
Abstract
Previous studies have indicated a neuroprotective effect of remote limb ischemic preconditioning. The aim of the present study was to assess whether upper arm ischemic preconditioning is feasible and safe in patients with unilateral middle cerebral artery (MCA) stenosis compared to healthy volunteers. Ten patients with unilateral MCA stenosis and 24 healthy volunteers underwent limb ischemic preconditioning, consisting of five cycles of 5-min inflations of a blood pressure cuff to 200 mmHg around an upper limb followed by 5 min of reperfusion. Limb ischemic preconditioning has no significant effect on the heart rate, oxygenation index, or mean flow velocity in patients with unilateral MCA stenosis or healthy volunteers. However, healthy volunteers showed a reduction in blood pressure 30 min following reperfusion of the last cycle. Limb ischemic preconditioning was found to be safe and well tolerated in both patients and healthy volunteers. We highlight the potential of limb ischemic preconditioning as an adjunct to neuroprotective treatment.
Keywords
Introduction
Ischemic preconditioning (IPC) is a phenomenon in which transient periods of ischemia consequently protect against subsequent severe hypoxia (4,21,22,23,28). Preconditioning can be induced locally, where the same organ or tissue receiving the brief period of hypoxia is also the organ that will sustain the ischemic injury, or remotely, where the organ or tissue receiving the ischemic stimulus is different from the organ suffering subsequent ischemia (25). Local ischemic preconditioning resulting in prominent neuroprotection has been extensively reported within the brain, but has been difficult to apply in clinical practice (11). Animal models have shown that remote ischemic preconditioning (RIPC) induced by tightening the upper two thirds of both hindlimbs can increase tolerance to ischemia in the brain (6,11,33,34) and therefore may be a powerful clinical neuroprotective technique that may reduce ischemia–reperfusion injury.
Although the mechanism of RIPC is still unclear, its neuroprotective effects have been proven in animal models. Thus, encouraging neurologists to apply the benefits of RIPC in reducing ischemia–reperfusion injury in clinical settings appears to be important. Clinical trials have shown multiorgan protection against subsequent extended ischemia–reperfusion injury with the use of RIPC (14,24). Walsh et al. reported that RIPC appeared safe in patients with carotid endarterectomy (43). Our team reported that RIPC may be an effective way to improve cerebral perfusion and reduce recurrent strokes in patients with symptomatic atherosclerotic intracranial arterial stenosis (31).
The induction of RIPC depends on sublethal exposure to ischemia. RIPC does not come without risks, as it has been shown that hemodynamic stress may cause arteriolar rupture and that systemic hypotension may induce ischemic stroke (18,43). RIPC's effect on systemic and cerebral hemodynamic changes is important in clinical practice, as its effects on heart rate (HR), breathing rhythm, blood pressure (BP), and cerebral circulation influence its clinical application. However, this trial does not address the safety of RIPC in patients with severe cerebral artery stenosis or a cerebral aneurysm or whether it may induce cerebral ischemia or aneurysm rupture.
Here we reported on our preliminary experience with ischemic limb preconditioning (five cycles of 5 min of upper limb ischemia induced by inflating a BP cuff to 200 mmHg with 5 min of reperfusion) in patients with unilateral middle cerebral artery (MCA) stenosis compared to healthy volunteers. The scientific rationale for the present study was to determine the safety and feasibility of daily remote limb IPC. In view of recent studies implicating stem cell enhancement as a mechanism of action underlying IPC, we discuss its potential as adjunct therapy to stem cell-based regenerative medicine.
Materials and Methods
Subjects
Twenty-four healthy volunteers (male/female 1:1) between 40 and 70 years of age (eight volunteers 40–50 years old, eight volunteers 50–60 years old, and eight volunteers 60–70 years old) were recruited from the Healthy Physical Examination Center at Xuanwu Hospital, Capital Medical University. In addition, 10 patients (male/female 1:1) between the ages of 40 and 65 years (four patients 40–50 years old, three patients 50–60 years old, and three patients 60–65 years old) with unilateral MCA stenosis (>50%) diagnosed by transcranial Doppler (TCD) were also chosen. There were no significant differences between the ages of the two groups (t-test, p > 0.05).
