
Abstract
Remote patient management (RPM) has the potential to help clinicians detect early issues, allowing intervention prior to development of more significant problems. A 23-year-old end-stage kidney disease patient required urgent start of renal replacement therapy. A newly available automated peritoneal dialysis (APD) RPM system with cloud-based connectivity was implemented in her care. Pre-defined RPM threshold parameters were set to identify clinically relevant issues. Red flag dashboard alerts heralded prolonged drain times leading to clinical evaluation with subsequent diagnosis of and surgical repositioning for catheter displacement, although it took several days for newly-RPM-exposed staff to recognize this issue. Post-PD catheter repositioning, drain times were again normal as indicated by disappearance of flag alerts and unremarkable cycle volume profiles. Identification of < 90% adherence to prescribed PD therapy was then documented with the RPM system, alerting the clinical staff to address this important issue given its association with significant negative clinical outcomes. Healthcare providers face a “learning curve” to effect optimal utilization of the RPM tool. Larger scale observational studies will determine the impact of RPM on APD technique survival and resource utilization.
Clinician visibility to patient- and therapy-related issues has heretofore been problematic given the remote nature of home-based dialysis. The availability and application of a remote patient management (RPM) platform to monitor and modify automated peritoneal dialysis (APD) treatment parameters offer clinicians the potentiator earlier identification and intervention of PD-related problems occurring in the home. The present case report demonstrates the use of cycler-embedded RPM in identification of problematic draining that Led to diagnosis and ensuing correction of PD catheter migration. Non-adherence to prescribed therapy was also identified and addressed.
Case Report
A 23-year-old ESKD patient required hospitalization for urgent start of renal replacement therapy. Because of prior non-adherence, a newly available APD cycler with an embedded 2-way RPM system (Claria-Sharesource; Baxter Healthcare Corporation, Deerfield, IL, USA) was implemented in her care. Post-APD training and on return home, the patient's treatment was both remotely observed and altered regularly. Pre-defined RPM threshold parameters were set to identify clinically relevant issues.
The RPM system initially revealed no dashboard flag alerts and normal PD cycle volume profiles (Figure 1A). Subsequently, red flag dashboard alerts appeared (Figure 2A). It took several days before newly-RPM-exposed staff analyzed volume profiles and noticed prolonged drain times (Figure 1B), finally prompting them to call the patient for urgent clinical evaluation and radiological investigations. This led to a diagnosis of catheter displacement and surgical repositioning of the catheter after an unsuccessful conservative approach with laxatives. Post-PD catheter repositioning, drain times were again normal as indicated by the disappearance of flag alerts (Figure 2B) and unremarkable cycle volume profiles, except for one on February 28. The fill profile of the sixth cycle on that date (Figure 1C) was compatible with a resolving inflow occlusion, in keeping with a kinked or compressed line relieved by the patient (i.e. shift in patient position). Finally, identification of < 90% adherence to prescribed PD therapy was documented with the RPM system a few months later (Figure 2C) alerting the clinical staff to address this important issue, given its association with significant negative clinical outcomes.
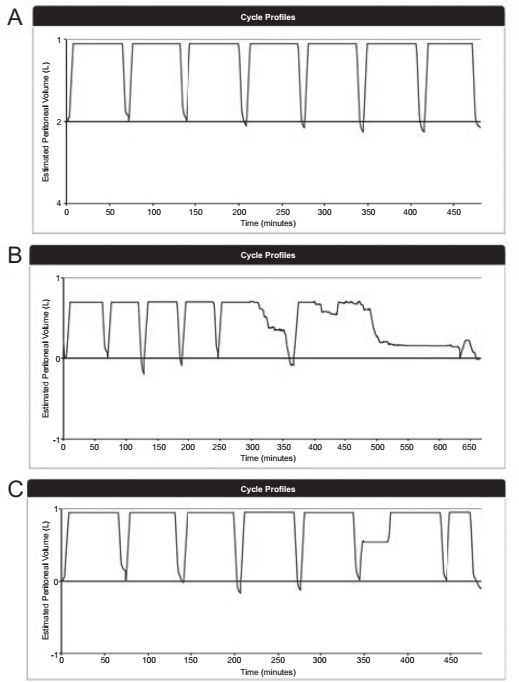
Cycle volume profiles. A: normal; B: prolonged drain times; C: transient inflow obstruction.
