
Abstract
Cell-based therapies, which all involve processes for procurement and reimplantation of living cells, currently rely upon expensive, inconsistent, and even toxic enzyme digestion processes. A prime example is the preparation of isolated pancreatic islets for the treatment of type 1 diabetes by transplantation. To avoid the inherent pitfalls of these enzymatic methods, we have conceptualized an alternative approach based on the hypothesis that cryobiological techniques can be used for differential freeze destruction of the pancreas (Px) to release islets that are selectively cryopreserved in situ. Pancreata were procured from juvenile pigs using approved procedures. The concept of cryoisolation is based on differential processing of the pancreas in five stages: 1) infiltrating islets in situ preferentially with a cryoprotectant (CPA) cocktail via antegrade perfusion of the major arteries; 2) retrograde ductal infusion of water to distend the acinar; 3) freezing the entire Px solid to lt; −160°C for storage in liquid nitrogen; 4) mechanically crushing and pulverizing the frozen Px into small fragments; 5) thawing the frozen fragments, filtering, and washing to remove the CPA. Finally, the filtered effluent (cryoisolate) was stained with dithizone for identification of intact islets and with Syto 13/PI for fluorescence viability testing and glucose-stimulated insulin release assessment. As predicted, the cryoisolate contained small fragments of residual tissue comprising an amorphous mass of acinar tissue with largely intact and viable (>90%) embedded islets. Islets were typically larger (range 50–500 μm diameter) than their counterparts isolated from juvenile pigs using conventional enzyme digestion techniques. Functionally, the islets from replicate cryoisolates responded to a glucose challenge with a mean stimulation index = 3.3 ± 0.7. An enzyme-free method of islet isolation relying on in situ cryopreservation of islets with simultaneous freeze destruction of acinar tissue is feasible and proposed as a new and novel method that avoids the problems associated with conventional collagenase digestion methods.
Introduction
All cell-based therapies require technologies for harvesting, expanding, modifying, and reimplantation of cells. Processes for preparing the therapeutic product are critical to its stability and potency but may be inherently injurious to the component cells. For example, the widely practiced technique of collagenase digestion of tissues to obtain isolated cells is fraught with detrimental side effects and other associated problems. A primary example is the transplantation of isolated pancreatic islets of Langerhans for the potential amelioration of type 1 diabetes. Inherent to the process of harvesting is the requirement for a controlled separation of the desired therapeutic cells from other unwanted cells in the donor tissue. This widely practiced procedure has recognized pitfalls due principally to the difficulty of controlling the digestive process to maximize the quantity of viable cells, while minimizing the harsh and potentially toxic conditions caused by the enzyme-based process, leading to evitable loss of valuable cells. Furthermore, while this process relies upon the purest and most expensive forms of enzymes, it is subject to batch variations and frustrating inconsistent results.
Collagenase, a crude byproduct of Clostridium histolyticum fermentation is heterogeneous, contains a large number of different enzymes, cellular debris, and high levels of endotoxins. These characteristics result in variable enzymatic activity of collagenase batches and reduced reproducibility in the islet isolation procedures (3,6,13,18,60). Lot-to-lot variability of commercial collagenases has been a major hindrance to the development of consistent techniques for islet isolation. Even the highly purified collagenase blends used in clinical islet isolations have recently been reported to suffer from significant interlot differences in digestion time, prepurification islet counts, percent recovery, viability, and insulin secretory function indices (63). Moreover, deterioration in enzyme activity and concomitant decline in isolation outcomes was noted using a single enzyme lot, even when the enzyme blends were used within the expiration date specified by the manufacturer (63). Clearly, an enzyme-free method of isolating pancreatic islets would offer significant advantages for a more consistent, less expensive method of islet isolation. To this end, this study evaluates an original new approach based upon cryobiological principles and the concept of differential freezing to destroy the exocrine component of the pancreas during simultaneous in situ cryopreservation of the islets.
Cryopreservation is a complex process of coupled heat and mass transfer, generally executed under non-equilibrium conditions. Control of the thermodynamic and osmotic processes during cooling and heating are fundamental challenges that dictate whether the biological system is protected or injured during freezing (19,39,40). The properties of cold can be harnessed for either the preservation and storage of cells and tissues (cryopreservation) or destruction of undesirable tissue such as tumors (cryosurgery) by carefully selecting and optimizing the conditions of freezing and thawing (2,12,64). Both modalities are highly significant in modern day medicine for a wide variety of clinical and therapeutic applications. The fundamental principle underlying the concept of cryoisolation is that the effect of ice in a biological system depends critically upon the amount and location of the ice (58). Cryopreservation and cryosurgical technologies allow these processes to be controlled to maximize the effects of protection or cryoinjury, respectively.