Healthy subjects underwent psychiatric and medical evaluation, which included a physical examination, body weight index measurement, blood test (fasted blood samples and 32 blood indexes were analyzed by the biochemical analysis instrument, including glucose, lactate dehydrogenase, low-density lipoprotein cholesterol, and so on), and an electrocardiogram. Subjects with a history of cardiovascular, cerebrovascular, pulmonary, hepatic, dermatologic, or hematologic diseases were excluded from this study. Pregnancy, diabetes mellitus, obesity, and the use of medications or medical devices were also excluding factors. Finally, patients with an acute stroke within the last 4 weeks, stenosis of the ipsilateral internal carotid artery or the contralateral MCA, or an inadequate temporal window were also excluded. The criteria for MCA stenosis criteria were (10) having a TCD systolic blood flow velocity of ≥160 cm/s and a mean blood flow velocity of ≥100 cm/s. All subjects' characteristics are given in Table 1.
The Demographic Characteristics of All Subjects

Values are mean ± SD.
Informed consent was received from each participant. Subjects fasted 2 h prior to arriving for the study. To keep the testing environment consistent, each subject laid supine in bed with at least one neurologist at his or her bedside. Before starting the test, the subjects were informed of testing details to alleviate anxiety. In addition, personnel maintained a neutral appearance and avoided talking to the subjects for the duration of the test. Studies were approved by the ethics committee of Xuanwu Hospital and were performed in a temperature-controlled laboratory (24°C to 26°C).
Induction of RIPC
RIPC was induced by inflating a 12-cm-wide BP cuff placed around the upper portion of the subject's nondominant arm for five cycles. Each cycle consisted of a 5-min period of 200 mmHg inflation with 5 min of reperfusion as previously described (2,20).
Assessment of Vital Signs
BP and HR were continuously monitored by a multiparameter electrocardiac monitor (Dinamap Pro 1000; General Electric Company, Rancho Cordova, CA, USA). BP was measured on the dominant arm five times throughout each cycle: 1) baseline, 2) during limb ischemia, 3) initiation of reperfusion, 4) immediately preceding subsequent ischemic cycle, and 5) 30 min after RIPC. HR was measured every minute. The same equipment was used for each participant to reduce experimental error.
Assessment of Ischemic Arm Pain
A visual analog scale was used to assess a subject's pain in his or her ischemic arm. The visual analog scale consists of a straight line with numbers ranging from 0 (no pain) to 10 (the worst pain imaginable) (Fig. 1). Subjects were asked to indicate their perception of arm pain by marking a point along the scale.
The visual analog scale. The number 0 represents no pain, while number 10 represents the most pain imaginable.
Assessment of Muscle Oxygenation of the Ischemic Arm and Brain Tissue
During RIPC, changes in the muscle oxygenation of the ischemic tissue were recorded by noninvasive near-infrared spectroscopy (NIRS; provided by the Dept. of Biomedical Engineering, Tsinghua University, China). Measuring probes were placed both on the skin of the brachioradialis muscle and the left prefrontal to reflect the extent of ischemia. The tissue oxygenation index (TOI) of the arm tissue was measured every minute. The TOI of brain tissue was recorded at the baseline and again 30 min following completion.
Assessment of the Cerebral Hemodynamic Changes
The mean flow velocity (MFV) in the bilateral MCA was used to detect cerebral hemodynamics. TCD (1.6 MHz EME-TC8080; Nicolet, Hamburg, Germany) was used to continuously monitor the MFV change in the bilateral MCA during RIPC. With the subject in a supine position, bilateral transducers were held in place with an adjustable head frame (Spencer Technologies, Redmond, WA, USA) on the temporal window during the TCD evaluation using search and fixation techniques (30). The BP of the anterior medialis and the pulse rate were noninvasively measured (Dinamap Pro 1000). MFV of the MCA was recorded between a depth of 50 and 60 mm at the baseline, during limb ischemia, at the initiation of reperfusion, immediately preceding the subsequent ischemic cycle, and 30 min after RIPC. The percent variation rates (VR) of the MCA MFV were calculated by the following equation: VR (%) = MFV at one time point/baseline MFV × 100%. The TCD evaluation and the subsequent interpretation of the data were done by an experienced technician.
Calculations and Statistical Analysis
All data were expressed as the mean ± SD and analyzed through SPSS 16.0 (IBM, Armonk, NY, USA). Continuous variables were compared by paired t-test. In all cases, a value of p < 0.05 was considered statistically significant. Statistical differences were analyzed by oneway ANOVA using the SNK test for post hoc comparisons after assessment of normality of the data distribution.
