
Abstract
Peritoneal dialysis (PD) was introduced in China later than in most Western countries, and PD research activity was quite limited until the 1990s. However, in the 2000s, and even more so during the last decade, there has been an unsurpassed increase in the number of PD patients, paralleled by a substantial increase in PD research activity reflected by an increasing number of PD papers from China. In this brief review, we describe some of the factors that may explain the dramatic developments in PD research in mainland China, such as the focus on basic research using scientific approaches that subsequently could be applied also in clinical studies. Another important factor was the growing interactions with international PD research centers in Hong Kong and in Western countries. Thanks to strong support from Chinese national and regional funding sources, a growing number of young Chinese researchers went to key international PD centers to learn about novel advanced research techniques. This paved the way for long-lasting, productive collaborations with benefits also for the foreign host institutions. Finally, we present some current research projects, including basic research that may contribute to the understanding of mechanisms behind complications such as peritonitis, and clinical projects aiming at improving PD management guidelines and better understanding of the potential of PD in China. Because of the size of the PD population, now the largest in the world, and the increasing number, and quality, of researchers in the PD field, PD research in China is destined to be a major contributor to advancements in PD in the near future.
Keywords
Growth of Chinese pd Research Internationally and Locally
Peritoneal dialysis therapy in China started to grow more rapidly in the mid-2000s due to the growing accumulated experience of the therapy and expanded insurance coverage (14), which was crucial. In addition, the Chinese Society of Nephrology started to advocate the use of PD. More detailed reasons behind the growth of PD in China are discussed in a separate section (below). University hospitals that already had a PD research background showed the fastest growth in their PD programs and reported outstanding clinical outcomes compared with less experienced centers (15–19). In papers published during this time, it is evident that growing international collaboration (20–24) between China and Western countries played an important role, partially due to the increase of overseas training programs for young PD specialists that provided Chinese researchers a unique opportunity to publish in higher-impact international scientific journals such as Peritoneal Dialysis International. Since then, Chinese PD research has gradually started to contribute to international nephrology societies. Over the course of the last decade, more clinical experience on PD has been shared (Figure 1a), including patient education, center management practices, and clinical strategies (such as 3 vs 4 exchanges, the “satellite PD center” model, etc.) aimed at improving clinical outcomes (16,25–32). It is worth noting that clinical outcomes from some PD centers are comparable with or even superior to their Western counterparts (15,16,18,19,22). This raises interesting questions about whether there are factors involved, such as patient and center management practices, Asian culture itself, patient compliance, or even genetics, that may explain these positive results.
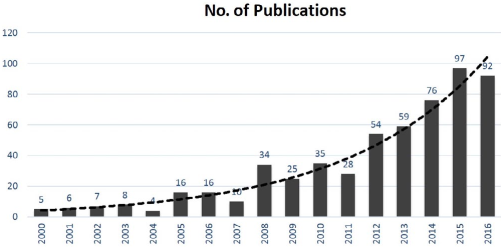
Increasing number of PD publications from China, data searched via PubMed (Chinese journals and papers from Hong Kong were excluded). PD = peritoneal dialysis.
While top PD centers in China were showing excellent outcomes (15,16,18,19,22) in the late 2000s, a large number of newer and often smaller centers started to use PD, sharing their single-center experiences in local journals. The number of local publications has increased to parallel the number published in international journals (Figure 1b). Compared with the years 2006 to 2010, the number of local PD publications increased remarkably during 2011 to 2015 (Figure 2). Common PD complications such as infections, including peritonitis, and cardiovascular disease (CVD) events, as well as problems related to quality of life and malnutrition, are among the top of the list, indicating the challenges facing clinicians. In terms of the difficulties pertaining to dialysis patient management, PD nurses have shared their clinical experiences in papers— accounting for 20% of all papers—written either by themselves or often with PD physicians. Apart from topics mentioned above such as care of PD-related infections and non-infection complications, topics often focused on patient education and PD center management. Compared with the limited resources in the early stages of PD in China, a considerable number of studies (7%) were sponsored by research funding from national or provincial governments and institutes, including universities or talent programs from 2011 to 2015. Obviously, the increased—and from an international perspective, uniquely expanded—investment in research and overseas training of researchers paved the way for the rapid growth of PD research in China (33).
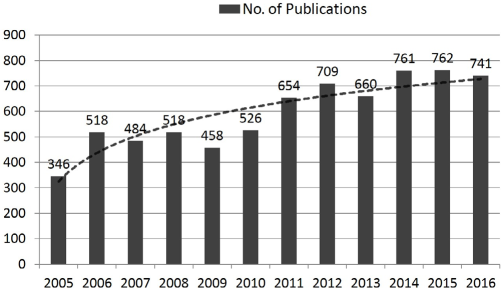
Increasing number of PD publications from Chinese journals, data searched via China National Knowledge Infrastructure (CNKI, www.cnki.net/). PD = peritoneal dialysis.
