
Abstract

Dear Editor,
It is with great interest that we have read the recent article “Enhancement of Human Peripheral Blood Mononuclear Cell Transplantation-Mediated Bone Formation” by Yang et al (13).
Every surgically active orthopedist has experienced the problem of atrophic nonunion in fracture treatment causing difficult situations for both the physician and the patient. The situation demands revision surgery with autologous bone grafting, which results in a considerable burden for the patient and prolongs the course of the disease. Depending on the location of the defect or the fracture morphology, the risk of nonunion is often predictable. This fact reveals the urgent need for methods that enhance the bone-healing capacity in these patients.
The authors directly addressed this problem. They investigated the applicability of blood mononuclear cells to enhance bone healing in an ectopic bone model in the mouse. Here, they showed the bone formation capacity in a combination of applying blood mononuclear cells along with a scaffold and recombinant bone morphogenetic protein 2 (BMP2). Principally, this combination could be transferred to the bedside/clinic as a single-step procedure to enhance fracture healing in the medium term.
However, the presented study contains a few debatable points, and in the end, we are not totally convinced that the presented results allow the interpretation of osteogenic differentiation of the applied peripheral blood mononuclear cells (PBMNCs) in the way the authors did.
If, in fact, the applied cells showed differentiation into bone cells, as the authors conclude, we are wondering which subset of the cells did so. As noted by the authors in the introduction, it is assumed that PBMNCs contain certain cells with an osteogenic differentiation potential, namely bone marrow-derived osteoblast progenitor cells (OPCs) (10) and monocytes (7). Are OPCs identical with the previously published peripheral blood-derived multi-potent mesenchymal stromal cells (PBMSCs)? Regarding the published surface markers, both cell types do not differ (4). However, because of the low prevalence of circulating PBMSCs within the peripheral blood (0-0.27 cells per 106 PBMNCs according to the literature), we doubt whether the applied PBMSCs account for the observed ectopic mineralization, as the application of 1 × 106 PBMNCs per scaffold would equal 0.81 PBMSCs (2, 4, 8) at best.
So, if some of the applied cells have (trans)differentiated as the authors conclude, it seems more likely that these cells were monocytes (7). However, in our opinion, the authors did not present sufficient evidence to conclude that the applied monocytes transdifferentiated into osteoblasts. To substantiate their conclusion of osteogenic (trans)differentiation of the applied human cells, they showed costaining of osteocalcin and the human cell marker human nucleus histone H1 (HNH H1) in their Figure 3 and RT-PCR data for the human bone-related markers osteonectin, osteocalcin, and core-binding factor subunit α-1/Runt-related transcription factor 2 (Cbfa1/Runx2) in their Figure 4. Regarding their Figure 3, the human cells represented only a minority of the total number of cells as was revealed by the 4′,6-diamidino-2-phenylindole (DAPI) staining. However, the authors did not mention whether the osteocalcin antibody was specific for human samples, and thus it remains unclear whether the signal was specific for the human cells. The presented RT-PCR data included positive signals for Cbfa1, osteonectin, and osteocalcin in the PBMNC + BMP2 group. Unfortunately, the primers for the Cbfa1 were not specific for human cells. The authors also detected the murine gene product (Primer-BLAST, NCBI), for which reason the detected Cbfa1 signal may have partially or completely originated from immigrated host cells. The positive signals for human osteonectin and osteocalcin within the scaffolds did not necessarily prove the osteogenic (trans)differentiation of human cells, as these markers are indeed characteristic of, but not specific for, osteoblasts (1, 3, 5). As shown in Figure 1 included in this letter, cluster of differentiation 45 (CD45)- and CD68-positive blood monocytes do express osteonectin and osteocalcin as well. Hence, the detection of human osteonectin and osteocalcin does not necessarily prove osteogenic (trans)differentiation of the applied cells. Since the PCR experiments were performed in a standard endpoint format rather than in real-time PCR, the presented data precluded any quantitative assessments of mRNA abundance that may have contributed to the clarification of its cellular source. Taken together, the authors' results did not present sufficient evidence for their hypothesis of (trans)differentiation of the human cells.