Results
Effect of RIPC on Blood Pressure and Heart Rate
The volunteers and patients were treated with brief repetitive bilateral arm IPC for five cycles (31). BP and HR were recorded five times during each cycle [(baseline), beginning of ischemia (I0), after 5 min of ischemia (I5), beginning of reperfusion (R0), and after 5 min of reperfusion (R5), and again 30 min after test completion (R30)]. All subjects tolerated the experiment without any complications. In healthy volunteers, the mean value of systolic BP, diastolic BP, and HR fluctuated from 120.3 to 128.0 mmHg, 67.4 to 76.7 mmHg, and 65.8 to 84.2 bpm, respectively. After undergoing RIPC, there was a significant reduction in diastolic BP (baseline, 73.4 ± 7.6 mmHg vs. R30, 68.3 ± 8.2 mmHg; p = 0.031, paired t-test; n = 24) and HR (baseline, 73.5 ± 8.3 bpm vs. R30, 68.4 ± 9.1 bpm; p = 0.027, paired t-test; n = 24) between baseline and 30 min after test completion, but no significant effect on systolic BP (baseline, 125.3 ± 11.7 mmHg vs. R30, 121.2 ± 14.1 mmHg; p = 0.162, paired t-test; n = 24) (Fig. 2A, B).
In patients, mean values of systolic BP, diastolic BP, and HR fluctuated from 137.5 to 152.6 mmHg, 84.3 to 90.4 mmHg, and 71.8 to 77.3 bpm, respectively. Comparing baseline and 30-min post-test completion, there was no significant effect of RIPC on diastolic BP, systolic BP, or HR. Diastolic BP (baseline, 87.6 ± 7.4 mmHg vs. R30, 86.2 ± 8.7 mmHg; p = 0.652, paired t-test; n = 10), systolic BP (baseline, 144.5 ± 10.6 mmHg vs. R30, 142.9 ± 15.2 mmHg; p = 0.431, paired t-test; n = 10), and HR (baseline, 74.7 ± 9.5 bpm vs. R30, 76.2 ± 8.4 bpm; p = 0.269, paired t-test; n = 10) values are depicted in Figure 2C and D.
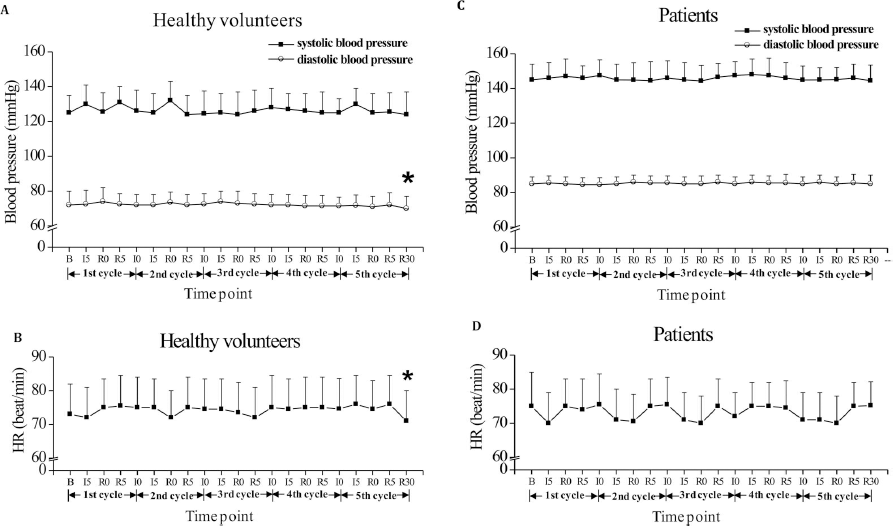
The effect of remote limb ischemic preconditioning (RIPC) on blood pressure (BP) and heart rate (HR) in healthy volunteers and in patients with middle cerebral artery (MCA) stenosis. (A) BP in healthy volunteers; (B) HR in healthy volunteers; (C) BP in patients; (D) HR in patients. B represents the time prior to RIPC; I0 represents the beginning of ischemia; I5 represents 5 min of ischemia; RO represents the beginning of reperfusion; R5 represents 5 min of reperfusion; R30 represents 30 min after completion. Healthy volunteers (n = 24) and patients (n = 10); *p < 0.05, R30 versus baseline (paired t-test).
