
Abstract
Stem cells have received a great deal of interest from the research community as potential therapeutic “tools” for a variety of chronic debilitating diseases that lack clinically effective therapies. Stem cells are also of interest for the regeneration of tooth-supporting tissues that have been lost to periodontal disease. Indeed, substantial data have demonstrated that the exogenous administration of stem cells or their derivatives in preclinical animal models of periodontal defects can restore damaged tissues to their original form and function. As we discuss here, however, considerable hurdles must be overcome before these findings can be responsibly translated to novel clinical therapies. Generally, the application of stem cells for periodontal therapy in clinics will not be realized until the best cell(s) to use, the optimal dose, and an effective mode of administration are identified. In particular, we need to better understand the mechanisms of action of stem cells after transplantation in the periodontium and to learn how to preciously control stem cell fates in the pathological environment around a tooth. From a translational perspective, we outline the challenges that may vary across preclinical models for the evaluation of stem cell therapy in situations that require periodontal reconstruction and the safety issues that are related to clinical applications of human stem cells. Although clinical trials that use autologous periodontal ligament stem cells have been approved and have already been initiated, proper consideration of the technical, safety, and regulatory concerns may facilitate, rather than inhibit, the clinical translation of new therapies.
Keywords
Introduction
Teeth serve as a means for mastication, phonation, and speech, and they shape our smiles and facial expressions. Although teeth can withstand enormous abrasive forces, their supporting apparatus (i.e., the periodontium) (Fig. 1) is susceptible to damage from bacterial attack, chemicals, and/or mechanical trauma. Periodontitis is a common, globally prevalent human chronic inflammatory disease encountered in dentistry (16, 23, 160). The disease causes pathological alterations and tissue degeneration in the alveolar bone and the tissues that surround and support the teeth (23, 160). If left untreated, these conditions may lead to tooth migration and mobility and eventually result in loss of the affected teeth (89, 160). In fact, periodontitis is the leading cause of tooth loss in adults, which indicates the urgent demand for effective management of this condition.

A schematic illustration and histological tissue sample (from dog) of the tooth supporting apparatus in normal periodontium. PDL, periodontal ligament.
Periodontal therapy has two main objectives: to arrest periodontal disease progression and to regenerate lost/ damaged periodontal tissues. Early efforts such as open flap debridement (OFD) and bone correction have focused on providing appropriate conditions for wound healing, in which the elimination of the periodontal infection is generally achieved by tooth scaling and root planning (3, 88). However, instead of the restoration of the periodontium's original architecture or function, healing occurs largely by a process known as periodontal repair, which leads to a long junctional epithelium that forms an attachment to the root surface (89, 215) (Fig. 2A). Subsequently, guided tissue regeneration (GTR), in which a temporal and spatial space that facilitates true periodontal regeneration is created, has been established as a valuable procedure that may yield highly beneficial clinical outcomes in certain clinical scenarios (211) (Fig. 2B). However, quantitative analysis of clinical data after GTR suggests that this therapy is only a successful and predictable alternative in a very few well-selected cases, such as those that involve narrow intrabony defects and class II mandibular furcations (23, 215).

A schematic representation of long junctional epithelium healing after OFD and periodontal tissue regeneration after GTR therapy. A schematic representation of long junctional epithelium healing after open flap debridement (OFD) (A) and periodontal tissue regeneration after guided tissue regeneration (GTR) (B) therapy [modified from (215)]. The periodontal defect normally fills with the epithelial cells and fibroblasts that generate a core of fibro-epithelium after OFD, which prevents true periodontal tissue regeneration. Following flap reflection and root planning, GTR employs a barrier membrane to prevent epithelial down-growth and fibroblast transgrowth into the wound space, thereby facilitating the maintenance of a site for target periodontal tissue regeneration. PDL, periodontal ligament; AL, attachment loss; PD, pocket depth.
The adjunctive use of various growth factors (100, 171, 184, 199), enamel matrix derivatives (EMD) (169, 180, 223), and platelet-rich plasma (PRP) (6, 70, 222) with GTR has been demonstrated to enhance the total outcome of periodontal therapies and implant surgery in both animal models and human clinical trials (22, 23, 112). These biological modulators/mediators appear to accelerate the recruitment and repopulation of a variety of tissue-forming cells, including progenitor and stem cells, within the periodontal space and may encourage further progression of endogenous periodontal regeneration and faster osseointegration of dental implants (100, 171) (Fig. 3). Although current endogenous regenerative technologies are promising, they do not offer a universal regenerative solution. Healing may be restricted by an age-related decline in progenitor populations or by the intrinsically low regenerative potential of certain tissues such as the periodontium (161). To date, the goal of complete, predictable regeneration of damaged tooth-supporting apparatus has not been attained, especially in cases of advanced periodontal defects or dentoalveolar ridge defects in implant sites (6, 7, 25, 26, 215).
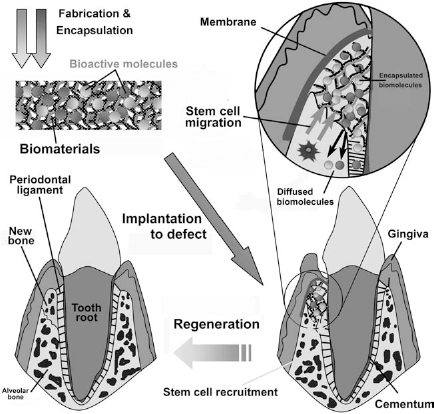
A schematic representation of the endogenous regenerative strategy for periodontal regeneration wherein biological molecules and pharmaceutical agents are encapsulated in an acellular scaffold (biomaterial) for release after implantation to induce the recruitment of endogenous stem cells for regeneration (only a small subset of patients can ultimately benefit from these techniques).
In recent years, cytotherapeutic approaches have been investigated to overcome the limitations of existing procedures for periodontal regeneration (224). Cell-based therapies may represent the next wave in biological production and promises to provide cures to patients suffering from a spectrum of degenerative diseases, including periodontitis, through cellular replacement or tissue engineering-based regeneration (23, 37, 119, 154). Stem cell populations that possess the abilities to self-renew and to maintain a differentiated and functional cell type for the life of an organism are particularly appealing therapeutic agents due to their typically rapid and extensive proliferation and their potential to provide customized cells to the patient (37, 154). The use of stem cells for regenerative therapy crosses all disciplines of medicine and provides a universal paradigm of curative goals based on scientific discovery and clinical translation (35, 36, 102).