Cryopreservation of Pancreatic Islets
Techniques for cryopreservation of isolated pancreatic islets have been available in the literature for over 30 years, thus providing the expectation that viable islets could be preserved during the freeze destruction of the pancreas. Our own contributions in this field established the interaction between a variety of key factors that, as cryobiologists, we knew were important for survival of cryopreserved islets. In particular, we discovered that dimethyl sulfoxide (DMSO) was a better cryoprotectant for islets than glycerol and that the interaction of cooling and warming rates was dependent upon the extent of permeation of DMSO before freezing for highest survival (50,51,54,55). In 1994, Rajotte et al. reviewed the status of islet cryopreservation outlining the procedural differences needed for different species including human islets (32). More recently, in collaboration with Rajotte and Lakey with the Edmonton group, we showed that postcryopreservation survival of islets can be improved using “intracellular-type” preservation media as the vehicle solution for the cryoprotectant DMSO (17). Conceptually, the application of these cryobiological principles was to design a process that provided in situ cryopreservation of the islets while simultaneously destroying the unwanted exocrine portion of the gland as described below.
The Cryoisolation Concept
With reference to the simplified schematic in Figure 1, the conceptual baseline cryoisolation can be described as a five-step process (57).

Schematic diagram of pancreas pretreatment for the cryoisolation concept of islet isolation. (A) Antegrade infusion of islets in situ with cryoprotective agent (CPA) solution via a vascular access for protection of the islets during freezing. (B) Retrograde ductal infusion of water (or isotonic saline) to maximize freeze destruction of the acinar tissue. In the absence of CPA, intracellular ice crystallization (depicted by *) in all acini and duct cells coupled with extracellular freezing in the connective tissue will maximize tissue disruption and cell lysis.
Step #1 (Fig. 1A): Vascular Infusion of Islets In Situ with Cryoprotective Agent (CPA)
Antegrade perfusion of the celiac and superior mesenteric arteries with a CPA should be performed under controlled conditions of temperature and pressure. Perfusion should be maintained sufficiently long to allow equilibration of the islets with a permeating CPA but not long enough to avoid CPA equilibration with the entire gland. The rationale for this step is to deliver sufficient CPA to the islets to protect them against freezing injury during subsequent freezing of the pancreas.
Step #2 (Fig. 1B): Ductal Infusion of Water (or Isotonic Saline)
Retrograde infusion of water into the pancreatic duct should be initiated immediately upon completion of step #1. This process is continued until the gland is visibly distended. The rationale for this step is to impregnate the exocrine tissue with water to facilitate extensive destructive ice formation in the noncryoprotected tissue upon freezing.
Step #3: Freezing of the Pancreas
Upon completion of steps #1 and #2, the entire pancreas will be cooled to subzero temperatures until frozen solid. The rationale for this step is to maximize ice formation in the unprotected exocrine gland to facilitate tissue disruption for subsequent disintegration of the gland, in order to release the cryoprotected islets.
Step #4: Warming and Physical Disruption of the Pancreas
Conceptually, the macrostructure of the pancreas should be disrupted either while still frozen or during thawing, whichever provides the most efficient disintegration of the gland.
Step #5: Separation and Purification of the Islets
Islet tissue will be separated and purified from the unwanted cryolysate using a combination of techniques including filtration, density gradient separation, and/or tissue culture.
Materials and Methods
Pancreas Procurement
Pancreata were obtained from small farm pigs (Domestic Yorkshire, male, 25 to 32 kg, Hambone Farms, Orangeburg, SC, USA) using the previously published technique we have used extensively in studies to develop methods of pancreas preservation (46,48). All animal care and handling complied with policies and approval of the Institutional Animal Care and Use Committee (IACUC) at the Medical University of South Carolina (Charleston, SC, USA), where the organ procurements were carried out.
In brief, following in situ cold flushing with organ preservation solution [Lactated Ringer's solution (Baxter, Deerfield, IL, USA) and Unisol™ (Unisol-I; ORS, Itasca, IL, USA)] (42,43), the pancreas was removed from the donor with a duodenal segment attached around the pancreas head to protect the superior and inferior pancreaticoduodenal arteries. During perfusion preparations, the pancreas was maintained cold on ice. The common bile duct and pancreatic duct openings are part of the duodenum segment. The splenic vein and artery on the spleen side were ligated prior to spleen detachment. A 5- to 7-cm-long aortic segment was left attached to the pancreas for subsequent organ cannulation for whole pancreas perfusion. The segment included the openings of both superior mesenteric artery (SMA) and celiac trunk (CT) vessels. All exposed arterial branches on the margin of gastroduodenal and hepatic sides of the pancreas were meticulously identified and ligated to ensure uniform perfusion throughout the gland and allow the effluent to emerge only from the portal vein. The pancreatic duct was cannulated using its opening on the duodenum side to preserve all early duct branches and to ensure subsequent good organ distension. For whole pancreas perfusion, a seal ring cannula (ORS) was placed on the aortic patch formed by the longitudinal sectioning of the aortic segment inclusive of SMA and CT openings, without interfering with the two vessel lumens. This cannulation provided a sealed flow link between the pancreas and perfusion system. The aortic patch cannula was attached to the pump infusion port as previously described in detail (46,48).
Cryoisolation Processing
The conceptual technique outlined above embodies a significant number of variables for which we had to select a specific set of values, in order to test feasibility and develop preliminary data. In some cases, key variables such as the choice of CPA and its concentration were selected based upon relevant information in the literature, including our own prior work on islet cryopreservation and pancreas perfusion (9,10,17,24,51,52,54–56). Other variables, such as the cooling and warming conditions, were selected initially based on practicality and experience-based intuition. While space limitations do not permit us to present and discuss the complete set of variables and the selected corresponding values, we can report that proof-of-concept data have been developed using the porcine pancreas as the tissue model using the baseline conditions outlined in Table 1.