Effect of RIPC on Tissue Oxygenation Index
The TOI of the ischemic forearm was continuously detected before, during, and 30 min after test completion. During ischemia within each cycle, the TOI of the ischemic forearm in all subjects decreased steadily until reperfusion, when it rapidly transcended baseline values, as indicated in Figure 3. The TOI values nearly returned to the baseline prior to each successive cycle (p > 0.05, TOI of the first minute in every cycle vs. that of the 10th minute, paired t-test) (Fig. 3). There was no significant difference between brain tissue oxygenation before and after RIPC in both healthy volunteers (baseline, 59.38 ± 13.67% vs. R30, 58.96 ± 15.02%, p = 0.352, n = 24) and patients (baseline, 57.64 ± 14.82% vs. R30, 58.21 ± 12.49%, p = 0.213, n = 10) (Fig. 4).
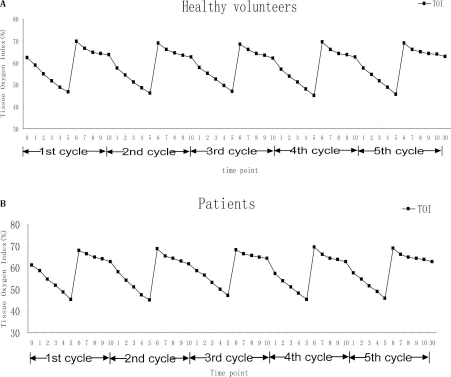
The effect of RIPC on the tissue oxygenation index (TOI) of the ischemic forearm in healthy volunteers (n = 24) and patients (n = 10). During every cycle, the TOI decreased to a low level at the end of ischemia, overshot when reperfusion began, and then decreased to the baseline at the end of reperfusion. Numbers 0–10 represent every minute in five cycles. Number 30 represents 30 min after completion.

The effect of RIPC on the TOI of brain tissue in all subjects. No significant difference was observed between baseline and R30 measurements (in healthy volunteers, baseline, 59.38 ± 13.67% vs. R30, 58.96 ± 15.02%, p = 0.352, n = 24; in patients, baseline, 57; 64 ± 14.82% vs. R30, 58.21 ± 12.49%, p = 0.213, n = 10). R30 represents 30 min after completion.
Effect of RIPC on Ischemic Arm Pain
For all subjects, ischemic arm pain gradually increased with each cycle's progression, with the maximum level of pain present toward the end of ischemia. We evaluated how pain perception changed with ischemic tolerance by comparing peak pain levels within each cycle. The greatest level of pain was observed in the second cycle (second cycle, 5.16 ± 1.61 vs. first cycle, 5.06 ± 1.54; p = 0.638, one-way ANOVA; n = 34), with a decreased level of pain in the fourth and fifth cycles (fourth cycle, 4.67 ± 1.53 vs. first cycle; p = 0.012; fifth cycle, 4.08 ± 1.87 vs. first cycle; p = 0.001; one-way ANOVA; n = 34) (Fig. 5).

The effect of RIPC on pain in the ischemic arm in all subjects. The pain gradually increased in the ischemic arm over the course of each cycle. The highest pain levels experienced during the fourth and fifth cycles were significantly lower than that in the first one (the fourth cycle, 4.67 ± 1.53 vs. the first cycle; p = 0.012; the fifth cycle, 4.08 ± 1.87 vs. the first cycle; p = 0.001; one-way ANOVA; n = 34). *p < 0.05, **p < 0.01, versus the first cycle (one-way ANOVA).
Effect of RIPC on Mean Flow Velocity of the Middle Cerebral Arteries
There was no definitive trend of MFV VRs (Fig. 6A, B). For healthy volunteers, the ranges of MFV VR in the left and right MCA were 80.11–118.81% and 80.41–120.18%, respectively. There were no differences in the mean values of MFV VR between inflation and deflation in each vessel (paired t-test, p > 0.05, n = 24) (Fig. 7A, B). For patients with MCA stenosis, the ranges of MFV VR in the stenotic MCA and the contralateral MCA were 84.75–124.39% and 86.67–131.41%, respectively. They also showed no differences in MFV VR between inflation and deflation (paired t-test, p > 0.05, n = 10) (Fig. 7C, D).
