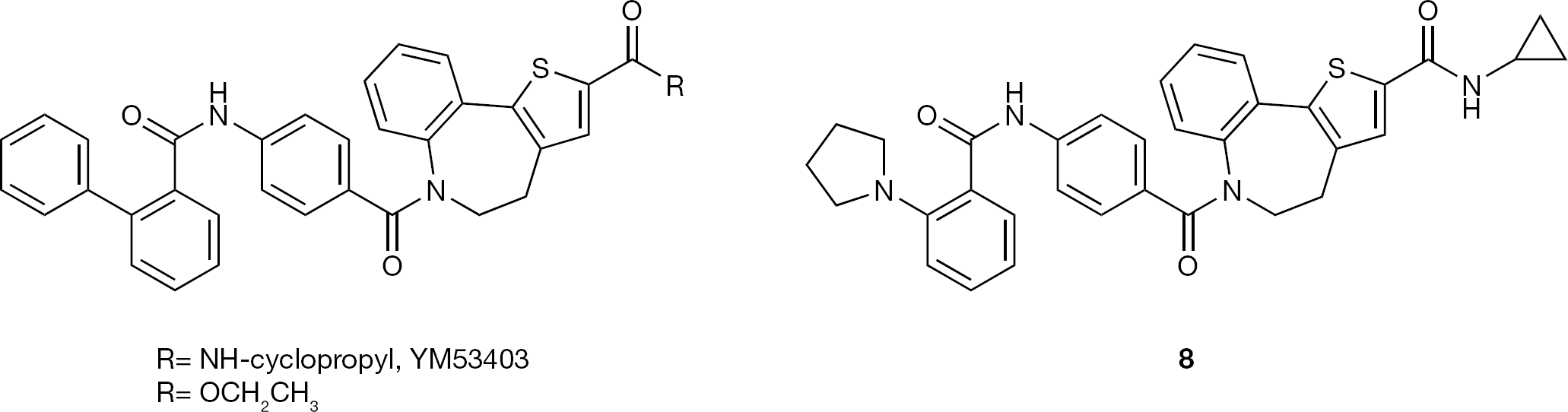
Benzazepine inhibitors of viral replication
Further mechanism of action data was described for YM53403. Time-of-addition studies indicated that activity was observed up to 8 h post-infection and was very similar to ribavirin. Mutant generation and sequencing identified a single change in the L (polymerase) gene, Y361H, suggesting that the mode of action of the drug was through the polymerase. More recently, related compounds have been the subject of a patent application from Gilead [61] exemplified by compound
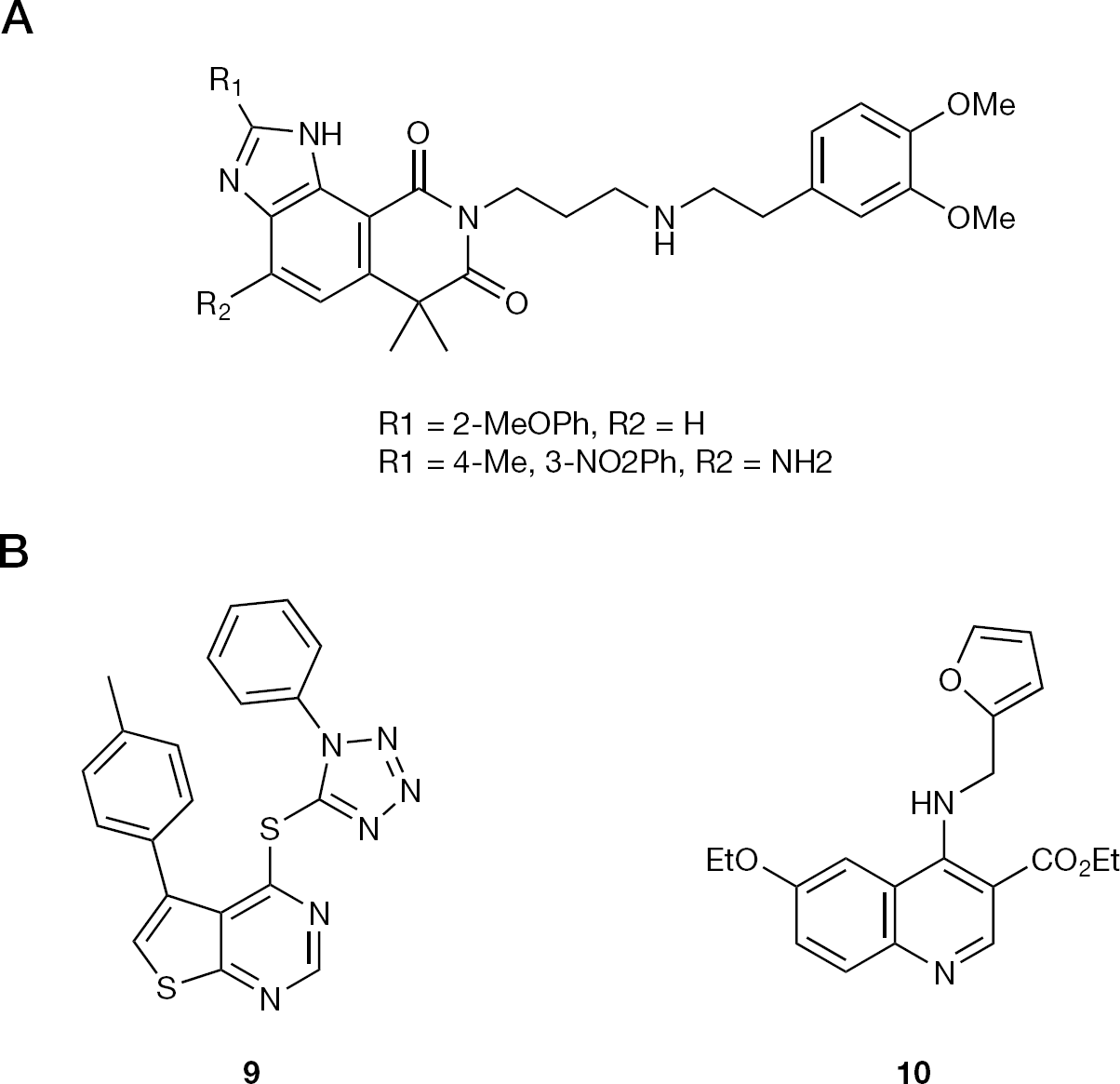
Replication inhibitors: Quinazoline-dione inhibitors
A lead optimization programme of these potential RNA synthesis inhibitors (Figure 8A) was reported [62] (see also [63]).
Potential replication inhibitors
Replication inhibitors: Transcription and regulation inhibitors
Olivo and co-workers [64] used a minigenome screening approach to screen for RSV replication inhibitors, although compounds of only moderate activity were identified. Thienopyrimidine (compound 9; Figure 8B) had an EC50<25 μM and quinoline (compound 10; Figure 8B) an EC50 of 1.46 μM. No further work has been reported.
Antisense agents such as peptide-conjugated phos-phorodiamidate morpholino oligomers can interfere with viral protein expression. One such molecule, AUG-2, targeting the L protein has demonstrated anti-RSV activity [65]
Host-virus interactions
Recent efforts on RSV drug discovery from Bonavia et al. [66] have been published. The anti-RSV activity of general, broad-spectrum compounds was extensively assessed. Compounds 11 and 12 (Figure 9) possessed namomolar activity against RSV and time-of-addition studies determined these compounds to be acting at a point post-viral entry and probably at the point of virus replication. Wider antiviral activity against Paramyxoviridae, Orthomyxoviridae, Flaviviridae and Retroviridae suggested the target might be cellular rather viral. Affinity capture experiments indicated compound 11 binds strongly to dihydroorotate dehydrogenase (DHODH) and compound 12 binds to the trifunctional complex CAD (carbamoyl-phosphate synthetase 2, aspartate trans-carbamylase and dihydroorotase). As expected these compounds were toxic to certain cell types.