Conditions Selected for Trial Feasibility Tests of Cryoisolation of Porcine Pancreatic Islets

CPA, cryoprotectant; DMSO, dimethyl sulfoxide; CT/SMA, celiac trunk/superior mesenteric artery.
Baseline Process
The baseline process used to test feasibility of the cryoisolation concept comprised five steps (57).
Process Step #1: Vascular Perfusion to Infiltrate Islets In Situ with Cryoprotectant
The juvenile porcine pancreases were prepared for perfusion using the techniques we have published recently (46–48). In brief, antegrade perfusion of the celiac and superior mesenteric arteries was achieved using an aortic patch and our proprietary “seal-ring” cannula. During dissection, a thermocouple was advanced to the center of the gland via a portal vein access and sutured in place. The pancreatic duct was also cannulated as previously described. As illustrated in Figure 2A, perfusion with a cryoprotective solution was performed under controlled conditions of temperature (6–8°C) and flow rate (15–17 ml/min) to preferentially equilibrate the islets within the gland. Perfusion was maintained sufficiently long enough to allow equilibration of the islets with DMSO (Sigma-Aldrich, St Louis, MO, USA) as a permeating CPA but not the whole gland. Thirty minutes of perfusion with 2 M DMSO in Unisol (UHK-CV) solution (5,53) on ice was selected for this feasibility study based on previous studies (17,33,51). The rationale for this step is to deliver sufficient CPA to the islets to protect them against freezing injury during subsequent freezing of the pancreas.

Panel of photographs illustrating the principal steps of processing in the preliminary cryoisolation technique. (A) Antegrade vascular perfusion of the excised pancreas with cold cryoprotectant solution for preferential infiltration of islets in situ. (B) Retrograde ductal infusion of water (or isotonic saline) on ice via the cannulated pancreatic duct to impregnate the exocrine tissue with water for maximum formation of destructive ice during subsequent cooling. (C–E) Progressive cooling of the gland on a metal tray suspended on the surface of boiling liquid nitrogen to freeze the pancreas to −160°C. (F, G) Mechanical crushing and pulverizing the frozen pancreas to reduce it to “frozen gravel.” (H, I) Pulse grinding of the crushed frozen pancreatic gravel in an electric ice grinder/blender. (J) Thawing of pancreatic fragments by addition of cold medium to dilute out the CPA and further fragment the preparation by pulse blending. (K) Initial purification of the cryoisolate by decanting through a stainless steel sieve to remove fibrous debris. (L) Washing and sedimentation of the cryoisolate by centrifugation.
Process Step #2: Retrograde Ductal Infusion of Water
At the conclusion of the cryoprotectant infusion in step #1, the pancreas was immediately infused with ice-cold deionized water (120 ml) via retrograde injection through the previously cannulated pancreatic duct (Fig. 2B). This process is equivalent, in volume and technique, to the pancreatic distension with enzyme solution during the conventional collagenase preparation and isolation of islets, and it is designed to impregnate the exocrine tissue with water that will form copious amounts of destructive ice during freezing.
Process Step #3: Freezing of the Pancreas
Step #3 involved cooling the pancreas to subzero temperatures to promote freezing by surface conduction with the pancreas placed on a metal tray floating on the surface of boiling liquid nitrogen (-196°C). Figure 2C–E illustrates the progressive freezing of a pancreas in a metal tray that cooled the gland at −11°C/min to −160°C. The frozen pancreas was sealed in a plastic bag and stored in the vapor phase of a liquid nitrogen cryostorage container.
Process Step #4: Mechanical Disruption of the Frozen Gland
In step #4, the frozen pancreas was removed from storage and mechanically crushed and pulverized into small fragments. As shown in Figure 2F, the pancreas was initially broken into pieces by fracturing with a hammer and chisel. In this way, the frozen gland could be divided into pieces of a desired size and also allowed separation of the unwanted duodenum and recovery of the embedded thermocouple for reuse in another preparation. Further pulverization of the frozen pieces could be accomplished in a variety of ways, but crushing by mechanical compression (hammering in a containment bag) followed by 10 × 1-s pulse grinding in an ice grinder proved effective in this feasibility study (Fig. 2G, H).
Process Step #5: Thawing to Generate the Cryoisolate Product
Thawing of the pancreatic fragments commenced during the mechanical fragmentation process in which the product was exposed to ambient air (Fig. 2I). The thawing and fragmentation process was accelerated by adding cold medium [M199 with trypsin inhibitor (0.1 μg/ml; Worthington Biochemical, Lakewood, NJ, USA)] directly to the tissue fragments in the ice grinder reservoir and blending using 13 × 1-s pulses (Fig. 2J).
Process Step #6: Washing and Sedimentation of Cryoisolate
Finally, the preparation was decanted through a stainless steel sieve (Walmart tea strainer, Bentonville, AR, USA) (Fig. 2K) and the filtered effluent (cryoisolate) collected for washing twice by centrifugation (Former Scientific, Marietta, OH, USA; Model 5682) in 500-ml conical centrifuge tubes (Corning, Fisher Scientific, Waltham, MA, USA) using 1,200 rpm/300 × g for 3 min in cold Hank's buffered salt solution [HBSS + 5% fetal calf serum (FCS) + trypsin inhibitor (Sigma-Aldrich)] (Fig. 2L). The final cryoisolate pellet was resuspended in medium from which samples were taken for microscopic examination, for viability assessment and insulin release assay.