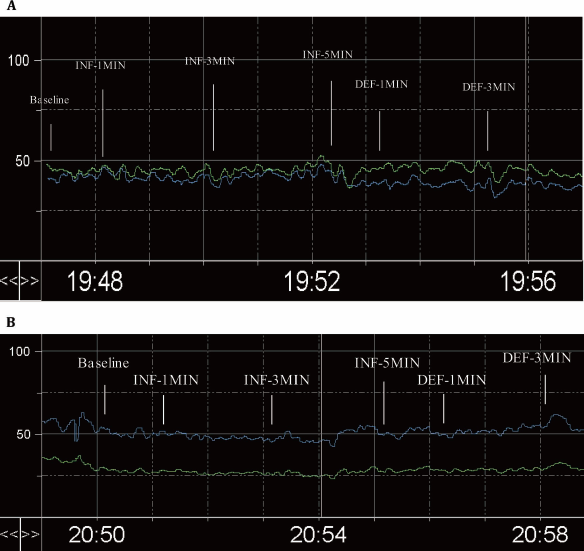
The trend window of mean flow velocity (MFV) in one healthy volunteer and in one patient with left MCA stenosis during the entire process. The green and blue lines represent the MFV of left and right MCA, respectively. (A, healthy volunteer; B, patient; INF, inflation; DEF, deflation).
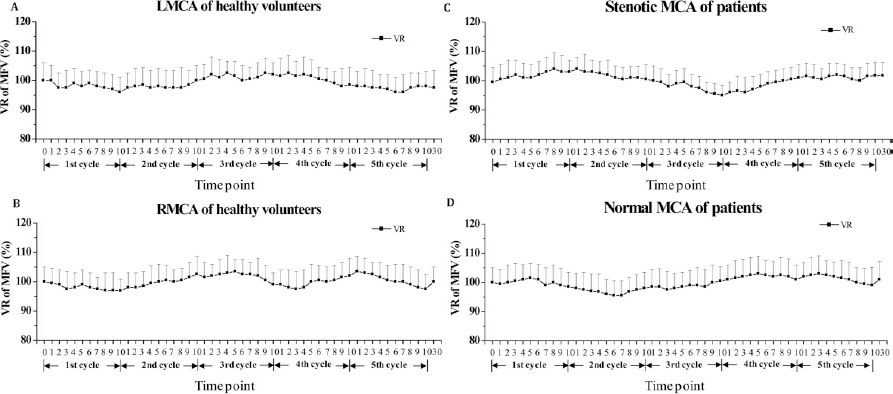
The MFV variation rates (VRs) of left MCA and right MCA in healthy volunteers and in patients with MCA stenosis. (A) LMCA of healthy volunteers; (B) RMCA of healthy volunteers; (C) stenotic MCA of patients; (D) normal MCA of patients. Numbers 0-10 represent every minute in five cycles. Number 30 represents 30 min after completion.
Discussion
Within the last 20 years, we have seen the therapeutic use of brief ischemic episodes in reducing tissue ischemia–reperfusion injuries following prolonged ischemia (38). Unfortunately, vital organs, such as the heart and brain, have not benefited from IPC in clinical practice. Regardless, because of RIPC's powerful innate mechanism of multiorgan protection, we believe that it is close to becoming a standard clinical technique. Several trials have reported reductions in myocardial injury when RIPC is used as an adjunct to major cardiac or vascular surgery (2,19). Botker et al. demonstrated that RIPC use before hospital admission increases myocardial salvage and has a favorable safety profile in patients with suspected first acute myocardial infarction (2).
Because neurons are very sensitive to hypoxia or ischemia, only a few clinical reports have assessed the preconditioning potential of the brain. Koch et al. was particularly concerned if patients with a subarachnoid hemorrhage would be able to tolerate repetitive and longer limb ischemia times safely. In their study, subjects were monitored for cerebral vasospasms and delayed cerebral ischemia (25). It is well known that ischemia/hypoxia preconditioning depends on sublethal ischemia/hypoxia exposure. Thus, the strength and duration of RIPC should play an important role in the outcome of neuroprotection. BP, HR, MFV, TOI, and pain were the measured vital signs to track RIPC safety and feasibility. The change in vital signs may reflect ischemic tolerance. Our study included healthy adults and patients with unilateral MCA stenosis, with strict monitoring of these vital signs. In this study, the subjects' BP and HR fluctuated within the normal range. Additionally, subjects did not complain of dizziness, chest discomfort, or other cardiovascular symptoms. Thirty minutes following five cycles of limb ischemia, there was a decrease in diastolic BP and HR in healthy volunteers. This phenomenon may be explained by RIPC-induced upregulation of nitric oxide (NO) (20,45,47), which is known to cause both potent vasodilation and neurotransmission derived from perivascular nerves (36). However, there were no changes in patients with unilateral MCA stenosis. The differences may be due to the variations of vascular endothelial function between healthy volunteers and patients (39). However, the details still need to be further investigated.
