
Abstract
Background
The optimal methodology of establishing access for peritoneal dialysis (PD) remains controversial. Previously published randomized controlled trials and cohort studies do not demonstrate an advantage for 1 technique over another. Four published meta-analyses comparing outcomes of laparoscopic versus open PD catheter (PDC) insertion have given inconsistent conclusions and are flawed since they group basic and advanced laparoscopy together. The aim of this systematic review and meta-analysis is to examine whether advanced laparoscopic interventions consisting of rectus sheath tunneling and adjunctive procedures produce a better outcome than open insertion or basic laparoscopy used only to verify the catheter position.
Methods
A literature search using Medline, Embase, and Cochrane Database was performed, and meta-analysis was performed using RevMan 5.3.5 software (Nordic Cochrane Centre, The Cochrane Collaboration, London, UK). Outcomes evaluated incidence of catheter obstruction, migration, pericannular leak, hernia, infectious complications (peritonitis and exit-site infection) and catheter survival.
Results
Of the 467 records identified, 7 cohort studies, including 1,045 patients, were included in the meta-analysis. When advanced laparoscopy was compared with open insertion, a significant reduction was observed in the incidence of catheter obstruction (odds ratio [OR] 0.14, 95% confidence interval [CI] 0.03 – 0.63; p = 0.01), catheter migration (OR 0.12, 95% CI 0.06 – 0.26; p = 0.00001), pericannular leak (OR 0.27, 95% CI 0.11 – 0.64; p = 0.003), and pericannular and incisional hernias (OR 0.29, 95% CI 0.09 – 0.94; p = 0.04), as well as better 1- and 2-year catheter survival (OR 0.52, 95% CI 0.28 – 0.97; p = 0.04 and OR 0.50, 95% CI 0.28 – 0.92; p = 0.03, respectively). Compared with basic laparoscopy, catheter obstruction and migration were significantly lower in the advanced laparoscopic group, whereas catheter survival was similar in both groups. All outcomes, except catheter obstruction, were similar between the basic laparoscopy and open insertion. The infectious complications such as peritonitis and exit-site infections were similar between the 3 groups.
Conclusions
Advanced laparoscopy was associated with a significant superior outcome in comparison with open insertion and basic laparoscopy.
A PDC can be inserted into the peritoneal cavity employing open surgical, blind percutaneous, fluoroscopically-guided percutaneous, peritoneoscopic, and laparoscopic techniques. Over the past 6 decades, the open surgical technique of PDC insertion has been adopted worldwide because of its ease of application and perceived low cost to healthcare providers. The introduction of laparoscopic insertion by Amerling et al. in 1993 offers potential advantages over other techniques, including the ability to insert the catheter under direct vision, which ensures correct position of the catheter, reduced length of hospital stay, morbidity, postoperative pain, and recovery period, and improved catheter survival (2). The major strengths of laparoscopy include the prevention and resolution of common mechanical problems that adversely affect catheter outcomes.
The laparoscopic insertion technique may be either basic, where the laparoscope is used to verify the position of the catheter, or advanced. The advanced technique, introduced by Crabtree et al., includes rectus sheath tunneling (RST) and adjunctive procedures such as omentopexy, adhesiolysis, excision of appendix epiploica (epiploectomy), salpingectomy, and colopexy (3,4). It facilitates laparoscopic visualization of the peritoneal cavity for adhesions and hernias. Through a paramedian approach, with or without the help of a trocar, the PDC is inserted so that a length of 4 to 6 cm of the catheter passes through a tunnel in the rectus sheath on the surface of the posterior rectus sheath prior to its entry into the peritoneal cavity inferior to the arcuate line. A long course of the catheter in the rectus sheath and a short course in the peritoneal cavity prevents migration and omental wrapping. In addition, omentopexy is carried out either as routine or selectively, where the redundant omentum is anchored to the anterior abdominal wall of the upper abdomen (5).
Currently, there are 4 published meta-analyses comparing the outcomes of laparoscopic versus open PDC insertion (6–9). However, all of these meta-analyses are flawed, as they group together studies that have used both basic and advanced laparoscopic techniques. They therefore are unable to explore the potential advantages of the advanced laparoscopic technique.