Cryoisolate Analysis
The principal method of evaluation was light microscopy after staining with dithizone (Sigma-Aldrich) to specifically identify islets in the final preparation using an Olympus IX70 inverted microscope. Samples were also taken for viability assessment by fluorescence staining with Syto-13/propidium iodide (PI) (Invitrogen-Molecular Probes, Eugene, OR, USA) (1) on an Olympus BX41 microscope (Center Valley, PA, USA) equipped with appropriate filters for 488 nm absorption and 509 nm emission fluorescein isothiocyanate (FITC) fluorescence. The islet sizes were determined using ImagePro (Rockville, MD, USA) and Lumenera Infinity Analyze v.5.0.2 (Ottawa, ON, Canada).
Functional evaluation of the cryoisolated islets was undertaken using the static glucose-stimulated insulin secretion assay in accordance with standardized methods previously published and used extensively for in vitro evaluation of isolated islets (9).
Although several trial runs to evaluate several variables in the process were undertaken to develop a basic protocol for feasibility testing, three replicate preparations were evaluated using the baseline process outlined above and are reported here.
Results
Morphological Characterization of Cryoisolate
Dithizone-Staining for Identification of Islets
As illustrated in Figures 3, 4, and 5, phase-contrast microscopy of samples of cryoisolate showed that the preparations comprised fragments of tissue, many of which contained one or several embedded islets readily identified by dark red dithizone staining. Figure 3A–D illustrates the appearance of the cryoisolate fragments comprising an amorphous mass with clearly distinguishable dithizone-stained islets of varying shapes and sizes. The shell of nonstained material surrounding the islets was presumed to be the remnants of acinar tissue destroyed by freezing. The degree of cleavage and separation of the dithizone-positive islets from the exocrine tissue was variable, with the majority of islets remaining embedded in the unstained material (Fig. 3). Figure 3D shows intact islets embedded in residual exocrine tissue with a vascular or ductal structure clearly apparent. In contrast, some discrete islets were more cleanly separated with very little residual exocrine or ductal tissue (Fig. 3B). In all cases, the acinar tissue appeared unstructured and amorphous, consistent with generalized destruction and with an abundance of zymogen granules dispersed throughout the acellular debris (Fig. 3B).

Dithizone staining of cryoisolate fragments showing the presence of multiple stained islets embedded in an amorphous shell of freeze-destroyed acinar tissue. The degree of cleavage and separation of the dithizone-positive islets from the exocrine tissue was variable with the majority of islets remaining embedded in the unstained material (A, C, and D). (D) Intact islets embedded in residual exocrine tissue with a vascular or ductal structure clearly apparent. In contrast, some discrete islets were more cleanly separated with very little residual exocrine or ductal tissue (B). In all cases, the acinar tissue appeared unstructured and amorphous, consistent with generalized destruction and with an abundance of zymogen granules dispersed throughout the acellular debris (B). (B and D) Reproduced from Taylor and Baicu (45) with the permission of Elsevier, the publishers of Transplantation Proceedings.
Islet Size
Islets identified by dithizone staining showed a wide variety of dimensions ranging from <50 μm to >500 μm diameter (Figs. 4 and 5). Figure 4 illustrates the identification of many larger islets that exceeded the dimensions typically observed in samples prepared by conventional enzyme digestion of juvenile porcine pancreata (Fig. 4C) (48).

Islet size. Dithizone staining of cryoisolate samples illustrating the typically larger islets structures (A, B, D), observed in comparison with the preparations from conventional collagenase digestion of juvenile porcine pancreas (C). Image analysis software (ImagePro and Luminera Infinity Analyze v.5.0.2) was used to generate accurate calibrated sizing as indicated by the scale bars. (D) Reproduced from Taylor and Baicu (45) with the permission of Elsevier, the publishers of Transplantation Proceedings.
Viability and Function of Cryoisolate Tissue
Figure 5A and B illustrates that samples of cryoisolate stained with the fluorescent probes Syto-13/PI for assessment of membrane integrity showed a clear demarcation of the green fluorescent viable cells (presumed pancreatic islets) surrounded by a shell of red fluorescent dead material. Figure 5C and D also shows the corresponding phase-contrast images of the same fluorescent islets illustrating the strong correlation between the phase boundary of the viable cells and the surrounding diffuse amorphous dead material that, apart from a few scattered isolated viable cells, stained almost exclusively with PI. The discrete embedded islets shown here are representative of the cryoisolated islets, which were generally greater than 90% viable by the Syto-13/PI assay.

Cryoisolated islets prepared from porcine pancreas after 8 months of storage at −135°C. Fluorescent micrographs of cryoisolate preparations stained with Syto-13/propidium iodide (PI) showing green fluorescent structures with >90% viability embedded in a shell of red fluorescent dead material (A, B). The corresponding phase-contrast micrographs of the same cryoisolate fragments show the phase boundary of the viable cells and the surrounding diffuse amorphous dead material (C, D). Intact dithizone-positive islets identified in cryoisolate fragments prepared from pancreata after 8 months of storage in the vapor phase of liquid nitrogen at −135°C (E, F). All micrographs are presented at the same magnification represented by the scale bar in (F).