Nonetheless, to explore new therapeutic applications, stem cell therapy constitutes one of the most complex organizational and regulatory areas (37, 154). Similarly to the difficulties described in the literature (168), the introduction of stem cells into widespread dental healthcare faces a number of biological, technical, and clinical challenges (10, 28, 119). The scientist or clinician who attempts to implement stem cell science into clinical practice may feel overwhelmed by the apparently endless regulatory requirements and practical issues that must be confronted to move from proof-of-concept studies in animal models to trials with human subjects (35, 36, 102). However, periodontal regenerative medicine based on stem cell biology continues to expand its scope. With the help of further translational research and interdisciplinary collaboration, this type of regenerative medicine will definitely offer new classes of therapeutics for treating diseases with safer and more effective outcomes that are not possible with current therapies (35–37, 94, 102, 154).
In this article, we provide an overview of the ongoing novel approaches that use stem cell-based therapies in the field of periodontology, with particular emphasis placed upon the considerations involved in the translation of these innovations from the bench to the bedside. In this regard, we outline the steps that are needed to move stem cells into clinical dentistry and the challenges that lie ahead on the stem cells' “roadmap to clinical practice.” Finally, we offer a complementary perspective on the safety issues for stem cell-based products and clinical protocols for stem cell-based therapies in periodontal regenerative medicine. Although our focus in this review is on the regeneration of the periodontium, the concepts introduced should be more generally applicable to other tissues.
Stem Cell-Based Therapies: From Bench to Bedside
Stem cells are central to the development of new treatment options for tissue regeneration and the construction of controllable models for biological research. In recent decades, the accelerated pace of stem cell research and the accumulated body of knowledge have spurred interest in the potential clinical applications of stem cells as regenerative “tools” (154). Initial evidence from pioneering studies has documented the likely breakthrough that stem cells offer for various human diseases that have so far defeated modern medical care (36, 37, 154). To a certain degree, stem cell research has already resulted in a number of clinical applications, such as those for the repair of skin (147), bone (166, 208), articular cartilage (14), and cardiac tissues (193, 216), and therapeutic treatments for diabetes (9) and systemic lupus erythematosus (200). The role of stem cells in this context is under intense scrutiny and may help to define the principles of organ regeneration through the development of innovative therapeutics for organ failure. Meanwhile, the evidence gathered thus far has driven many elegant studies to explore the role of stem cells and their manifold dental applications (10, 116, 212). To this end, considerable efforts are devoted to the development of stem cells as therapeutics in regenerative dentistry, which offers scientists hope for the eventual availability of tooth/ periodontal tissue reconstruction methods (10, 20, 119, 212). Given this level of excitement, it is hardly surprising that the theory-to-therapy approach to the use of stem cells would move forward into translational human studies at the earliest possible stage. However, the translational arm of stem cell science in dentistry largely remains in a relatively primitive state compared with other related research fields such as the management of Alzheimer's disease and cardiac ischemia (28, 71). Nevertheless, collective progress in stem cell technology, biomaterials, engineering, and molecular medicine has advanced the state of periodontal regenerative medicine in recent years and has opened new avenues for translational research in the treatment of periodontitis. Yet, several inherent problems with the translation of stem cell therapy into clinical periodontology must be carefully considered (119).
First, given current knowledge, there remains doubt on the subject of introducing stem cell-based therapy into clinical regenerative dentistry (28). Thus far, there is no way of knowing how successful these therapies will eventually prove to be in our clinics. In contrast to incurable and life-threatening diseases such as neural or cardiac diseases (9, 193, 216), for which cell-based therapy is more likely to be warranted and accepted by both the government and patients, periodontal tissue regeneration by cell therapy will not be economically viable or competitive with current root canal therapy or dental implants, at least not in the field of public opinion today (28). Of note, teeth are nonessential for life and are thus not considered to be a major target for stem cell therapy. Nonetheless, this very fact makes therapeutics that aim at the regeneration of periodontal tissues ideal for the evaluation of new cell-based therapies. Because the patients are usually healthy, possible therapeutic complications would be far less risky or life-threatening for such healthy patients compared with those with substantial comorbidity (28, 212). In this regard, periodontal surgeons are in an ideal position to capitalize on emerging technologies and will be, as noted in another conceptual paper (28), at the forefront of the transition of stem cell research into the clinical reconstructive arena, although safety issues cannot be ignored (224). In fact, a wealth of scientific and preclinical research has demonstrated that stem cell transplantation can regenerate periodontal tissue (15, 41, 43, 44, 48, 49, 83, 96, 116, 145, 155, 207, 213, 219, 221, 228), and several clinical trials involving the use of stem cells in human patients have already begun or are in preparation (52, 134, 224).
From a regulatory perspective, a number of translational issues need to be addressed before any form of cell therapy can be widely applied for patients with periodontal disease (28, 119, 168). For example, the diversity of stem cells available offers a variety of choices to clinicians, and a universal stem cell for “all diseases” is unlikely to exist (28, 168). Therefore, the “right” stem cell will have to be used for the “right” disease, which suggests that the choice of the optimal cell type is one to be considered carefully; other considerations include the mode of in vivo delivery of cells, the problem of directly or indirectly measuring the impact (if any) of an intervention, the timing of any treatment, and, perhaps above all, the safety of the patient (178).
Given the above considerations and challenges, the question arises as to exactly where we are on the translational road map from stem cell biology to stem cell therapy. At this moment, are we headed in the correct direction, taking a tangential course, defining a rigorous and standardized clinical protocol, or have we reached a fork in the road (71)? Prior to clinical application, it must be demonstrated in animal models that a stem cell-based approach induces substantial improvement of the functional deficits that resemble debilitating symptoms in patients (158). In addition, it is important to determine the biological mechanism underlying the observed effects of a stem cell-based treatment in an animal model; the events following cell transplantation are currently poorly understood (97, 224). From careful examination of the literature, it is evident that much more remains to be performed to introduce stem cells as therapeutics in clinical periodontal regenerative medicine (Table 1).