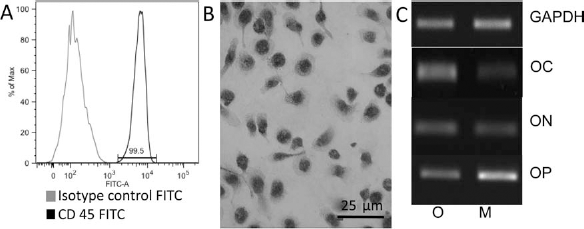
Investigation of human monocytes isolated by gradient centrifugation and subsequent selection via adhesion on day 6 of in vitro culture. Cells were obtained from blood samples of healthy volunteers who gave their written consent, with the approval of the responsible ethics committee of TU Munich, Germany. (A) Histogram of fluorescence-activated cell sorting (FACS) analysis for the hematopoietic marker CD45 [fluorescein isothiocyanate (FITC)-labeled mouse anti-human CD45 antibody; Biozol, Eching, Germany]; (B) immunohistochemistry for the monocyte marker CD68 (mouse anti-human CD68 antibody; DAKO, Glostrup, Denmark); (C) RT-PCR of osteoblasts (O) and monocytes (M). Cells are positive for the typical bone markers osteocalcin (OC), osteonectin (ON) and osteopontin (OP). Primer sequences: GAPDH, (s) GTCAGTGGTGGACCTGACCT, (as) AGGGGTCTACATGGCAACTG; OC, (s) ATGAGAGCCCTCACACTCCTC, (as) GCCGTAGAAGCGCCGATAGGC; ON, (s) AGCACCCCATTGACGGGTA, (as) GGTCACAGGTCTCGAAAAAGC; OP, (s) CTCCATTGACTCGAACGACTC, (as) CGTCTGTAGCATCAGG GTACTG.
An alternative conclusion compatible with the presented results is that host cells [e.g., mesenchymal stem cells (MSCs) or osteoprogenitor cells (OPCs)] were mobilized from bone marrow by the BMP2 signal and migrated into the BMP2-loaded scaffolds. Otsuru et al. (10) have shown that after implantation of a BMP2-loaded collagen scaffold of comparable size into a mouse model, the host tissue surrounding the implants expressed a large amount of stromal derived factor-1 (SDF-1). This was significantly promoted by the BMP2 signal. The SDF-1 effectively recruited CD45-negative, C-X-C chemokine receptor type 4 (CXCR4)-positive host OPCs from the bone marrow via the CXCR4 receptor. As a consequence, the number of CD45 negative cells rose from 20% up to 83% within the peripheral blood mononuclear cell fraction. Besides the effective migration of OPCs into the BMP2-loaded scaffolds, the mentioned work proved differentiation of the OPCs within the BMP2-loaded scaffolds into osteoblasts, expressing Cbfa1, osteopontin, alkaline phosphatase, and osteocalcin (10). According to the work of Otsuru et al. (10), host OPCs could have been effectively mobilized from bone marrow into the BMP2-loaded scaffolds where they differentiated into osteoblasts in response to the BMP2 signal. Here, they expressed murine Cbfa1 (which could have been picked up in the RT-PCR with the pan-specific primers) and mineralized matrix (which was detectable in x-ray analysis). The observation that the PBMNC + BMP2 group presented a better mineralization and detectable Cbfa1 expression in comparison to the BMP2 group may be due to the beneficial effect (possibly mediated by cytokine secretion) of the human PBMNCs on the osteogenic differentiation of the host cells (11).
If indeed it will be proven that the applied cells did not directly participate in osteogenic differentiation, it would be interesting to test whether the presented approach with PBMNCs shows advantages over the widely used method with platelet-enriched plasma (PRP) preparations. These PRP preparations are commercially available and already routinely used in patients (12). Furthermore, a PRP preparation contains the PBMNC fraction used in the present study (9). Possibly, the approach presented by Yang and coworkers does not differ from a previously published combination of PRP and BMP2 application (6).
Footnotes
Acknowledgment
The authors declare no conflict of interests.