The insulin secretory function of samples of the islets from replicate cryoisolations was determined by conventional static glucose stimulation assay and enzyme-linked immunosorbent assay (ELISA) insulin determination (49). The mean stimulation index relative to baseline was 3.3 ± 0.7 (n = 3), establishing the presence of insulin secretory cells within the isolates.
Discussion
In modern day medicine, cellular therapies, regenerative medicine, and tissue engineering all involve technologies for harvesting, expanding, modifying, and reimplanting live viable cells and tissues. A primary example that illustrates the idea behind this study is the transplantation of isolated pancreatic islets of Langerhans for the potential amelioration of type 1 (insulin dependent) diabetes (36). Inherent in the process of harvesting the donor cells is the requirement for controlled separation of the desired therapeutic cells from other unwanted cells in the donor tissue. Historical development of islet isolation methods have relied upon crude cutting of the tissue into fragments, which fails to separate the target cells from the unwanted cells. Today, the field of islet transplantation relies totally upon enzymatic digestion processes that destroy the extracellular matrix of the tissue releasing the entrapped islets for further processing and purification. This widely practiced procedure has recognized pitfalls due principally to the difficulty of controlling the digestive process to consistently yield an optimum quantity of viable cells. Moreover, the process is harsh and even toxic, causing some inevitable loss of valuable cells. Furthermore, the process relies upon the purest forms of the enzymes, which are very expensive and still subject to batch variations that have led to frustrating variability and inconsistency in attempts to optimize and standardize these processes (3,6,13,18,60,63).
Enzymatic Preparation of Isolated Islets
The entire field of islet research and transplantation is dependent upon enzymatic digestion of excised pancreata to generate isolated islets. The forgoing discussion illustrates the well-documented vagaries and variability that has inherently led to inconsistencies in the outcomes of islet isolation yields and functionality. Moreover, in 2007, the FDA and Roche Diagnostics (manufacturer of collagenase enzymes for islet isolation) independently warned users of the potential risk of bovine spongiform encephalopathy (BSE) due to the fact that bovine brain extracts are used in the feeder cultures of the Clostridium histiolyticum bacterium from which the collagenases are derived in commercial preparations (http://www.fda.gov/cber/rules/catruminant.htm). This led to a worldwide temporary hold on the use of the most widely used collagenase products pending both the development and evaluation of alternative sources of collagenase. The field of clinical islet transplantation and islet research has been set back for several years pending the resolution of these enzyme-related questions. Clearly, an enzyme-free method of isolating pancreatic islets would offer significant advantages for a more consistent, less expensive method of islet isolation (57).
Cryobiological Principles Applied to the In Situ Cryopreservation of Islets and Selective Destruction of Acinar Tissue
The process of simply freezing cells or tissues results in dead, nonfunctional materials unless steps are taken to avoid freezing injury (19,39,40). Cryopreservation is a complex process of coupled heat and mass transfer, invariably carried out under nonequilibrium conditions. During slow freezing, water is removed from cells and tissues as ice begins to form in the extracellular environment. The transformation of water into ice outside of the cell causes an osmotic imbalance that result in the exosmosis of water to the extracellular region, where it is frozen into ice. Water loss continues until temperatures are reached at which the diffusion of water across the membrane becomes negligible (20). The amount of water loss from the cell is dependent upon the cooling rate after the formation of extracellular ice. Slow cooling rates prolong the exosmosis of cellular water to the extracellular space and therefore produce greater cellular dehydration. Excessive dehydration leads to a series of cell injury mechanisms that are classified as “solution effects” that include exposure to increasingly toxic concentrations of electrolytes caused by removal of water from the liquid phase and membrane damage from excessive cell shrinkage. During rapid cooling, the period of water exosmosis is shortened, as membrane permeability to water quickly decreases with temperature. Water becomes trapped within the cell, and the cytoplasm begins to supercool as the resulting thermodynamic imbalance of water increases. Finally, the intracellular water equilibrates thermodynamically with the extracellular solution resulting in a phase change that transforms the intracellular water to ice. Widespread formation of intracellular ice in the cell has been uniformly associated with lethal cell injury (14,21). For most cell types, there exist optimal cooling rates that lead to maximum cell viability. These cooling rates provide sufficient cellular dehydration to prevent the formation of intracellular ice without causing excessive water loss that may lead to cell injury via “solution effects.” Warming cells from cryopreserved states is typically performed with maximal warming rates to prevent the recrystallization of ice from smaller ice crystals as the sample temperature is raised from cryogenic levels to the melting point of the solution. It has been established that recrystallization during rewarming is deleterious and results in lower cell viability, although the exact mechanisms of injury are not fully understood. However, it has been shown that viability is greater when cells are warmed rapidly through the conditions in which recrystallization occurs.