Main Considerations and Challenges in Designing a Stem Cell-Based Therapy for Periodontal Regeneration in Human Beings

For stem cell-based periodontal therapy, we must be aware that several of these requirements can be tabled, but not overlooked, due to the nonfatal nature of the disease. If we wait for every question to be answered, the timely introduction of novel treatments will be impossible (28). Of note, there is mounting evidence that highly proliferative stem cell populations exist in and around the teeth (68, 86, 87, 133, 138, 141, 182, 188, 189, 204, 227) and can be easily obtained from naturally lost or surgically removed teeth and cultured in vitro under ordinary serum-supplemented culture conditions. It is also suggested that stem/progenitor cells from either inflamed human dental pulp (4) or inflamed periodontal ligament (PDL) tissue (156) retain tissue regeneration potential, which renders the isolation of useful dental stem cells from biologic waste (e.g., teeth that are extracted for clinical reasons) a possibility.
The multipotency, high proliferation rates, and accessibility of dental stem cells make them an attractive source of mesenchymal stem cells (MSCs) for tissue regeneration (4, 68, 90, 138, 156, 182, 189, 227, 228). The discovery that odontogenic tissues are a source of adult stem cells has opened up a new role for dentists in the field of translational medicine (28, 198). Dentists are positioned to become key providers of stem cells, and as a result, their linkage with the medical field will become very intimate. However, stem/progenitor cells isolated from dental follicles fail to form dentin, cementum, or bone in vivo, although they express high levels of bone sialoprotein, osteocalcin, and alkaline phosphatase (141). Such results are suggestive of the selective behaviors of different cell types in translational research in periodontal regeneration (28). Although studies have shown that stem cells from one tissue can generate cell types of a completely different tissue, adult stem cells normally generate cell types of the tissue in which they reside. Therefore, periodontal ligament stem cells (PDLSCs) are the primary candidate among dental stem cells for clinical trials of periodontal regenerative therapies (119). In addition to the choice of an appropriate cell type, translating preclinical tests to human trials is compounded by consideration of the delivery method to be used and translation of dosages in accordance with cell survival. Many other issues must be approached when designing clinical trials of cellular therapies for periodontitis. Such issues include appropriate outcome measures, controlling for confounding factors such as individual differences, and the existence of possible surrogate outcomes through the use of magnetic resonance imaging (MRI) and newer imaging techniques. It is also important to establish standardized clinical protocols and clinical database registries in advance of early proof-of-concept studies (28). Investigators must adopt a standardized nomenclature and characterization schema for cell products to accurately define potency and determine clinical outcomes from early proof-of-concept studies (224).
Overall, stem cell therapy holds promise for addressing a number of unmet medical needs but, despite its considerable impetus, faces numerous challenges that include support for translational research in this area. In the following sections, we will review the progress in various practical problems to explain how we have arrived at the conclusion that clinical science has progressed to a stage at which the “translation threshold” can be safely and appropriately crossed, and therefore, why we have already commenced a small pilot/feasibility study of autologous PDLSC treatment in patients with periodontitis in Xi'an, China (NCT01357785). Bearing in mind the essential need for the translation of basic research into clinical practice, we also attempt to tackle the controversial issue of how cost-effective periodontal therapy is and how we can address the biggest challenge that periodontal physicians and surgeons face in day-to-day practice: the biological approach to changing patients' oral health.
Preclinical Models
Demand for Preclinical Models
The use of animal models in translational research is a necessary step prior to the initiation of clinical trials with new therapeutics (197). The anatomy, physiology, and pathogenicity of experimental models should relate as closely as possible to those of patients to demonstrate the clinical potential, efficacy, and safety of new treatments before they are applied in humans (158). Although a number of preclinical models, such as furcation, dehiscence, fenestration, supra-alveolar, and intrabony defects, that predominantly use canine or nonhuman primate platforms are suggested for use to evaluate various proposed new therapies, which model is most suitable for the evaluation of cell-based therapy for pathological situations that require periodontal reconstruction remains to be identified (97, 158, 190, 197). We are aware of animal models that have provided a large amount of data, but it is sometimes difficult to determine whether such findings are applicable to humans. It is increasingly apparent that animal models often fail to capture all of the aspects relevant to the transition from lead validation to clinical development. Notwithstanding such limitations, in vivo models do provide distinct advantages for better understanding aspects of the molecular, cellular, tissue, and anatomical processes that occur in response to the delivery of therapeutic cells. Notably, some large-animal (canine or nonhuman primate) preclinical studies have accurately predicted the outcomes of large Phase II and phase III randomized controlled human trials for biologics [reviewed in (158)] such as fibroblast growth factor (FGF)-2 (103, 104, 144) and platelet-derived growth factor (PDGF)-BB (60, 78, 148). Although these models are strongly applicable in the development of clinical guidelines and endpoints for the initiation of human clinical trials, much more remains to be considered if they are to be used as animal models for cell-based translational research.
Surgically Created Defects
In terms of surgically created models, furcation defects are considered to be clinically reproducible and have been recommended as a preferred model to evaluate periodontal regeneration procedures; degree II furcation defects generally present more favorable healing outcomes than degree III furcation defects (17, 64, 82, 121). Recently, it has been found that effective periodontal regeneration can be induced by the delivery of either bone marrow mesenchymal stromal cells (BMSCs) (72) or BMSCs transfected with FGF-2 in this defect model, for which the regenerative speed of periodontal bone tissue in groups transplanted with BMSCs containing the modified FGF-2 gene was greater than in those transplanted with BMSCs alone (203). To compare the effectiveness of MSCs with PRP as a scaffold and autogenous cortical bone (ACB) grafts with and without PRP in the regenerative treatment of class II furcation defects (5 mm in height and 2 mm in depth) in dogs, Simsek et al. concluded that there is no significant difference in periodontal regeneration between ACB, ACB/PRP, and MSCs/PRP treatments, with complete filling of class II furcation defects with cementum, alveolar bone, and PDL in all groups 8 weeks post-surgery (186). However, the use of BMSCs and PRP led to a reduction in intrabony defect depth and a resolution of bleeding and tooth mobility in a subsequent small clinical trial (218). Therefore, class II furcation defects seem to be an inadequate model for studying periodontal regeneration with respect to testing cell-based regenerative procedures. Meanwhile, we must be aware that the treatment outcomes for furcation defects may vary with defect morphology, the size of the furcation defects and the shape of the surrounding alveolar bone (163). In addition to interproximal bone height, treatment outcomes may also be significantly affected by tooth anatomy, such as root divergence and root trunk length (151, 163).