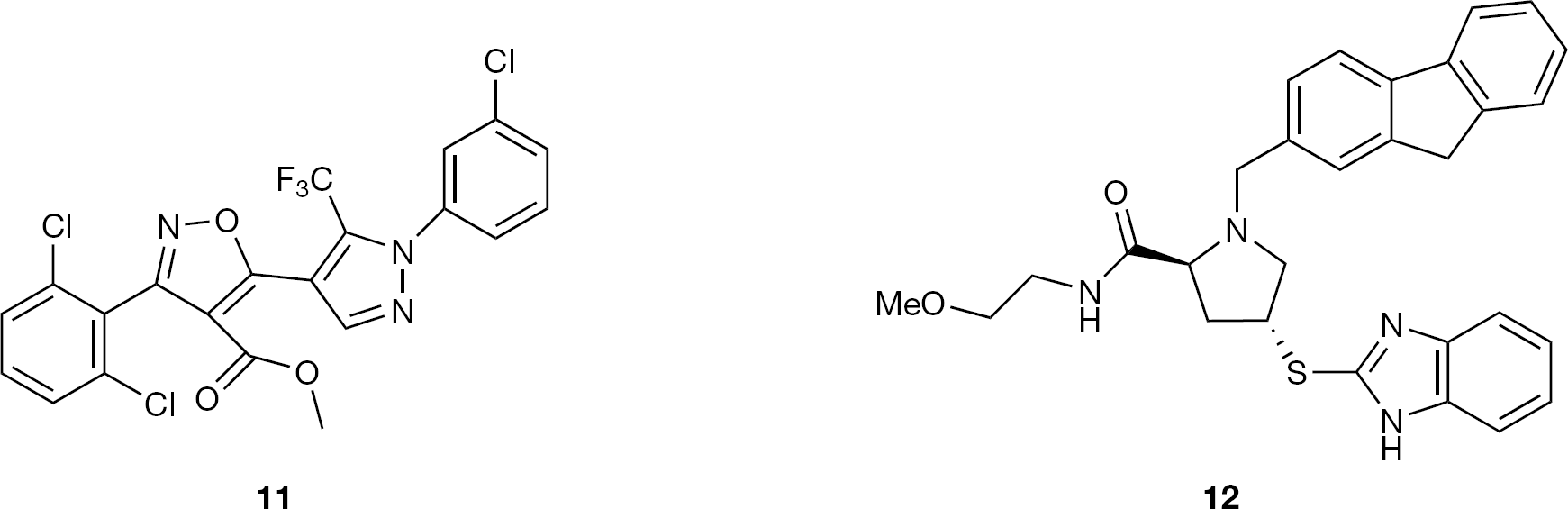
Broad-spectrum compounds targeting host-virus interactions
Efforts were made to test these compounds in a cotton rat model, but readouts were confounded by in vivo toxicity attributed to the compounds mechanisms of action.
Other mechanisms of action
In a previous review, a wide variety of compounds identified as inhibitors of RSV (up until 2006) were discussed. The reader is referred to this comprehensive list [28].
siRNA
RNA interference (RNAi) using synthetic small interfering RNAs (siRNAs) is a powerful way to suppress gene expression in vitro and has been widely used for gene function studies. The possibility of using RNAi as a therapeutic modality has been explored in a number of in vivo models of disease [67]. siRNA delivery and administration is a major stumbling block for such therapy. The assessment of siRNA as antiviral therapy by direct administration into the lungs using a nebulizer is thus very attractive as a general proof of concept for siRNA. The murine model of RSV has been used by Bitko et al. [68] and Alvarez et al. [69] to show effects of siRNA therapy on viral load. This is surprising given the very limited replication of RSV in this model [70], but gave confidence to these investigators to take the potential therapy into the clinic.