The use of cryoprotectants during freezing and thawing of biological materials has become established as an essential component for avoiding freezing injury. A wide variety of cryoprotectants have been identified, with DMSO being the most widely used. Interestingly, a comparison of chemicals with cryoprotectant properties reveals no common structural features. These chemicals are usually divided into two classes: 1) intracellular cryoprotectants with low molecular weights, which permeate into cells and 2) extracellular cryoprotectants with relatively high molecular weights (greater than or equal to sucrose, e.g., 342 Da), which do not penetrate cells (20). The primary mode of protection for permeating cryoprotectants is the displacement of intracellular water by the cryoprotectant. Regulated removal of intracellular water is essential to inhibiting the lethal formation of intracellular ice. Intracellular cryoprotectants, such as glycerol and DMSO at concentrations from 0.5 to 3.0 M, are effective in minimizing cell damage in many small biological systems frozen with slow cooling rates (39–41). Frozen tissues undergo extensive extracellular ice formation, even during procedures that result in otherwise excellent cell viability. The extent of freezing damage depends upon the amount of free water in the system and the ability of that water to crystallize during freezing. Parenthetically, we have developed techniques of ice-free cryopreservation that employ high concentrations of cryoprotective agents (>50%) to bring about amorphous, or vitreous, solidification that avoids ice formation, a process referred to as vitrification (37,44,58,59). In contrast, conditions in which the normal architecture of the tissue is destroyed by freezing will be promoted in the acinar tissue of the pancreas to bring about tissue disruption and disintegration. The conceptual plan is to couple this with strategic cryoprotection of the embedded islets to preserve their structure and function during the freezing process. In principle, this approach will allow the selective preservation of the islets during a process that will facilitate the disintegration of the rest of the pancreas for the ultimate separation and purification of the islets.
Cryopreservation of Pancreatic Islets
Effective techniques for cryopreservation of viable pancreatic islets have been available for several decades, and our own contributions to the literature in this field established the interaction between a variety of key factors that are important for survival of cryopreserved islets. Importantly, we showed that DMSO was a superior cryoprotectant for islets compared with glycerol and that the interaction of cooling and warming rates was dependent upon the extent of permeation of DMSO before freezing for highest survival (50,51,54,55). Development of the cryoisolation concept aims to take advantage of the current state of the art of islet cryopreservation with concomitant and selective destruction of acinar cells in the frozen pancreas to evaluate a new concept for islet isolation that could significantly reduce or even eradicate the dependency upon enzymatic digestion of the pancreas.
Initial Trials Using Preliminary Baseline Conditions: Proof of Concept
The conceptual technique outlined above embodies a number of variables for which we proposed a set of initial conditions outlined in Table 1, in order to undertake a preliminary trial attempt at implementing this new approach. Key variables, such as the choice of CPA and its concentration, were selected based upon relevant information in the literature, including our own prior work on islet cryopreservation and pancreas perfusion (9,10,17,24,51,52,54–56). Other variables, such as the cooling and warming conditions, were selected initially on the basis of practicality and experience-based intuition.
Physical Parameters
The initial trial runs carried out in the manner described above resulted in a cooling rate of 11°C/min and a final temperature in the frozen pancreas of ≤–160°C. The solid frozen gland was divided into two sections to test two different modes of pulverization and warming. In the first, the frozen piece containing the thermocouple was immersed directly into warm (30°C) tissue culture medium. This yielded a warming rate of 12°C/min, but macroscopic fracturing was not achieved. It was therefore concluded that this mode of warming is unlikely to produce the extensive thermal fracturing anticipated or necessary to shatter the tissue into small islet-containing fragments. Further work on this aspect of the approach will attempt to maximize and control thermomechanical stresses in frozen tissues to optimize the disruption phase (29). An alternative mode of pulverization involved mechanically crushing and fracturing the frozen tissue in two stages. The first was to physically split the frozen pancreas into small lumps and chips with a hammer and chisel to effectively reduce the frozen gland to pieces that could be loaded into an electric ice crusher. The second stage was to physically grind and chop the frozen tissue chips while immersed in cold (4–6°C) or room temperature medium. This also served to affect rapid warming and dilution of the cryoprotectant at the same time as mechanically pulverizing the tissue in the blender. The resulting cryoisolate was filtered and washed through a stainless steel mesh (tea strainer) to remove macroscopic and stringy debris. The filtered effluent was stained with dithizone, a widely used indicator for identifying islets and examined under the microscope for the presence of intact islets.
Characterization of the Cryoisolate
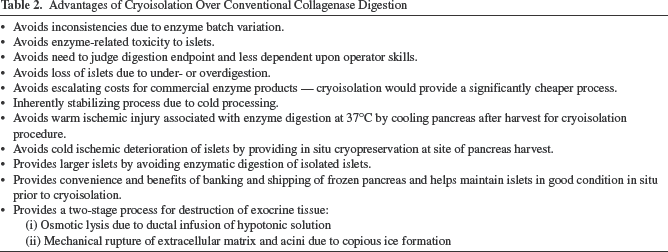
Various examples of the stained tissue in the cryoisolate are shown in this report. As predicted, the tissue was reduced to an amorphous mass in which clearly distinguishable islets were present. The degree of cleavage of the islets from the exocrine tissue was variable. In all cases, the acinar tissue appeared unstructured and amorphous, consistent with generalized destruction, with an abundance of zymogen granules dispersed throughout the acellular debris. The high abundance of zymogen granules observed in the islet preps of this initial cryoisolation trial is an excellent indication that our objective of selective acinar cell destruction was achieved. In contrast with conventional islet isolation, where lytic enzymes from damaged exocrine cells are present at the optimum temperature for their activity, processing in the cold was anticipated to attenuate detrimental enzymatic activity during islet purification. This significant technological advantage is included in a list of potential benefits and advantages summarized in Table 2 and discussed below.