The development and characterization of the critical-size, supra-alveolar, periodontal defect model was first proposed by Wikesjö et al. in 1991 (214), and studies of these defects are much better at assessing periodontal regeneration than the dehiscence defect model. However, dehiscence defects also represent a common clinical situation [reviewed in (97)] and may still be used as a simple model to evaluate the biodegradation of a biomaterial within the periodontal environment (61).
Fenestration defect models have great regenerative potential and optimal healing capacity (18, 19, 179), but they may be useful only to evaluate early healing events in response to various therapeutic procedures. Although these models allow the study of periodontal healing/regeneration without interference from the oral epithelium, saliva, and oral microorganisms (202), fenestration defects have disadvantages and are less suitable for studies of the regeneration of PDL (152). Through the use of fenestration defects, Li et al. suggested that cryopreserved BMSCs had a regenerative capacity 8 weeks after surgery that was similar to that of freshly isolated BMSCs in the application for periodontal regeneration (116). However, this similarity must be further confirmed in other more complex situations.
The one-wall intrabony defect model is a surgically created, experimental periodontal defect model (acute model) that is an alternative to natural disease or ligature-induced periodontal models (chronic models) [reviewed in (97)]. The one-wall intrabony defect model is a preferred model with which to observe the nature of wound healing after periodontal regenerative therapy and to evaluate the efficacy and safety of adjunct biomaterials, biological modulators, grafts, and alternative treatment concepts prior to clinical application (98, 99, 113, 194). Although three-wall defects also appear to be reproducible models and have been used to examine multilayered sheets of PDL-derived cells for periodontal regeneration (91), the superior measurement outcomes of one-wall intrabony defects suggest that they, rather than three-wall intrabony defects, should be considered when quantitative evaluations are required (97).
Crucial Barriers to Progress
From a careful examination of the literature, it is evident that advancements are still needed to better exploit preclinical animal models for the evaluation of cell-based periodontal therapies prior to human testing. For example, cell-based therapeutics have not yet been tested in the critical-size, supra-alveolar periodontal defect models. Compared to surgically created periodontal defects, models of periodontitis may mimic natural periodontal tissue loss much more closely, although currently available disease induction protocols (modulating host defenses, introducing microbial flora) remain largely unrefined (41, 123, 153). Periodontitis models in different species commonly are induced by the placement of a bacterial plaque retentive ligature in the gingival sulcus around the molar teeth. In addition, alveolar bone loss has been induced by the inoculation or injection of human microbial pathogens in different animal models (153). Clearly, methods that may mimic the natural development events of periodontitis remain to be established. Challenges in this field include, but are not limited to, obvious differences in host–microbial interactions, defect morphology, and the implications of long-term disease development (97, 153, 158). Moreover, the selection of appropriate animal models to the satisfaction of regulatory authorities is often a difficult dilemma. Smaller immunodeficient rodent models such as rats and mice are useful for assessing functionality, retention, and safety issues related to the administered human stem cells but have limited utility in providing anatomical and physiologically relevant data. In this regard, larger animal models such as nonhuman primates and monkeys may be more relevant, especially for the assessment of specific delivery devices, route of administration, stem cell dose, and volume. However, studies with large animal models are very expensive and are often limited to specific centers that house the appropriate infrastructure, resources, and expertise, which makes the studies financially and scientifically less accessible (97, 153). Furthermore, to allow for more targeted and refined human clinical investigation, the continued development of systemic health status (e.g., simulating common disease conditions that alter wound repair, such as diabetes mellitus, cigarette smoking, osteoporosis, and others) lies ahead of the continued refinement of preclinical animal models. The use of a genetic animal model to explore new aspects of periodontium development can provide a better understanding of the causes and progression of periodontal injuries in humans.
Overall, current animal models in which well-defined defects are produced and studied may not be appropriate for the evaluation of periodontal regenerative protocols in humans (214). A simple and reproducible model that truly mimics the human pathogenesis of periodontal disease has yet to be discovered (153). Increased growth in the development of cell-based approaches for periodontal regeneration requires a thorough examination of when and how the appropriate endpoints can be evaluated prior to entry into human clinical trial testing (158). Additionally, translation of the knowledge and understanding gained from animal models to human trials requires attention to the differences between animal and human periodontitis.
Design of Implantation
Cell Administration Modes
Although the major effort in this field thus far has been and still is the identification of potentially therapeutic cells, it is now clear that the development of delivery techniques to transplant these cells into the body and promote their efficient engraftment will provide an equally challenging task (140). The delivery of cells where they are needed is of tantamount importance to the discovery of cell sources because proper cell function and cell fate is influenced by a number of in vivo factors and interactions that require robust control for the safe and effective regeneration of functional tissue (42). Historically, the most direct and convenient means of cell delivery has been the direct injection or infusion of a suspension of cells into the diseased site (140) (Fig. 4A). However, the efficacy of injected stem cell-derived populations in the regeneration of the targeted tissues and organs is less tangible and remains a controversial issue. More importantly, intraosseous periodontal defects involve substantial structural deficits and require bridging or filling materials that function as synthetic analogs of the extracellular matrix (ECM) to provide a substrate for transplanted cell adhesion, to control the localization of the cells in vivo, and to serve as a template for the formation of new tissue masses (199). In such cases, cells need to be delivered in a matrix-guided manner, and it has been assumed that they can replace cells that have been lost or damaged by disease in the target location (Fig. 4B). Of note, there has been considerable progress in the development of bioengineered constructs derived from the incorporation of cells into natural or synthetic biomaterial scaffolds following their expansion and differentiation in vitro (15, 41, 43, 44, 145, 155, 207, 213, 219, 221) (Fig. 4C). We are aware that the cell scaffolds made today are routinely information rich and incorporate biologically active components that are used to alter cell fate in vivo or to induce the artificial formation of tissues or organs in bioreactors (i.e., to engineer such tissues before their use in the regenerative treatment of choice) (27). These medical devices are capable of producing three-dimensional (3D) engineered tissues with mechanical properties that are compatible to those of various functional tissues (150). Although these sophisticated approaches are promising, they have yet to be tested for periodontal regeneration.