The aim of this systematic review and meta-analysis is to examine the outcomes of advanced laparoscopic PDC insertion technique in adults and compare them with those of the open insertion and basic laparoscopic insertion techniques.
Methods
Literature Search Strategy
A systematic electronic literature search was performed in PubMed, EMBASE, and Cochrane Library databases from inception to 20 September 2017. The search terms “peritoneal dialysis,” “laparoscopy,” “laparotomy,” “open,” “rectus sheath,” tunnelling,” “preperitoneal,” and “catheter” were used. There was no language restriction. All articles relevant to the laparoscopic or open insertion of PDC were identified, reference lists of relevant studies were further scrutinized for additional citations, and all pertinent references were compiled in the EndNote software (Version X 7.4; Thomson Reuters, Philadelphia, PA, USA).
Literature Screening
The authors independently screened the titles and abstract of the records identified in the electronic searches, excluding all obviously not relevant studies, and examined the full texts of potential studies. Any discrepancies in eligibility judgments were resolved by discussion between the authors. The studies had to describe 1 or more of the following outcome measures: the incidence of catheter obstruction, migration, pericannular leak, hernia, peritonitis, exit-site/tunnel infection, and catheter survival.
Clinical question structured in PICOM format
Is advanced laparoscopic insertion of PDC associated with improved outcomes compared with open or basic laparoscopic insertion techniques?
Exclusion criteria
Duplicate publications and those which did not conform to the PICOM format were excluded.
Data Extraction and Critical Appraisal
The methodological quality of the observational cohort studies was assessed using the Newcastle-Ottawa scale (NOS); the quality score was calculated based on 3 major components: selection of the group of study (0 – 4 points), comparability of the group (0 – 2 points) and assessment of the outcome (0 – 3 points). The maximum of 9 points represents the highest methodological quality; a NOS score of 7 or more was considered a “good” study (10). The level of evidence of individual studies was assessed using the Oxford Centre of Evidence-Based Medicine – Level of Evidence document (11). Quality and potential for bias of the randomized controlled trials was evaluated using the Cochrane Collaboration's tool for assessing risk of bias by Higgins (12).
Statistical Methods
The meta-analysis was performed using RevMan 5.3.5 software (Nordic Cochrane Centre, The Cochrane Collaboration, London, UK). Heterogeneity of treatment effects between studies was assessed using the Q (heterogeneity chi square (χ2) and the I2 statistics. For I2, > 50% indicated significant heterogeneity in the studies, and in this situation a random-effects model was used. For homogeneous studies, a fixed-effects model and the Mantel–Haenszel (M-H) method for calculation was adopted. For smaller event rates (0 – 1), the Peto method was applied. For dichotomous outcomes, we reported results as an odds ratio (OR), while in reporting continuous outcomes, weighted mean difference (WMD) was used. Summary estimates and 95% confidence intervals (CIs) were calculated. Overall effects were determined by the using Z-test. A p value < 0.005 was considered significant. Forest plots were drawn based on these results. The minimum number of studies considered appropriate for display of a forest plot was 2 (13). Finally, the quality of each conclusion was assessed by the GRADE tool (GRADEpro GDT, Cochrane Community, London, UK) (14). Univariate analysis was performed on the studies of advanced laparoscopy that did not have control groups by comparing their outcomes with control groups from the open insertion studies used in the meta-analysis. Epi Info (V7.2.1.0, supplied by Centre for Disease Control and Prevention, Atlanta, GA, USA) was used for the univariate analysis.
Results
Search Results
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow diagram is presented in Figure 1. The search yielded 467 records, of which 7 cohort studies, including 1,045 patients, were included in the meta-analysis group that compared advanced laparoscopy with open insertion and basic laparoscopy (Table 1). There were 14 studies of advanced laparoscopic PDC insertion that did not include a comparator group (Table 2). Seven studies compared basic laparoscopy with the open insertion technique (Table 3).