Meanwhile, in order to prolong patients’ treatment time on PD, many research projects focused on the mechanisms of peritoneal fibrosis and explored potential effective ways to protect the peritoneum from dysfunction due to fibrosis. For a long time, basic research was considered more prestigious, probably influenced also by similar priorities in the US, and was often promoted at the expense of clinical research in China to help young researchers have a successful scientific career. In the past decade, a large number of important basic experimental studies, targeting major changes to the peritoneum, from transforming growth factor (TGF)/Smad signal pathway, NF-κB, and Rho-kinase, to recent reports on serum response factor (SRF), peritoneal fibrosis, and angiogenesis, were reported by Chinese researchers (34 35 36 37-38). Several treatments, including SRF inhibitor (36), proliferator-activated receptor (PPAR)-γ agonist (21,35), suramin (39), recombinant human endostatin (40), and Smad 7 gene transfer (37), targeting fibrosis and other peritoneal membrane alterations, were proposed and tested by Chinese investigators. The results have been presented in high-impact international journals during the last decade.
Potential Reasons for pd Research Boom
With the largest population in the world, China has many long-term unsolved problems due to limited medical resources. For example, patients complain both about the difficulty of reaching out to doctors and about the high costs they have to pay for diagnosis and treatment. This has triggered intensive efforts by the government to find more cost-effective treatments for chronic diseases such as ESRD. It encourages researchers to explore the link between patient characteristics and clinical outcome among patients from remote areas (41,42), as this could provide evidence of the most effective way of using PD in developing areas. To reduce the need for patients to visit hospitals in large cities, the government encourages local hospitals in lower-tier cities and towns to provide treatment locally instead. Thus, many new startup PD programs began to learn and practice PD, contributing to the large number of PD papers in Chinese journals (Figure 1b, Figure 2). Most of these papers describe and analyze various aspects of the reality and daily challenges of the therapy and the efforts required to manage critical patients.
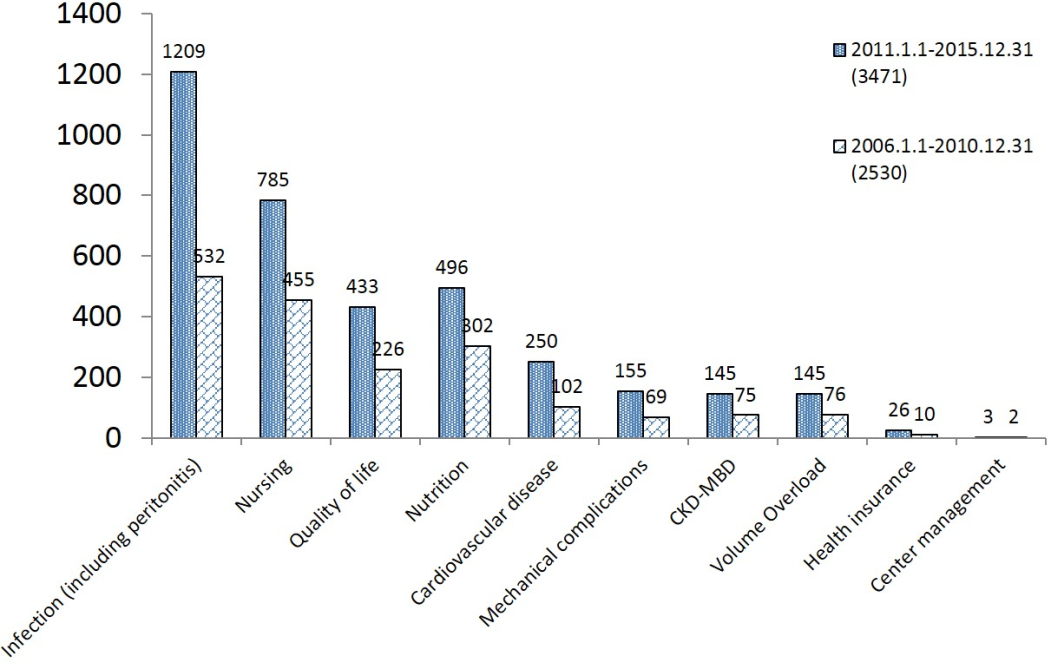
Top topics for PD research from Chinese journals in 2006–2010 and 2011–2015, data searched via CNKI. We searched each research area listed in the figure by related key words, such as “infection,” etc., together with “peritoneal dialysis,” via CNKI. We found a total of 1,209 papers published from January 1, 2011 to December 31, 2015, and 532 papers published from January 1, 2006, to December 31, 2010, under the classification of “Infection”. The “Infection” topics include “PD-related peritonitis,” “exit-site and tunnel infection,” etc. “Nursing” includes any topic related to patient management, such as complications, education and training, home visits, etc., and are mainly written by nurses. “Mechanical complications” refers to catheter problems such as catheter migration, catheter wrap and leakage, etc. “Health insurance” refers to economic evaluation, reimbursement system, or policy, etc., on PD therapy. CKD-MBD = chronic kidney disease-mineral and bone disorder; CNKI = China National Knowledge Infrastructure; PD = peritoneal dialysis.