Proposed strategies for stem cell delivery in periodontal regeneration. Stem cells are isolated and expanded in culture prior to transplantation or used with minimal manipulation after harvest and then delivered by one of four strategies (cells that are not immediately used may be stored for future use). Cells suspended in medium (or injectable biomaterials) can be injected directly into the diseased periodontium (A), where they are expected to move to the site of interest or stay at the site of injection and function via the secretion of trophic mediators to elicit regenerative effects, instead of or in addition to direct participation in tissue building. For matrix-guided delivery, cells may be seeded on a material vehicle, which is typically a biodegradable polymer, and then implanted at the site of injury (B). Alternatively, cells are allowed to proliferate and differentiate on the vehicle (or scaffold) to create tissue-like constructs in culture prior to transplantation (C). Based on this concept, cell biomaterials are cultured in a bioreactor and the generated constructs are implanted at a specific anatomic site, where the scaffold serves as a template to guide tissue formation and is typically designed to degrade in concert with the deposition of new extracellular matrix (ECM) and cell proliferation. Recently, cell sheet engineering has been developed as an alternative for cell delivery in the field of periodontal tissue engineering (D), either through the direct transplantation of cell sheets in host tissues or by the homotypic layering of individual cell sheets. In this manner, an entirely natural periodontal tissue assembled by cells with mature ECM can be engineered to avoid the shortcomings of traditional scaffold-based design.
Recently, the use of naturally occurring ECM materials as scaffolds, termed cell sheet engineering, for the repair and regeneration of periodontal tissues has been receiving increased attention. This novel technique enables the transplantation of cell sheets with their conserved structures, so the functional in vitro constructs can be transplanted directly to the wound in vivo (89). Strategies that assemble monodispersed cells in a tissue-mimicking manner represent a valuable extension of current scaffold-based tissue engineering initiatives and could be feasible as new therapeutic approaches for cell delivery that would be useful in clinical settings (41, 55, 56, 207, 213, 220) (Fig. 4D).
However, there are some drawbacks to the use of cell sheets. A principal disadvantage is their poor mechanical properties, which leads to a demand for additional materials such as fibrin gels during stratification and makes it difficult to fabricate grafts with certain thicknesses and controllable stiffness (41, 220). Finally, the fundamental question of which approach or combination of approaches for cell delivery will lead to the most successful cell engraftment, survival, and physiological functioning will ultimately depend on the disease to be treated, the method/site of implantation, and the health status of the individual patient. Answers to these questions will require extensive additional basic research (48).
The Role of Biomaterials in Delivery
Advances in our understanding of the interactions of stem cells with their in vivo milieu are leading to the development of new biomaterials-based approaches for delivering stem cells and regulating their fates toward the regeneration of target tissues (77, 130). Material carriers may be particularly useful for quantitatively controlling and manipulating not only the fate of the transplanted cells but also the endogenous niche cell populations that may contribute to tissue repair (89). The combination of stem cells with biomaterials, and sometimes also with growth factors, may largely enhance the efficacy of cell therapy (199). While cells are fabricating their own natural matrix structure around themselves, the scaffolds should provide structural integrity and then eventually break down to leave the newly formed tissue. During this process, the cells should maintain important characteristics of stem cells and allow for appropriate differentiation of their progeny (39, 174). Although sophisticated pretransplantation manipulations and material carriers may dramatically improve the survival, engraftment, and fate control of transplanted stem cells and their ultimate clinical utility (140), for commercial success, cell therapy products must be efficacious and cost-effective, which introduces a potential dichotomy between the need for sophistication and ease of production in cell-manufacturing bioprocesses (161). Clearly, there is a danger that the over-engineering of devices will make their translation to clinical use unlikely. The solutions to this challenge is to monitor every phase of cell-based product development, including bioreactor design and process control, and identify the simplest functional performance required to resolve a defined clinical problem (161).
To provide appropriate physical (e.g., strength) and chemical (e.g., degradation rate) properties, vehicles for cell delivery have traditionally been designed from a classic materials science perspective (111). To bridge the gap between stem cell research and clinical application, the delivery scaffold needs to function as a developmentally conducive extracellular niche at a clinically relevant scale and in a manner that accommodates stringent clinical prerequisites (including economic and manufacturing prerequisites) (39, 199). In this context, the scaffold facilitates the delivery of cells and/or growth factors to the site of damage and provides an appropriate template for new tissue formation. The scaffold should thus constitute a dynamically durable but degradable 3D structure that serves as a functional tissue substitute that, over time, can be replaced by cell-derived tissue function (39). More recently, however, the design space for synthetic biomaterials has expanded to include biological criteria that mimic the regulatory characteristics of natural ECMs and ECM-bound growth factors (127). Diverse techniques are now available to produce cell delivery systems with networks of channels and interconnected pores, different pore sizes and surface area to volume ratios, and the properties of biocompatibility and hybridizability with a wide spectrum of molecules (45, 126, 130, 199).
Consideration of Material Types
Biomaterials for cell delivery can be either naturally derived or synthetic. The advantage of employing natural biomaterials, such as collagen (13, 57), fibrin (118, 191), hyaluronan (i.e., hyaluronic acid, HA) (118), or chondroitin sulfate (CS) (53) for cell delivery scaffolding is their similarity to the ECM (i.e., their ability to mimic certain aspects of native ECM). These materials facilitate cell adherence, migration, differentiation, and ECM deposition, and exhibit high chemical versatility, typically good biological performance, and inherent cellular interaction and cell- or enzyme-controlled degradability (80, 129). However, the limitations of natural polymers are their range of physicochemical properties, requirement of extensive purification protocols, and potential pathogen contamination when harvested from animal or human sources (42). In addition, a substantial variable space inherent to these delivery systems exists because they combine various cues (e.g., types, densities, and organization of adhesion ligands, and the presentation of various cytokines and growth factors); the development of large-scale screening approaches will be required to thoroughly and systematically examine this space to design optimal material systems for clinical application (5).