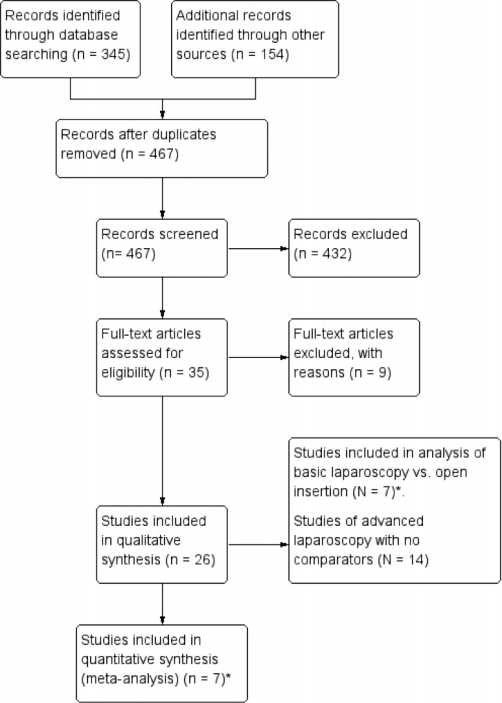
PRISMA flow diagram of the systematic literature search. * 2 studies (3 and 16) compared advanced and basic laparoscopic with open-insertion technique.
Characteristics of the Studies Comparing Advanced Laparoscopic, Basic Laparoscopic, and Open PDC Insertion
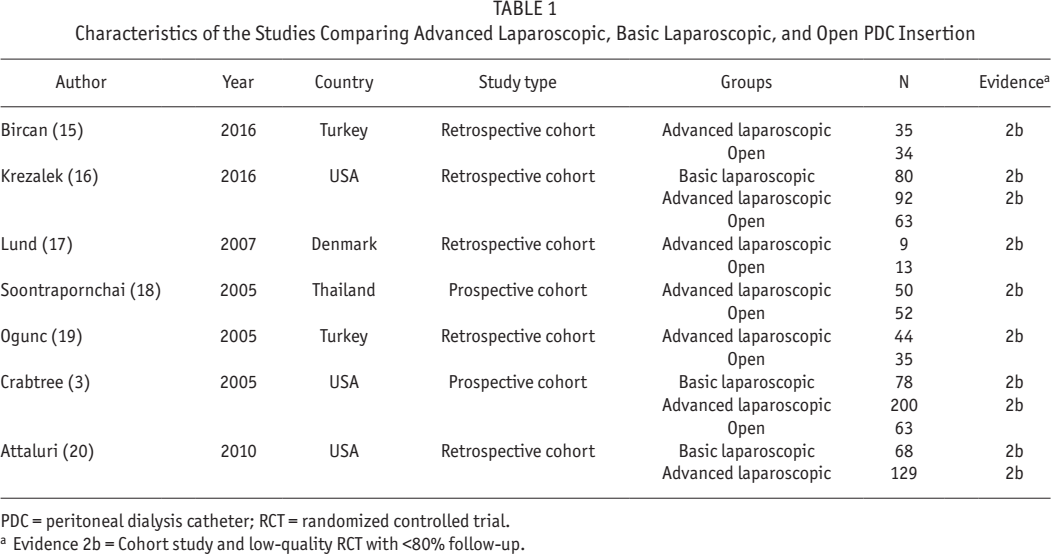
PDC = peritoneal dialysis catheter; RCT = randomized controlled trial.
Evidence 2b = Cohort study and low-quality RCT with <80% follow-up.