Advantages of Cryoisolation Over Conventional Collagenase Digestion
Not all islets identified in the cryoisolate were completely intact. For example, the islet shown in Figure 4D has a diffuse or loose structure that could reflect osmotic shock due to direct immersion into isotonic medium during warming in this trial run. If so, this problem can readily be averted by employing the technique of osmotic buffering that is commonly used during CPA dilution in cryopreservation protocols (9,39). Future feasibility testing and optimization of this technique will be designed in such a way as to take advantage of osmotic buffering to protect the structure of the islets and minimize osmotic swelling and lysis during efflux of the permeating CPA. Osmotic buffering would not impact the simultaneous destruction and lysis of the acinar cells since these would not have been protected by CPA permeation. Nevertheless, the ragged and uneven boundary appearance of the islets in this pilot experiment is not necessarily an indication of damage since the pancreases for these feasibility tests were harvested from young pigs (<6 months) from which islets are not generally easily obtained by the conventional enzyme digestion technique and which typically have a more ragged, ill-defined shape compared with the more rounded and compact appearance of islets from adult pigs (>2 years old) (4,7,16,23).
The demarcation of islets embedded in the cryoisolate fragments is clearly apparent using both dithizone staining and the Syto-13/PI fluorescent membrane integrity assay (Fig. 5A–E). The latter also shows that while the boundary between the “live” and “dead” tissue is clearly apparent (presumed to depict viable cryoprotected islets embedded in the freeze-destroyed exocrine tissue), this is not a completely all-or-none phenomenon. Some individual viable cells are seen scattered throughout the predominantly “dead” exocrine tissue, particularly in close proximity to the presumed “islet structure.” This observation is consistent with the notion that the kinetics of CPA permeation are not precisely controlled in these nonoptimized preliminary studies, and some leakage of CPA from the perfused islets into the surrounding acinar tissue prior to freezing would confer some cryoprotection to exocrine cells in close proximity to the islets. The high viability of the cryoisolated islets illustrated in Figure 5 is of particular significance because this cryoisolate was prepared from a frozen pancreas that had been stored at −135°C in vapor phase nitrogen for 8 months prior to cryoisolation. The ability to process a fresh pancreas with immediate cooling minimizes the cascade of injurious events inherent with warm ischemia and associated with conventional enzyme digestion processing for islet isolation. Moreover, the cryoisolation approach provides the convenience and benefits of long-term biobanking and shipping of the frozen pancreas and helps to maintain the islets in good condition in situ prior to cryoisolation.
Islets were typically larger (Fig. 4A, B) than their counterparts isolated from juvenile pigs using conventional enzyme digestion techniques, where >90% are in the range 50–100 μm (48). In marked contrast, islets identified in the cryoisolate ranged in size from <50 μm to >500 μm. This represents a potentially highly significant outcome, as it suggests that the cryoisolation technique could improve the yield of isolated islets by avoiding the inherent overdigestion of islets prepared using the collagenase enzyme approach. For example, based upon the standard convention for counting isolated islets, a single cryoisolated islet with a diameter >350 (Fig. 4A, B) is equivalent to approximately 100 islets in the range 50–100 μm typical of >90% of islets isolated from juvenile pig pancreas using conventional Liberase enzyme digestion (48). Moreover, this observation further suggests that the juvenile pig pancreas contains larger islets than has typically been assumed on the basis of conventional enzyme digestion of the pancreas (4,48).
Finally, evaluation of the cryoisolate for islet viability clearly showed the presence of functional islets on the basis of both a fluorescent membrane integrity test and glucose-stimulated insulin secretion, even after several months of storage of the CPA-impregnated pancreas.
Benefits, Challenges, and Further Development
These first attempts at cryoisolation of islets are highly encouraging, showing proof of concept that differential freezing conditions can be applied to a single pancreas to effect in situ cryopreservation of intact islets while facilitating the destruction of the surrounding acinar tissue. While the conditions selected for these pilot runs are unlikely to be optimal, our prior published studies on islet cryopreservation give some clues as to why these initial attempts were encouragingly successful.
In earlier published studies, we examined the interactions of the extent of DMSO permeation with cooling rate and warming rate as critical determinants of survival of isolated rat islets (51). From this, it was seen that survival would be expected to depend upon the interaction of these key variables in such a way that cooling at 11°C/min in these pilot experiments correlates with >50% survival of islet function normalized to controls when the islets were warmed quickly after full or partial equilibration with 2 M DMSO (51). These earlier studies further indicate that survival might be expected to increase to about 80% if cooling is reduced by an order of magnitude to approximately 1°C/min, and warming is rapid. This gives one clear direction for the further evaluation and development of this technique. Slow warming was detrimental for slowly cooled islets irrespective of whether the islets were fully or partially equilibrated with the CPA (20% survival). These earlier data support the notion that rapid warming of the cryoisolated islets by direct immersion in warm osmotically buffered medium is necessary for recovery of functional islets.