Importantly, the concept of management of chronic diseases such as ESRD (43,44) was established and gradually spread and was accepted among the nephrology community during the last 10 to 15 years. This has provided a good platform for establishing follow-up systems for home therapy patients. Patients received better care thanks to these programs and their compliance with PD prescriptions, and regular follow-up, including lab tests, improved significantly. A more transparent process for clinical research in line with internationally established rules was also implemented, such as the need for patients to sign Patient Information and Consent Forms and to submit study protocols to an ethical review board for approval. Measures like these have in turn increased patients’ willingness to join research projects and thereby contribute to studies aimed at improving clinical outcome. These changes made it possible to record and store large amounts of patient data in PD centers for later use in research.
At the same time, especially since the beginning of the new century, there was a push for more research in the medical society in China, because research was and still is tightly linked with career development among the new generation of doctors. As mentioned above, several young nephrologists were well trained in world-class universities and hospitals, and when they returned, they usually had a high capability and motivation to report data from their centers. Furthermore, key PD guidelines have been translated into Chinese since 2010, facilitating their application among Chinese doctors, and guiding and prioritizing research interests. The guidelines clearly stated future research trends and the need for high-level evidence in some critical areas to solve clinical problems, which stimulated research in these fields (45,46). Finally, industry research funding in preferred topics guided PD research in the hottest research areas, such as continuous quality improvement (CQI) in PD centers (15,16,18,19), preservation of residual renal function (RRF) (47), and new training models for startup PD centers (28). Such grants give young doctors a unique opportunity and possibility to benefit from funding for projects focusing on PD studies. The procedure to draft and submit applications is also a learning process. Whether they succeed or fail, applying for a research project and documenting experiences and research interests helped pave the way for Chinese researchers to get into PD research.
Impact on Clinical Practice
While a Kt/V of 2.0 was generally recommended in the late 1990s, following the publication of the large cohort study by the Canada-USA Peritoneal Dialysis Study Group (CANUSA) (48), some of the results from that study were not supported by a subsequent publication, which prospectively observed patient survival among patients with different levels of urea removal in China. The results of the latter study indicated that a Kt/V of 1.7 might be a more reasonable target among Chinese patients (49). Partially due to the economic situation at that time, the lower Kt/V target was followed by many PD programs, and was more generally approved several years later at a national consensus meeting on chronic PD therapy (50). In the same year, the Chinese study was cited as one of the references which supports a Kt/V clearance target of 1.7 that was now recommended by the 2006 ISPD adequacy guideline (51). These publications triggered an argument in China as to whether it is acceptable for patients to start with 3 exchanges per day in the early stage of PD therapy instead of the standard regime of 4 exchanges. Although there was no strong evidence to support this theory, many patients in China were starting dialysis with 3 exchanges when they had a certain level of residual renal function. It is not until recently that there was a randomized control trial (RCT) comparing renal function decline and patient survival in patients using 3 vs 4 exchanges. This study (32) showed that starting with 3 exchanges per day appears to be a safe regimen if patients are carefully monitored.
Another example comes from Peking University. Physicians realized that the bag exchange procedure at home was rarely monitored after the first round of training in the hospital, and they hypothesized that improper procedures may be a risk factor for peritonitis in incident patients. In a prospective observational study (52), clinical characteristics and bag exchange procedures were evaluated at 6 months after the start of PD therapy in incident patients. The study showed that not wearing a facemask and cap, as well as having anemia, were independent risk factors for peritonitis. This provides evidence to support the importance of providing patient education according to the International Society for Peritoneal Dialysis (ISPD) guidelines (53,54), which have since been widely applied in continuous medical education courses and in patient education programs in China.