Characteristics of the Studies Including Advanced Laparoscopic PDC Insertion without Comparators
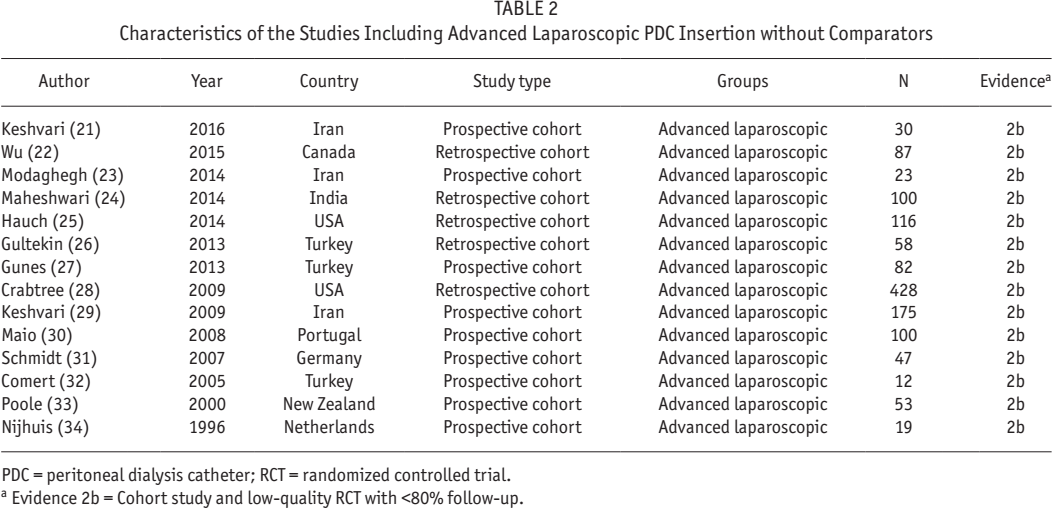
PDC = peritoneal dialysis catheter; RCT = randomized controlled trial.
Evidence 2b = Cohort study and low-quality RCT with <80% follow-up.
Characteristics of the Studies Comparing Basic Laparoscopic and Open PDC Insertion
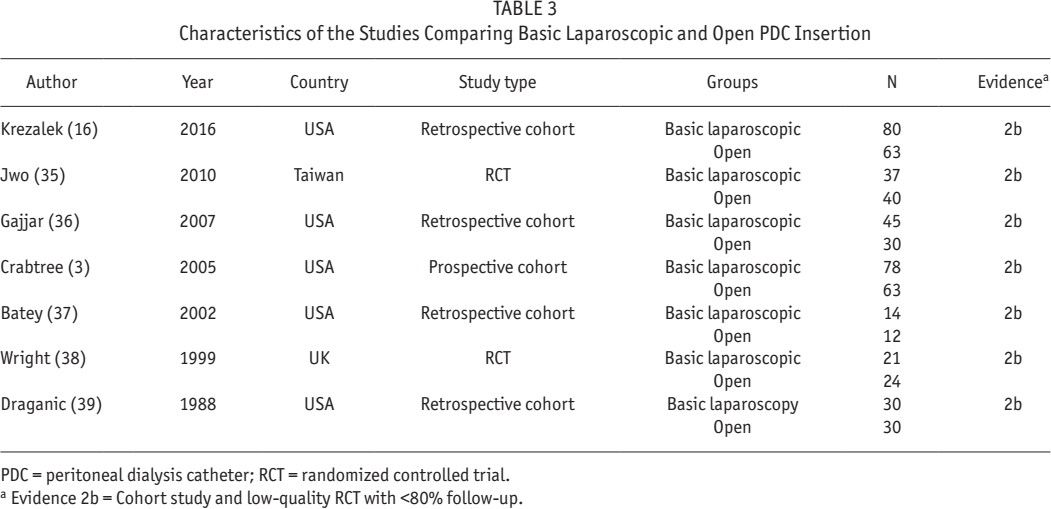
PDC = peritoneal dialysis catheter; RCT = randomized controlled trial.
Evidence 2b = Cohort study and low-quality RCT with <80% follow-up.
Study Quality
There was no RCT comparing advanced laparoscopy with open insertion or basic laparoscopy. With NOS criteria, the cohort studies scored an average of 6.3 points, indicating medium quality (3,15–20).
Advanced Laparoscopy Vs Open Insertion
Catheter-related outcomes
In the 5 studies (3,15,16,18,19) involving 668 patients that compared the outcomes of advanced laparoscopy with open insertion and were included in the meta-analysis, catheter obstruction occurred significantly less frequently in the advanced group (Figure 2A). Catheter migration was examined in 5 studies (15 16 17 18-19) including 427 patients, demonstrating a lower incidence of catheter migration in the advanced laparoscopy group (Figure 2B). The incidence of pericannular leak was reported in 5 studies (3,15,16,18,19), including 668 patients, and their meta-analysis significantly favored the advanced laparoscopy group (Figure 2C).