Synthetic biomaterials such as poly(α-hydroxy esters) and ceramics commonly offer higher primary stability and are more amenable to macro-/microstructure formation than natural biomaterials (187). Polymer composition, hydrophobicity, crystallinity, and degradability will affect the rate of cell release from these scaffolds and the rate of tissue ingrowth. At the current stage of periodontal tissue engineering, new biomaterial schemes for clinical cell administration that make better use of the biological principles of osteogenic growth factor function and the cell biology basis necessary to produce functional tooth-supporting structures are evolving (23). Alongside their basic function as protective embedments for osteogenic growth factors, these new classes of bioactive polymers are engineered with additional functionalities that better preserve growth factor activity and more closely mimic the in vivo release mechanisms and profiles of multiple growth factors from the ECM (22, 25, 26). Consequently, the preparation of either natural or completely synthetic materials with biological characteristics of the ECM has become central to periodontal tissue engineering approaches that aim to deliver both stem cells and growth factors in a therapeutically efficient mode (24, 199). Although current systems demonstrate incremental advances in transplanted cell utility, strategies that integrate multiple cues into one system may provide drama tic improvements in the future (22, 27).
Further Redesign of Biomaterials
The design of cell delivery vehicles in the future will likely continue to take inspiration from the specialized microenvironments (i.e., natural stem cell niches) that contain and controllably activate stem cell populations within tissues (140, 199). Coordinated interactions with soluble factors, other cells, and ECMs define a local biochemical and mechanical niche with complex and dynamic regulation that stem cells sense (42) and that orients the cleavage plane during stem cell mitosis to control the balance between symmetric and asymmetric division and, therefore, fate and function (136). Together with these advances, it may be possible to devise more sophisticated delivery systems that localize and maintain the viability of the delivered cells and activate the cells to a proliferative state. These types of systems may also induce their daughter cells to migrate outward over time to provide a continuous flow of cells at the optimal differentiation state for their direct participation in regeneration (140). In addition, these systems may also be designed in the future to enhance the homing of exogenous (135) or host progenitor cells (63, 80) prior to local, material-controlled programming and redispersion to sites of tissue repair (140). However, before these synthetic medical devices are to be used in the clinic, several fundamental aspects such as the design of cell–material interactions and the contribution of delivered stem cells to tissue homeostasis and repair need to be clarified in translational research (42).
Recently, biologically inspired (biomimetic) structural designs of biopolymers have been used to endow cell delivery devices with versatile functionalization chemistries, flexibility in fabrication, and biocompatibility in vitro and in vivo (199). In this regard, polymeric materials such as alginate, collagen, chitosan, and silk are being explored as bulk and film materials for cell delivery that may provide a path toward clinical applications (5, 127). In particular, hydrogels offer a means of creating mechanically functional devices for cell delivery systems and lead the way in the production of a new generation of medical devices for translational research (45, 107). Based on our attempts in this field (29–31) as well as those of many others (33, 58, 73, 75, 76, 132, 139, 167, 210, 226), perhaps one of the most intriguing directions for future research is the development of hydrogel devices that can integrate with existing vasculature and slowly degrade to fully recapitulate native tissue structure and function while providing critical interim functions such as tissue maintenance, drug release, mechanical support, and cell delivery (32, 62, 105, 109, 117, 209). However, further refinement of the methodologies used to propagate and incorporate cells into a hydrogel scaffold is needed. An ideal methodology should encourage the integration and function of the implanted cells alongside the host cells.
Because it is still not clear whether human stem cell derivatives can integrate into recipient tissue and fulfill the specific functions of lost or injured tissues, it will be necessary to demonstrate that, after transplantation, stem cells develop into stable cells and display the characteristics and functions of normal host cells (224). With this in mind, one soon realizes that the true obstacle lying in the road of translation comes from stem cell biology rather than biomaterials science. It is hoped that as our knowledge of progenitor cells, growth factors, and delivery systems improves, we will make stem cell-based therapy a safe, robust, and effective approach for periodontal regeneration. The rate at which biomaterial approaches are being applied to address questions in stem cell biology ensures that new insight into the mechanistic regulation of stem cell fate will be gained (199). Although there are now many ingenious biomaterial platforms with which to analyze the biophysical and biochemical properties of stem cell niches, these platforms have only just begun to be applied to directing stem-cell fate (45, 126, 130, 199). Despite the high expectations, only a handful of cell therapeutic products have made it to market, of which the vast majority are in preclinical and early clinical development. Whether these potentially curative technologies ever reach (or are even tested on) patients will ultimately depend on technologies to manufacture (and deliver) cells in a robust and cost-effective manner (102). Collaborative efforts between cell biologists and materials scientists are critical for answering the key biological questions in cell delivery design and fostering interdisciplinary stem cell research in directions of clinical relevance (126).
Assessing the Effects of Cell Therapy Intervention
The history and fate of transplanted stem cells or progenitor cells is generally assessed by in vitro labeling with a fluorescent dye, thymidine analog [e.g., bromodeoxyuridine (BrdU)], or transfected gene, such as LacZ or green fluorescent protein (GFP), and visualization by immunohistochemistry after the removal of the tissues or organs (54). Measuring any effects of an investigative stem cell therapy in periodontal medicine is no easier than it is in any other therapeutic intervention in medical science, and we can learn from the valuable information emerging from other published materials including clinical trials of cell transplantation for cases of cardiac/musculoskeletal injury (66, 74, 93, 181). Meanwhile, biomedical imaging is developing very quickly, and a number of new tools are increasingly being used to monitor/track the fate of transplanted stem cells; this assessment includes but is not limited to cell survival, migration, proliferation, differentiation, homing to their targeted destinations, and regenerative impact (114, 195). For example, potentially reparative cells can be labeled with magnetic nanoparticles (a noninvasive, in vivo method to study the fate of transplanted cells) to render them MRI visible after implantation, and superparamagnetic iron oxide (SPIO) nanoparticles have been used as a feasible means to enhance the contrast of cellular targets in MRI (115). The use of SPIO-labeled stem cells in animal models of disease can help to determine the optimal timing and location of transplantation. Although SPIO nanoparticles have not been approved by the U.S. Food and Drug Administration (FDA) specifically as intracellular contrast agents, a clinical study that used stem cells labeled with SPIO in patients with neurological diseases was reported by Zhu et al. in 2006 (229); this approach may be adapted to evaluate the therapeutic effects of stem cells in the context of other diseases (165). Most labeling techniques currently use one of two approaches: the attachment of magnetic nanoparticles to the stem cell surface or cell internalization of biocompatible magnetic nanoparticles by endocytosis or phagocytosis (54). However, from a safety perspective, even trivial manipulation of cells prior to implantation might best be avoided (from a regulatory perspective, this is certainly the case).