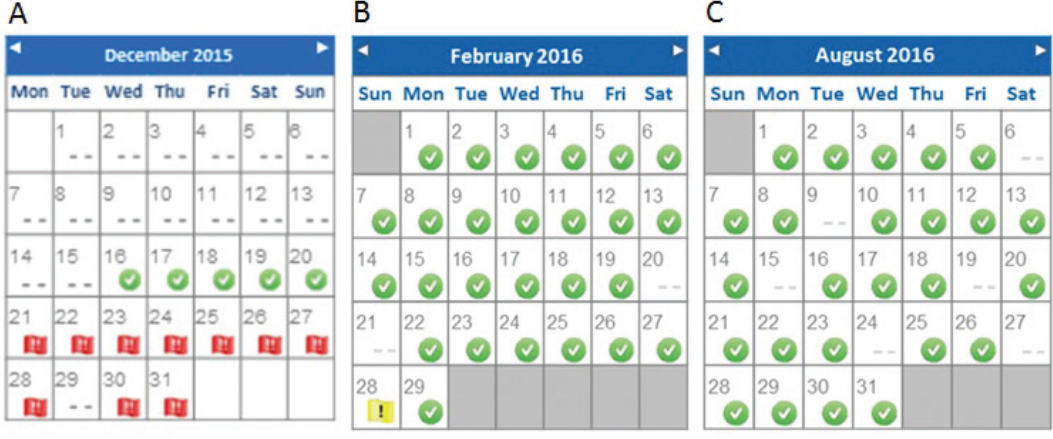
Monthly overview diagrams. A: red flags indicating an issue; B: green flags indicating unremarkable PD therapy course; C: absent marks identifying 20% non-adherence to prescribed PD therapy.
Discussion
Early technique failure can Lead to Lack of confidence in the success of PD for both patients and clinicians, contributing to a decreased willingness to embrace PD as a viable form of renal replacement therapy. Recent preliminary global data reveal that catheter-related issues and leaks are the leading causes of technique failure in the first 120 days of PD, accounting for 37% of all transfers to in-center hemodialysis (Personal communication, Arbor Research, Ann Arbor, MI, USA, 2017). The case report described here demonstrates the identification of prolonged drain times through an APD-embedded RPM platform that led to clinical evaluation and radiological investigations with diagnosis and ensuing correction of PD catheter displacement. While it took the clinical staff, naive to RPM prior to its use in this patient, several days to analyze the data and intervene for poor PD catheter drainage, it is unclear if or when slow catheter drain times would have been reported by the patient. As catheter migration can lead to progressive volume overload, unintended increased intraperitoneal volume or other adverse events with potential negative impact on therapy success and subsequent technique failure, early diagnosis is of the utmost importance. In this context, any tool that can alert clinicians to an occurring issue and lead to earlier clinical evaluation and discussion with the patient about encountered problems during PD treatment is valuable. Worthy of note, RPM-transmitted drain profiles do not differentiate the cause of abnormal drain flow, which still requires clinical evaluation.
As already mentioned, non-adherence of > 10% has a major negative impact on long-term prognosis and should therefore be actively evaluated and quickly addressed, and RPM could be of great help in this setting. According to recent data, non-adherence rates in PD are high, ranging from 2.6 - 53% for dialysis procedures (10). Young patients may be particularly at risk (11), possibly because they are more likely to be occupation-ally and socially active and therefore confronted with logistic challenges in following the convention of traditional treatment (12); they may, however, feel disturbed in their privacy by RPM and this potential down-side should be addressed in the future.
Remote patient management could offer further advantages to patients with physical, geographic, and social limitations. As it spares patients the necessity of coming to the PD clinic for treatment analysis and potential subsequent modification, some specific populations, such as people with reduced mobility, could particularly benefit from it. Although regular clinical evaluation is mandatory for the good care of PD patients, RPM could help maintain the frequency of visits to the clinic at the minimal security threshold, typically on a monthly basis, for such populations. Moreover, clinical follow-up of patients can be further improved as APD cycler-embedded RPM affords important daily clinical data such as blood pressure values and daily weights provided before each PD therapy is initiated, the main limitation being potential voluntary or involuntary human errors. Bluetooth enabling is a necessary enhancement to overcome these problems. Finally, RPM could improve clinician time-efficiency, enabling identification of patients flagged as having potential clinical issues, who could then be prioritized.
Issues should be recognized sooner than in the case described here where red flags associated with poor catheter function persisted for at least 10 days before being fully addressed. Remote patient management is just now being more broadly adopted for home dialysis. As might be expected with use of any new tool, efficient practice only evolves through a Learning curve. Mechanisms to accelerate and share best RPM practices, both to facilitate more effective use in improving outcomes and to avoid the setting of alerts that contribute more noise than benefit, need to be developed. Remote patient management internet forums and clinical decision support guides may help serve this purpose.
In conclusion, RPM is a promising tool that may help clinicians to improve PD therapy outcomes and both patient and clinician confidence in embracing home dialysis. It is nevertheless certainly not a substitute for clinical evaluation and communication with the patient. Clinicians must also review dashboards on a daily basis, at least for patients at higher risk for problems. They must furthermore invest the time and effort to learn appropriate and timely responses to alerts if RPM is to impact clinical-economic outcomes. Larger scale observational studies, including the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS), will determine the impact that RPM has on APD technique and patient survival, overall resource utilization, and greater global take-on of home dialysis therapies.
Footnotes
Acknowledgments
The authors would like to thank Deniz Iklim Viol and Derek Wiebenson of Baxter Healthcare for their assistance in obtaining the dashboard screenshots and profiles needed for development of the figures in this manuscript.
We have read and understood Peritoneal Dialysis International's policy on conflicts of interest disclosure and declare the following interests: VJD reports grants and personal fees from Baxter during the conduct of the study. JS is an employee of Baxter Healthcare Corporation. PYM and CSC have nothing to disclose.