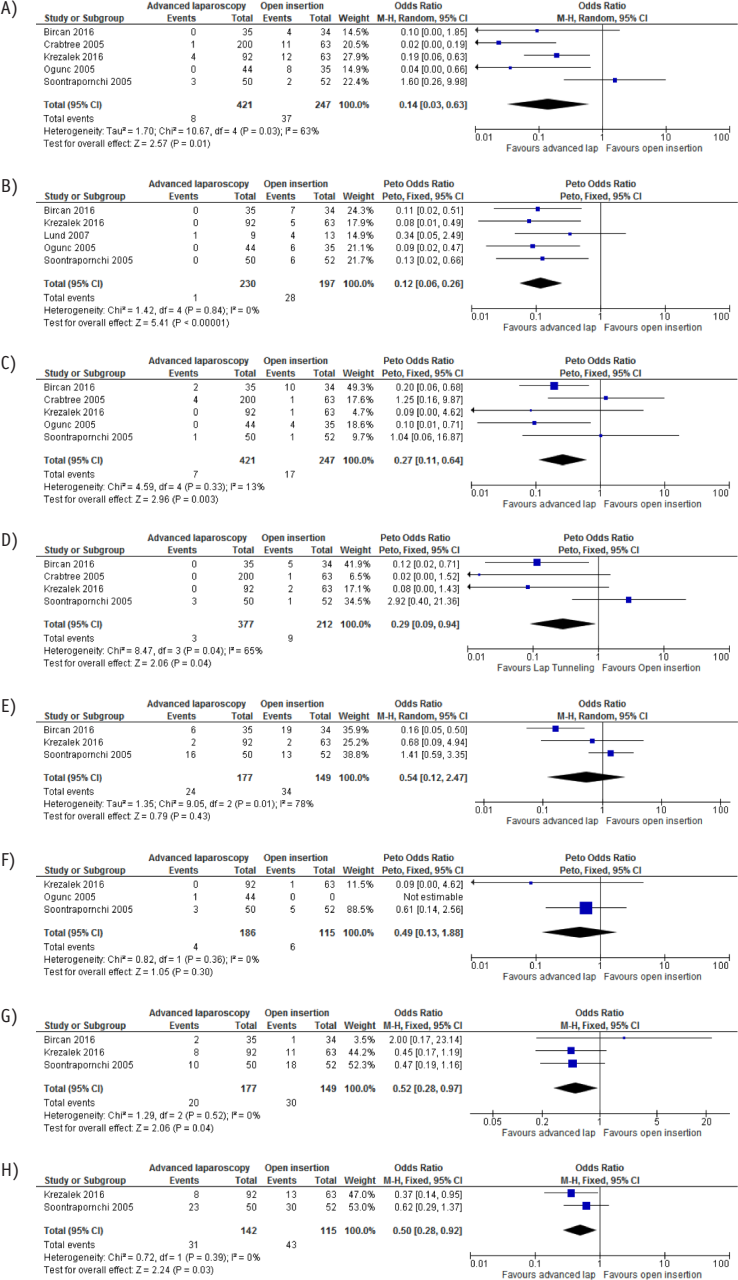
Forest plots comparing advanced laparoscopy and open insertion. A) Risk difference of catheter obstruction. B) Risk difference of catheter migration. C) Risk difference of pericannular leak. D) Risk difference of pericannular and incisional hernias. E) Risk difference of peritonitis. F) Risk difference of exit-site infection. G) Risk difference of the 1-year catheter survival rate. H) Risk difference of the 2-year catheter survival rate. M-H = Mantel–Haenszel; CI = confidence interval; df = degrees of freedom.
Hernia
The incidence of pericannular and incisional hernias (4 studies (3,15,16,18) involving 589 patients) was significantly less frequent in the advanced laparoscopy group (Figure 2D).
Infections
Three studies that investigated the incidence of peritonitis after PD catheter insertion were included in the meta-analysis, with a total of 326 patients (15,16,18). There was no statistically significant difference in the risk of developing peritonitis between the groups (Figure 2E). Similarly, 3 studies (16,18,19), involving 301 patients, showed no significant difference in the incidence of exit-site infection between the 2 groups (Figure 2F).
Catheter survival
The 1-year (Figure 2G) (15,16,18) and 2-year (Figure 2H) (16,18) catheter survival rates were better in the advanced laparoscopy group.