Despite mounting biological evidence that shows that periodontal regeneration can occur following cell therapy in humans, complete and predictable reconstruction still remains an elusive clinical goal (especially in cases of advanced periodontal defects). Methodologies for the isolation and characterization of stem cells from periodontal tissues were established in 2004 and are a good starting point for understanding the role of stem cells in periodontal healing (23, 182). Implicit in the generative, regenerative, and immunological functions of tissue-specific stem cells is the proper localization of these precursors, which is essential for building organs and tissues during development and fostering localized tissue defense and repair after damage (110). Biologically, although stem cells were originally heralded for their ability to contribute to tissue regeneration through engraftment and long-term survival in injured tissues via their presumed plasticity, recent findings have suggested a plethora of additional mechanisms through which stem cells exert their seemingly beneficial effects, including immunomodulation and paracrine processes (140). However, we have an incomplete understanding of the way that roots develop, and little is known about the signaling mechanisms that occur during this process (201, 224). The molecular pathways that underlie the self-renewal and differentiation of many, if not all, types of stem cells are also largely unknown. It is important to emphasize that animal models can provide a great deal of information about the molecular mechanisms that regulate particular biological processes. In addition, unresolved issues such as the lack of conformity with respect to isolation and ex vivo culture expansion protocols and the heterogeneity by which populations and subpopulations of tissue-specific stem cells are characterized continue to be obstacles. The conflicting data regarding the ability of implanted stem cells to engraft and differentiate into functional PDL fibroblasts, osteoblasts, and cementoblasts, and the numerous studies that report the beneficial effects of stem cells, but only in early time frames, suggest that their benefits are solely attributable to paracrine mediated effects (140). For periodontal regeneration to occur, we need to replicate the key cellular events that parallel periodontal development and to understand the specific cell types, the inductive factors, and the cellular processes involved in the formation of the periodontium (23). New studies provide increasing support for the notion that stem cells in vivo require inputs from particular defined microenvironments, or “niches,” that support unique stem cell functions. Given that the fate of stem cells is influenced by their interaction with the microenvironment (including soluble and immobilized factors, ECM, and signals from neighboring cells), understanding the key components that regulate the properties of stem cells may elucidate ways to expand stem cells properly and control their differentiation precisely (110). Numerous studies assessing the effects of cell therapy have emerged from work on cell culture and in animal models. In the latter case, while some species (e.g., primates) are more suited than others (e.g., mice) for use to understand stem cell behavior in humans, findings from animal studies will not always be directly extrapolated to humans.
Clinical methods for assessing regenerative periodontal treatments are clearly more important than any paraclinical test because the reproduction in humans of results from well-designed, well-controlled, and well-conducted animal studies may be difficult. Currently, outcomes are mainly assessed by clinical parameters such as periodontal probing, radiographs, and reentry evaluations (119, 120). These methods are inappropriate for demonstrating true attachment gain because histology continues to be the only reliable method to evaluate the efficacy of a new therapy aimed at achieving periodontal regeneration. The application of histological examinations in clinical periodontal therapy trials is difficult, if not impossible; well-controlled human histological studies with appropriate controls are hard to accomplish. New robust, reproducible, and specific clinical outcome measures of function, disability, and handicaps in cell-based periodontal therapy warrant further investigation. It is clear that much more work is needed, and evidence from long-term studies is absolutely required to validate the nature of stem cell-based therapy before the development of a genuine “off-the-shelf ” therapeutic product is achievable for periodontal regenerative medicine (175).
To correctly assess the effects of a cell therapy intervention, it is also important to emphasize that the identification of more new and effective biomarkers will provide us with the opportunity to increase our knowledge of periodontal regeneration. Normally, a biomarker is a characteristic that can be objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacological responses to a therapeutic intervention. It is timely for the biomarker industry to expand, and evaluation of potential candidates should be encouraged alongside clinical end-point-driven trials. Successful candidates that perform efficiently and cost-effectively in rapid “rule out” or “rule in” strategies and facilitate the early triage of patients into low-risk and high-risk treatment groups will be quickly integrated into clinical decision-making protocols. Biomarkers that facilitate the choice of the most appropriate cells and enable titration of doses to prevent side effects or to screen for potential cell interactions are likely to be attractive to clinicians.