Direct delivery of siRNA into the lungs allows a very localized effect and limits systemic spread [67,71]. ALN-01 was first given by intranasal administration to healthy volunteers 2 days before and 3 days after inoculation with a clinical isolate of the virus. The data showed a 38% reduction in the RSV infection, which occurred in the siRNA-treated groups. Unfortunately the control group used phosphate-buffered saline (PBS) as a placebo rather than the better control of a mismatched siRNA. Since ALN-01 was safe and well-tolerated in the study, it would be justified to use a control RNA to judge if the effect is due to a direct or indirect antiviral effect.
Further studies of ALN-01 have been done in patients who have undergone lung transplants [71]. In this heroic study, 521 transplant recipients were screened over 1 year for RSV infection. A total of 46 were found and 24 patients were studied. Of the 24 patients, 16 were given the siRNA and 8 placebo (PBS). Unfortunately, analysis showed that the placebo patients had a significantly higher viral load at the start of the study confounding analysis of antiviral effects. Not surprisingly, there was less symptomatology in the treated group than the placebo recipients.
A major limitation in antiviral therapy is the emergence of viral escape mutants that are no longer targeted by a given drug. In the case of siRNA therapeutics, escape mutants can hamper the recognition of the target sequence by the RISC. Mutations were found within the siRNA target sequence or in its vicinity, thus causing a conformational change of the RNA target structure. To overcome this problem, new combinatorial approaches have been developed in which multiple siRNAs targeting different viral genes are applied simultaneously (for a review see [72]). Such approaches will complicate the clinical development of siRNA as they will require the simultaneous development of multiple RNAs with the ensuing regulatory complications.
Future avenues of RSV research
By far the biggest issue facing the development of any new RSV medication is the design of clinical trials to demonstrate their effectiveness. The diversity of the RSV-infected patient population, their age spectrum and their prognoses all make evaluation of compounds in the clinic more difficult. Such a complex clinical trial scenario has prevented the progression of compounds into large Phase III trials in this risk-averse era of drug development.
The lack of good animal models in which to show ‘proof of concept’ for treatment of RSV disease is to some extent mitigated by the development of human challenge models. In such experiments volunteers (usually male and of college age) are infected intranasally with a challenge dose of the virus [73,74]. Such an insult results in an upper respiratory tract infection in a proportion of those infected. This type of infection is short-lived and produces relatively mild symptoms [56]. Whilst this mild symptomatology is important so that the experiments are ethically acceptable it does mean that the model is not equivalent to a natural viral infection in any significant patient group. The model used intelligently can be very useful to aid the development of a new RSV medicine or vaccine but trials in the real disease are essential to judge the effectiveness of any intervention.
Once a new drug has passed all the preclinical hurdles and is judged safe for further evaluation then it can be used in challenge trials. As the challenge is a high dose and produces a wave of virus replication over 3–5 days then it is sensible to use the model where the antiviral agent is given shortly before the infection. Given after challenge, compounds would have very little chance to inhibit replication before it is over. Compounds showing a strong antiviral effect in the model should then move on to a trial in real disease.
Two groups of patients present the best opportunities to judge the effectiveness of new RSV drugs. The adult immune compromised patient (usually stem cell transplant patients) is a group where successful trials have been run [71,75]. These trials are difficult because of the relatively small number of transplants done and the wide geographic distribution of transplant centres. By contrast, the patients are in need of therapy and the transplant community are keen to join such studies. The studies done to date have shown some encouraging effects on the outcome of infection, but require further work in larger studies [76].
The very best patient group from an experimental point of view are the very young. In babies from 0 to 6 months of age viral replication is extensive and extended in duration, resulting in an excellent opportunity to intervene [77]. The extremely young age of the patients is the problem. Companies have been reluctant to commit to the extensive preclinical work required to test a drug in such a vulnerable population.
RSV clinical work is subject to a catch 22 where the new agents require testing in a group where there are very large numbers but that are, for ethical reasons, difficult to reach. Despite these challenges a potent safe, RSV inhibitor is certain to win a commercially significant market if companies have the courage to finish development programmes.
Footnotes
KP, RA and PN are former employees of Arrow Therapeutics, a wholly owned subsidiary of AstraZeneca. The authors declare no current competing interests.