Advanced Vs Basic Laparoscopic Insertion
Catheter-related outcomes
In the 3 studies (3,16,20), involving 647 patients, that compared the outcomes of advanced laparoscopy with basic laparoscopy, catheter obstruction occurred significantly less frequently in the advanced laparoscopy group (Figure 3A) (3,16,20). Two studies involving 369 patients showed no migration of PD catheter in the advanced laparoscopy group (Figure 3B) (16,20). There was no significant difference in the incidence of pericannular leak between the 2 groups (Figure 3C) (3,16,20).
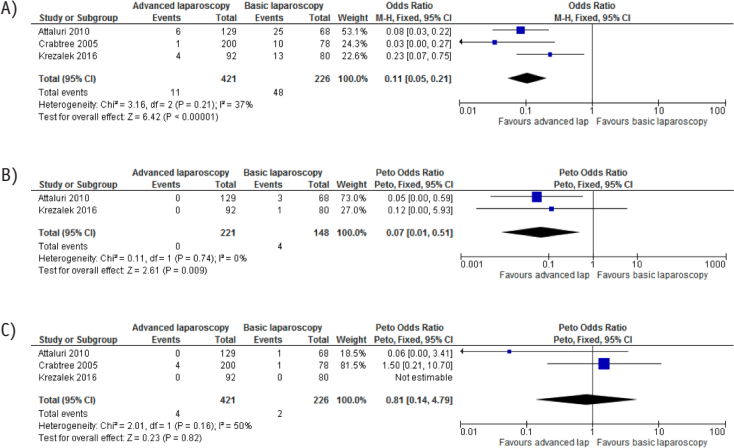
Forest plots comparing advanced and basic laparoscopic PDC insertion groups. A) Risk difference of catheter obstruction. B) Risk difference of catheter migration. C) Risk difference of pericannular leak. PDC = peritoneal dialysis catheter; M-H = Mantel–Haenszel; CI = confidence interval; df = degrees of freedom.
Infections
The incidence of peritonitis (3.75% vs 1.84%; p = 0.66) and exit-site infection (1.25% vs 0%; p = 0.21) was reported in 1 study (16), and these were not significantly different between the basic and advanced laparoscopic groups.
Catheter survival
One- and 2-year catheter survival was reported in 1 study (16): 85% in the basic and 91% in the advanced laparoscopic groups (p = NS). There was no report of bleeding or incisional hernia in either group.
Basic Laparoscopy Vs Open Insertion
Outcomes
In the meta-analysis, the incidences of catheter obstruction (5 studies; 464 patients) (3,16,36,38,39), catheter migration (3 studies; 246 patients) (16,35,37), pericannular leak (6 studies; 507 patients) (3,16,35,36,38,39), peritonitis (6 studies; 426 patients) (16,35–39); exit-site infection (5 studies; 400 patients) (16, 5,36,38,39); and 1-year survival (2 studies; 188 patients) (16,38) were compared between basic laparoscopy and open PDC insertion groups. Catheter obstruction occurred significantly less frequently in the basic laparoscopy group (Figure 4A). The incidence of catheter migration, pericannular leak, peritonitis, exit-site infection, and 1-year survival (Figures 4B to 4F) did not differ between the 2 groups.