Recently, a series of studies on peritonitis has been reported from Sun Yat-sen University Hospital, Guangzhou, showing among other things that peritonitis caused by extended-spectrum β–lactamase (ESBL)-producing Escherichia coli is associated with poorer prognosis (55) and that its incidence has been increasing continuously (56,57). In a study of 90 episodes of E. coli peritonitis (58), the risk of treatment failure was significantly increased when the patient had more severe comorbidities at baseline or had diabetes or hypoalbuminemia on admission. Prolonging the treatment course from 2 to 3 or more weeks reduced the risk of relapsing peritonitis. Without doubt, the results of the study guided clinical practice to further improve the cure rate among patients with peritonitis due to E. coli, and they were cited in the recent ISPD guidelines (54). The same team published further papers on preventing peritonitis by adjusting the patient–doctor contact interval (45) and addressing risk factors for the first episode of peritonitis, such as hypoalbuminemia (46). The impact of these and other Chinese studies on clinical practice is reflected in the introduction of new center management practices, including increased patient involvement, such as the use of patient education focus groups.
Barriers and Difficulties for Advanced Research
Although PD is becoming one of the hotter topics in nephrology research in China, the ability of Chinese researchers, especially in terms of raising hypotheses, designing and writing study protocols, analyzing data, and writing manuscripts that can be accepted in major journals, still has large gaps with opportunities for improvements. The curriculum for research training in medical school is very limited and such training is only included in post-graduate programs. Around 80% of local papers are published in non-major medical journals. In order to create more definitive and meaningful clinical research, there is an absolute need to run training courses, especially on basic statistics, or have statisticians in place to provide comments on study proposals. The Dialysis Scientific Training of Academic Research (DSTAR) program, which is led by local journal editors and senior researchers and sponsored by industry, is a good example. The format of DSTAR with small-scale discussion and sharing of research-related questions, e.g., study design, sample size calculation, etc., has been well accepted by young researchers. So far, 500+ doctors have benefited from DSTAR or similar training courses.
Secondly, the majority of Chinese studies are single-center reports, which may impede their value and application in clinical practice. On the other hand, it is hard to implement multicenter studies in China due to the lack of experience and diversified research interests. However, there are some collaborative studies, which have been extremely successful. To start, there was a series of cohort reports, involving networks of PD centers, which involved close collaboration among Chinese centers (42,59,60). With an open-minded, shared-resource, and collaborative spirit, more multicenter studies, either designed as RCTs or cohort studies, should be considered and implemented. Such studies will accumulate data and provide strong evidence to support local guidelines focusing on Chinese patients. In addition, such collaborations, which may include large numbers of patients, may in turn expand the impact of Chinese research findings on clinical practices worldwide.
Thirdly, while existing data show that clinical outcomes of PD among Chinese PD patients in general are equal to or better than their Western counterparts (20, 22–24), there is a lack of published national data that provides a global picture of PD quality around the country. The reports from modern large cities among relatively wealthy patients can hardly be said to represent the much poorer patients from the western and inner rural areas of China. With the establishment of the Chinese National Renal Data System (http://www.cnrds.net/) (61), which started collecting dialysis data nationwide 8 years ago, more solid and complete data will become available. Finally, when we compare data with Western countries, it should be noted that the clinical outcomes of PD therapy in China were obtained using basic products (conventional dextrose-based solutions and manual PD, not automated PD). Therefore, better outcomes should be expected when more advanced solutions and improved technologies are introduced in the near future.
Future Research
It is worth mentioning that some ongoing studies, which may answer current unsolved questions, are soon to be completed. For example, the results of a large RCT on quality of life in PD compared with hemodialysis (HD) will soon be available. This is important because outcome comparisons between HD and PD based on studies using RCT design have all failed due to the difficulties of running such studies. Furthermore, it may be more meaningful to focus on quality of life rather than patient survival (62), as we know now that survival is similar for dialysis patients treated by PD or HD. The ChinaQ study, which recruited 900+ patients with a RCT design in China [ChinaQ,NCT02378350] has just ended. Within the coming year, it will tell us whether quality of life is equal in HD and PD patients. Furthermore, there are several other ongoing studies in China that also deserve international attention, such as one focusing on the PD registration system (PERSIST, NCT02989298) and another exploring the potentials of a PD telemedicine management platform-based cohort (PDTAP, to be registered). These 2 national-level prospective cohort studies will explore associations between clinical characteristics and multiple clinical outcomes based on baseline and follow-up information in PD patients.
More and better PD research is rapidly emerging in mainland China. Through managing the barriers mentioned above, we may be able to answer important questions, such as 1) does nurse/patient ratio matter? 2) Is PD a more cost-effective therapy in a developing country like China? 3) Is PD more suitable for Asian/Chinese? 4) Will remote monitoring techniques help to improve patient outcomes? With these prospects in mind, China is destined to become a true global leader in research for PD therapy.
Footnotes
QY, TF, and BL are employees of Baxter Healthcare. JD has lectured at scientific meetings arranged by Baxter Healthcare. Baxter Novum is the result of a grant from Baxter Healthcare to Karolinska Institutet.