These earlier studies also give encouragement that the extent of equilibration with CPA might not be critical, provided that heat exchange is optimized toward fast warming coupled with slow cooling. It is anticipated that this could be beneficial in this newly proposed application since the conditions for full equilibration of islets in situ might not be easily determined in relation to the requirement for minimal permeation of the CPA into the exocrine cells. These interactive factors will be considered further in the design of studies for the further development and evaluation of this cryoisolation concept.
Islet Cleavage and Purification
In general, it has been the goal in the field of islet isolation to obtain purified preparations by complete cleavage of islets from the surrounding exocrine tissue. This has proved to be an ongoing challenge in order to judge the optimum endpoint of the enzyme digestion process to avoid destroying islets by overdigestion or losing islets entrapped in underdigested tissue. Nevertheless, there are reports in the literature that unpurified islets and tissue fragments survive longer than purified preps (8,15,25). Concern for the induction of apoptosis, mediated by disruption of cell–matrix interactions (11), has led to the suggestion that incompletely isolated islets that retain extracellular matrix connections might avoid inducing the transmembrane integrin signaling and prevent anoikis (34). More recently, it has been hypothesized from a review of the literature that extrainsular tissue, including acinar tissue, ductal tissue, peripancreatic lymph nodes, and vascular tissue, actually confer an advantage to islet survival/function after transplantation (61). Since the need or benefits of complete islet cleavage remains equivocal, it will be important in further development of this cryoisolation technology to explore the efficiency of the technique in separating the endocrine and exocrine portions of the gland. We anticipate, based upon our experience in cryobiology and the preliminary cryoisolation feasibility run, that the islets will not be completely cleaved. While this might be acceptable or even advantageous for transplantation based upon the premise outlined above, it will behoove us to explore ways to improve the efficiency of islet cleavage in the cryoisolation method should the basic method prove to be inefficient. One way to do this is to consider the option of including a low concentration of collagenase in the process to “clean up” the tissue fragments. Another conceivable way is to use tissue culture as a modality for the cleanup process, since the residual exocrine tissue injured during the cryoisolation protocol will die and disintegrate in culture.
Incompletely cleaved islets also impact conventional methods of density gradient purification and quantitation that will have to be taken into account during future studies aimed at optimizing this new approach. The significantly larger size of islets demonstrated in the cryoisolate by avoiding the inherent fragmentation due to enzyme digestion gives encouragement for anticipating greater yields of islet mass using the cryoisolation approach compared with enzyme digestion. This possibility will be the subject of further studies to develop this new technique.
Promoting Thermomechanical Stresses to Optimize Structural Destruction of the Gland at Cryogenic Temperatures
Having determined the feasibility of cryoisolation as a novel approach for reduced or enzyme-free isolation of islets, it will be necessary to optimize the baseline technique used in the feasibility studies. Based upon extensive experience with developing and optimizing both cryopreservation and cryodestruction protocols for a variety of tissues and cryosurgical applications, including pancreatic islets, future work will be designed to systematically optimize those variables in the procedure that are known to influence the cryopreservation of the islets in situ while maximally disrupting the exocrine portion of the frozen gland. Emphasis will be given to the generation of thermomechanical stresses in the gland to optimize the efficiency for differential freeze disruption and viable islet isolation (29,31,38). The objective will be to develop an experimental platform to facilitate pancreatic islet collection after thawing, with structural damage to the gland in the frozen state. In particular, we envision an experimental platform designed to generate thermomechanical stresses in the gland, which will ideally result in a dense network of fractures in the frozen organ. Four alternatives are identified for reducing the gland to small segments (fragments with cleaved, mantled, or embedded islets) at cryogenic temperatures: 1) mechanical impact, 2) grinding, 3) thermomechanical stress induced by differential expansion, and 4) thermomechanical stress driven by steep temperature gradients. The technique described in this preliminary, proof-of-concept study related to the first two alternatives, while a new experimental setup is envisaged to explore the feasibility of reducing the gland to small segments or fragments using the thermomechanical effects listed as the latter two alternatives (29).
Potential Benefits and Advantages of Cryoisolation
In summary, an enzyme-free method of islet isolation relying on in situ cryopreservation of islets with simultaneous freeze destruction of acinar tissue is feasible and proposed as a new and novel method that avoids the problems associated with conventional collagenase digestion methods. Successful demonstration of the feasibility of this new approach embodies a number of potential advantages and benefits of cryoisolation over the conventional enzyme digestion techniques, which are listed in Table 2. This successful proof-of-concept study now warrants further more in-depth analysis of the technique, which will include optimization of the cryobiological variables coupled with a more comprehensive assessment of islet quantity and quality. The latter should include a panel of relevant assays, such as oxygen consumption rate, insulin secretion during perifusion, and ultimately, transplantation into immunocompromised mice, as we have done with porcine islets isolated by the conventional enzyme technique (22,62).
Footnotes
Acknowledgments
The early discussions of this concept with David E. Pegg and the assistance of Elizabeth Greene in the preparation of the micrographs are gratefully acknowledged. This work was supported in part by a grant from NIH, National Institute of Diabetes and Digestive and Kidney Diseases # 1R43DK096773. The authors are presently, or were previously, employed by Cell and Tissue Systems during the course of this research work as indicated.