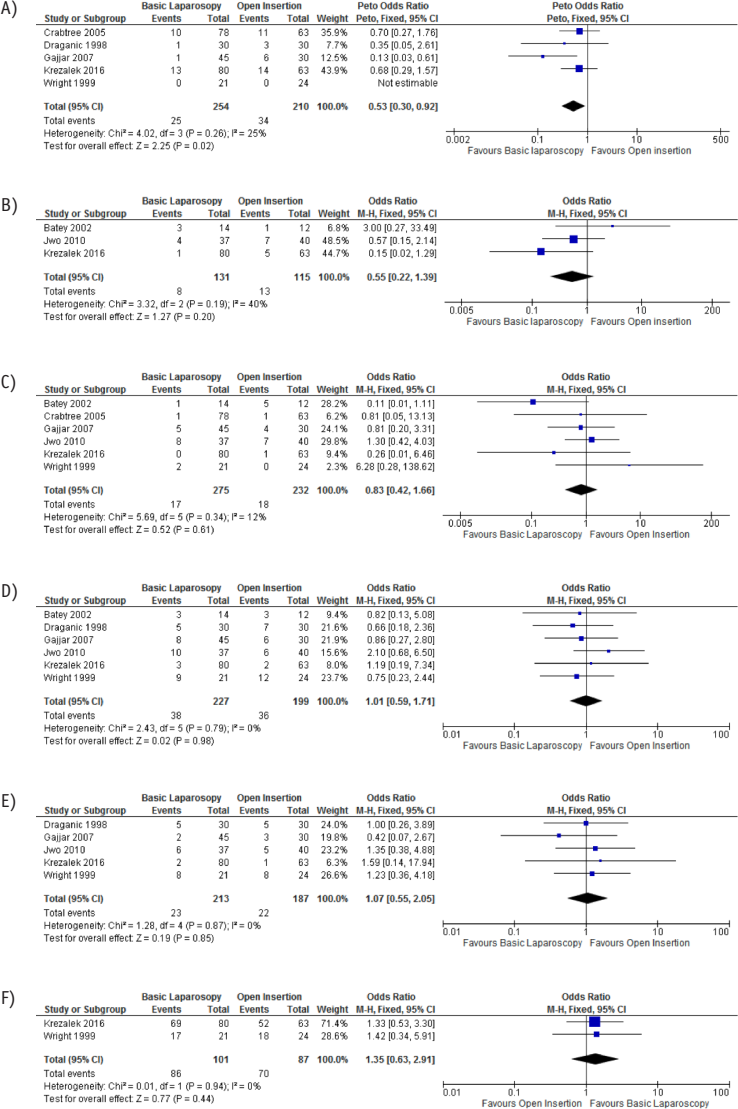
Forest plots comparing basic laparoscopic and open PDC insertion groups. A) Risk difference of catheter obstruction. B) Risk difference of catheter migration. C) Risk difference of pericannular leak. D) Risk difference of peritonitis. E) Risk difference of exit-site infection. F) Risk difference of 1-year catheter survival. PDC = peritoneal dialysis catheter; M-H = Mantel–Haenszel; CI = confidence interval; df = degrees of freedom.
Studies of Advanced Laparoscopic Insertion without Comparators
Fourteen cohort studies (21 22 23 24 25 26 27 28 29 30 31 32 33-34) were identified, including 1,330 patients who underwent advanced laparoscopic PDC insertion, that did not have comparators (Table 2). The incidence of catheter obstruction, migration, and pericannular leak was 4.6%, 0.8%, and 3.9%, respectively. Further details are available in the supplemental file (S1).
Discussion
This systematic review and meta-analysis has shown that the advanced laparoscopic PDC insertion, including RST and an adjunctive procedure such as omentopexy, produces a better outcome compared with conventional open and basic laparoscopic insertion techniques. The incidence of catheter obstruction, migration, pericannular leak, and hernias was significantly lower, and catheter survival at 1 and 2 years was better following advanced laparoscopy.
Several studies have examined the synergistic effect of combining RST, selective omentopexy, and adhesiolysis in terms of catheter dysfunction and catheter survival rates with (3,15–20) or without (21–34) comparison with open and basic laparoscopic insertion techniques. Crabtree et al. published the largest case series, which examined 428 patients who had a PDC placed using RST along with selective omentopexy and adhesiolysis. During the mean follow-up of 21.6 months, the overall catheter obstruction rate was 3.7% and the pericatheter leak rate, 2.6%. Only 0.9% of catheters were removed due to mechanical complications, and only half of them transferred to hemodialysis. Cumulative revision-free and assisted catheter survival probabilities for loss from mechanical complications at 5 years were 96% and 99%, respectively (28).
Ogunc published a case series of 44 patients who had a PDC inserted using RST, omentopexy indiscriminately, and selective adhesiolysis in 5 patients. After a median follow-up of 17.4 months, they observed no cases of catheter obstruction, migration, pericatheter leak, and pain. This was compared with their previous 35 open insertion cases, where catheter obstruction, migration, and pericatheter leak occurred in 22.8%, 17.1%, and 11.4%, respectively (19).