NIRS is a new rising technique to noninvasively monitor tissue oxygenation. The TOI was continuously monitored to delineate the regular change of tissue oxygenation in ischemic conditions. Both the arm and brain TOI did not change. Several physiological trials have suggested that exercise (35), visual stimuli (37), cessation of breath, selected vasoactive drugs, and BP changes (29) could influence the MFV of MCA or posterior cerebral arteries in healthy volunteers by as much as 20-30%. In contrast, RIPC has a minimal influence on MFV, even in patients with severe MCA stenosis. These findings further suggest that RIPC is a safe procedure for patients with cerebral vascular stenosis.
Although the mechanism is unclear, we found increased pain threshold after RIPC in both volunteers and patients. The optimal duration of limb ischemia remains uncertain (25). Several cardiac and neurological clinical studies have examined 5-min cycles of arm ischemia (12,16,25,40,42), whereas the duration of limb ischemia in laboratory animals has typically exceeded 10 min (1,5,27,41,44). While the specific mechanism of RIPC warrants further investigation, a number of studies have suggested that some of the underlying mechanistic pathways (such as a neural pathway, humoral pathway, or systemic response) and signal transduction cascades (e.g., adenosine, opioids, or NO) activated with remotely preconditioned target tissues may be similar to those recruited in the setting of local IPC (13). The intensity of the limb ischemia stimulation plays a key role in protecting the heart and brain against ischemia (8). Owing to increased pain, clinical studies currently cannot lengthen limb ischemia time. However, as we saw a change in the pain threshold after the third cycle of ischemia in our study, it may be possible to take advantage of the observed pain tolerance and eventually lengthen limb ischemic time.
Recent studies have implicated the role of stem cells in RIPC. Exposure of stem cells to paradigms of RIPC potentiates the therapeutic effects of stem cells in vitro (9,15,48) and in vivo (17,26,46). Such IPC stem cells appear to afford improved efficacy for stem cell-based regenerative medicine (32,46), including cardiac repair (3,45), blunting of cellular senescence (26), and stroke (49), possibly via the angiogenic stromal-derived factor 1/chemokine C-X-C motif receptor 4 (SDF-1/CXCR4) pathway (7,17). Investigations of RIPC-mediated modulation of stem cells will likely lead to novel treatment strategies for regenerative medicine.
Conclusions
RIPC provides a powerful defense against ischemic injury. Our data demonstrate the safety of repetitive limb ischemia in patients with unilateral MCA compared to healthy volunteers. Additionally, RIPC may decrease diastolic BP and HR within 30 min of reperfusion in healthy volunteers. Moreover, subjects tolerated ischemic arm pain well, especially in the fourth and fifth cycle, suggesting that RIPC elevates the human pain threshold. As this was a pilot study with a small sample size, we hope that the effects and safety of RIPC will be confirmed by further studies. Our interest in stem cell therapy will be considered as we advance RIPC for clinical applications of regenerative medicine.
Footnotes
Acknowledgments
We thank Guowei Lu from Capital Medical University, Yulan Wang from the Central Lab, Xuanwu Hospital, Capital Medical University, Youqin Liu from the Healthy Physical Examination Center, Xuanwu Hospital, Capital Medical University, and Haishu Ding from the Department Biomedical Engineering, Tsinghua University for their earnest help in the study conduct. We also thank Stephanny Reyes, Daniela Aguirre, and Diego Lozano of the Department of Neurosurgery and Brain Repair of the University of South Florida for their technical assistance in finalizing the manuscript. This project was supported by the National Science Foundation for Distinguished Young Scholars of China (No. 81325007) and the National Natural Science Foundation of China (No. 81160244). The manuscript has been approved by all authors for publication. The authors declare no conflicts of interest.