Crabtree and Fishman, in their prospective non-randomized case study consisting of 63 catheters implanted by traditional open dissection, 78 catheters implanted by basic laparoscopy without associated interventions, and 200 catheters implanted by advanced laparoscopy including RST, selective omentopexy, and selective adhesiolysis, observed catheter flow obstruction in 1/200 patients (0.5%) in the advanced laparoscopy group, 17.5% in the open dissection, and 12.5% in the basic laparoscopy group (p < 0.0001) (3).
Krezalek et al. published the outcomes of a cohort of 235 procedures using open technique in 63, basic laparoscopy with adhesiolysis in 80, and advanced laparoscopy including RST, selective omentopexy, and adhesiolysis in 92 patients. Mechanical catheter dysfunction occurred in 4 patients (4.5%) in the advanced laparoscopy group, 14 (17.5%) in the basic laparoscopy group, and 20 (31.8%) in the open group (p < 0.01). The rate of switch to hemodialysis was significantly lower in the advanced laparoscopy group (16).
Lastly, Attaluri et al. compared 68 patients in the basic laparoscopy group with 129 patients in the advanced laparoscopy group using RST and selective prophylactic omentopexy. They observed a catheter obstruction rate of 4.6% in the advanced laparoscopy group and 36.8% rate in the basic laparoscopy group (20).
This meta-analysis comparing the outcomes of basic laparoscopy with open PDC insertion showed a significantly lower incidence of catheter obstruction in the former group. However, other outcomes were similar between the 2 groups, which differs from the meta-analyses published previously (9,40). A prospective study by Li et al. (41) and a RCT by Tsimoyiannis et al. (42) compared catheter-related outcomes between laparoscopic and open insertion of PDC. In both studies, catheter immobilization was carried out by suturing the catheter to the lower abdominal wall in the former and to the uterus in females and bladder wall in males in the latter study. Because both studies differed from the rest of the advanced laparoscopic and basic laparoscopic groups in the method of suture fixation, they were not included in our meta-analysis. Both groups reported a significantly reduced rate of catheter migration. In a review article by Frost et al., it was recommended that proper RST and placement of deep cuff within the rectus sheath are the key to reducing catheter tip migration. Suture fixation can be associated with difficulty in catheter removal as well as being a potential cause of internal hernia or adhesion (43). Suture fixation may also impair the natural ability of the catheter to float to the largest area of PD fluid. Bar-Zohar (44) and Lu (45) showed a relatively high catheter dysfunction rate after suture fixation of 14% and 12%, respectively.
The results of this systematic review and meta-analysis reinforce the notion that advanced laparoscopic PDC insertion using RST in all cases, along with selective omentopexy and selective adhesiolysis, is associated with superior outcomes compared with basic laparoscopy and open insertion, in terms of both catheter dysfunction rate and overall catheter survival. There is significant evidence that basic laparoscopic insertion results in similar dysfunction rates as open insertion. The addition of omentopexy has not been studied by itself in any study, but it appears to lower the incidence of catheter dysfunction.
The limitation of this study is the lack of prospective RCTs comparing advanced laparoscopy with other modalities for PDC insertion. The studies included in the meta-analysis were retrospective and non-randomized prospective cohort studies, with a medium quality score on the Newcastle-Ottawa Scale. On assessment of the grades of evidence for each outcome measure using the GRADE tool (GRADEpro GDT, Cochrane Community, London, UK) (14), the observed evidence belonged to low quality (supplemental file S2). A prospective RCT comparing the outcomes of advanced PDC insertion with the 2 other techniques would be ideal. There is a multicenter randomized controlled single-blind trial currently underway in Europe to compare laparoscopic versus open PDC insertion but it was not stated whether this incorporates advanced laparoscopic technique (46).
The results observed from large cohort studies, both prospective and retrospective, suggest that laparoscopic RST and selective omentopexy produce superior outcomes without increasing risks to the patients. For this reason, it may be difficult to justify randomization of patients to open or advanced laparoscopy in a controlled trial. Ensuring a functioning PDC with its longevity is beneficial to the patient and reduces healthcare costs. Therefore, where possible, advanced laparoscopic insertion using RST, selective omentopexy, and adhesiolysis should be the preferred technique for PD catheter insertion.