Safety Issues
The history of the use of stem cells for therapeutic tissue regeneration illustrates that hazards in these novel therapies are twofold: adverse events affect not only the individual patient(s) but also the enthusiasm with which organizations and national regulatory and funding bodies support continuing and future translational endeavors (40, 178). There has, of late, been an increasing appreciation of the potential adverse effects of (and practical reservations concerning) stem cells following a period of predictably and boundlessly enthusiastic claims for stem cell therapies emanating from the scientific community (85). From a regulatory perspective, safety is the primary concern when examining potential new therapeutics that employ cell-based products, although teeth are nonessential for life (119, 212). Similar to many other translational attempts, there are many safety issues associated with the clinical use of ex vivo manipulated stem cells in periodontology, among which ensuring sterility is a priority (40). It is imperative to prevent any potential contamination due to defects in environmental conditions, handlers, culture containers, or raw materials, or cross-contamination with other products prepared at the same production plant (122). Although sterility assays can be adapted from conventional bioprocessing methods, stem cell-based therapies require more stringent safety assessments, especially in relation to the use of nonhuman products such as fetal calf serum (FCS), mouse feeder layers, and/or porcine trypsin (168). The establishment of optimal culture conditions free of potential cross-contamination is relevant in producing clinical grade human stem cell lines and for the performance of basic research that involves the regulation of self-renewal and lineage determination (120). Viruses are another form of contamination that should be tested for before stem cells can be used to treat human disease. Although a donor blood sample can be analyzed for the presence of human immunodeficiency virus, hepatitis B and C viruses, and human T-lymphotropic virus, there is also the possibility of virus contamination from reagents in the cell culture process, particularly if stem cells are grown on animal feeder cell layers or if single, massively expanded cell lines are used to treat many patients (168). Because cell culture medium often requires xenogenic products, an inherent concern is that current cell cultures may not be completely free of pathogens and infectious risks (131). The use of autologous patient serum has been considered as an alternative to FCS, but in vitro studies have shown that sera from aged patients may inhibit cellular function (1). Recently, human platelet lysate has been suggested as a substitute for FCS in the large-scale expansion of stem cells, but the functional capacity of the expanded cells has only been partially explored (34, 65, 177).
One of the main limitations in the clinical use of autologous stem cells is the insufficient number of cells that can be readily isolated from tissues. Because large numbers of cells are generally required for therapeutic efficacy, there is often a need to perform extensive in vitro culturing (168). For example, some autologous strategies may involve weeks to months of ex vivo bioprocessing (51). Timing is an inherent constraint of stem cell-based therapy in clinical practice (20). Prolonged culture of stem cells may increase the risk of cell contamination and has the potential to lead to cellular senescence and genetic/epigenetic changes.
The use of allogeneic stem cells is much less expensive than the use of autologous cells and should limit the ex vivo processing time (41). However, the decision to incorporate allogeneic stem cell-based therapies into routine clinical dental practice requires careful analysis of the risks and benefits associated with the procedure (28). It is important to understand how the immune system will respond to stem cells or their derivatives upon transplantation. If these cells are recognized by the host as “foreign,” the risk of rejection and associated pathologies may be greater than the potential benefit to the patient, especially in the treatment of nonfatal diseases such as periodontitis (168). Generally, the immunogenicity of a human cell depends on its expression of class I and II major histocompatibility antigens, which allow the body to distinguish its own cells from foreign cells (12). In this regard, human leukocyte antigen (HLA) matching may be important in pairing donors to hosts. However, unlike organ transplantation, not all cell-based therapies are used to treat life-threatening conditions, and the selection of HLA-matched donors may limit the extent of clinical application.
Embryonic stem cells (ESCs) are pluripotent stem cells derived from the inner cell mass of the blastocyst, an early-stage embryo. ESCs have attracted special attention by virtue of their unique properties and extraordinary potential in regenerative medicine. Human ESCs express low levels of class I major histocompatibility antigen, which points to a potential way to overcome these problems; however, this expression is upregulated with differentiation (20). Additionally, isolation of the embryoblast or inner cell mass (ICM) results in destruction of the fertilized human embryo, which raises ethical issues (122). A further possible solution to this problem lies in the use of autologous stem cells (from cell/tissue banks) to overcome immune rejection (12, 46).
The production of patient-specific induced pluripotent stem cells (iPSCs) generated by the epigenetic reprogramming of somatic cells through the exogenous expression of transcription factors is now feasible, and the differentiation of autologous iPSCs into cell types desired for transplantation is being explored (35). These cells, just like ESCs, are likely to have a major impact on regenerative medicine because they self-renew and retain the potential to differentiate into all of the cell types of the human body (101, 102). iPSCs are now relatively easy to isolate from somatic cells, and reprogramming can be accomplished by using nonmutagenic technologies, which raises hope for their use in periodontal medicine (48).
Stem cells that are located in vivo in a specialized microenvironment or niche in a range of adult tissues are termed adult stem cells. Compared with ESCs, adult stem cells have a more restricted (multipotent) differentiation capacity and generally give rise to cell types of the resident tissue. Adult stem cells offer several advantages for autologous and allogeneic therapies, including ease of derivation, tissue-specific differentiation potential, extensive but controlled proliferative activity, safety (lack of teratoma formation) and fewer ethical constraints than for embryonic cells (172). Over the last few years, there has been growing optimism in both basic scientists and clinicians toward the clinical application of BMSCs, although they are isolated from numerous other adult tissues including PDL and the pulp, for many disease pathologies. In particular, adipose tissue contains a large number of stromal cells, is relatively easy to obtain in large quantities and thus constitutes a very convenient stromal cell source (149, 205, 206). Tremendous advancements have been made from in vitro and in vivo preclinical studies using MSCs (175). Recent findings relating to the immunosuppressive effects of MSCs both in vitro and in vivo have also raised the possibility of using allogenic stem cells without the need for donor and recipient cross-matching (69, 137, 146, 164, 172). Because significant numbers of stem cells are necessary for clinical use, new technology for long-term cell/tissue cryopreservation is now clinically available; therefore, repeated harvestings for each treatment can be avoided (2). Following the demonstration that human postnatal stem cells can be recovered from cryopreserved human PDL (183), Li et al. proved that after cryopreservation for 1 month, BMSCs showed no altered regenerative capacity compared with freshly isolated BMSCs in the application of periodontal regeneration (116). However, the translational use of autologous and allogeneic stem cells for patient therapy far exceeds what is currently permitted in periodontal regenerative medicine. In terms of cell-based treatments for periodontitis, MSCs derived from dental tissues appear to be the leading candidates; they share common characteristics and are plastic-adherent fibroblast-like cells with trilineage potential to differentiate into chondrogenic, osteogenic, and adipogenic cell types.
Apart from immune rejection by the recipient of allografted stem cells (more a foreseen but unintended consequence than a hazard per se), perhaps the most serious adverse effects of stem cells are tumor formations upon transplantation in vivo (224). Although the increasing number of stem cell types available represents a unique opportunity for periodontal regenerative medicine, this safety concern could block or delay a large number of clinical trials. The need to demonstrate that a stem cell is not harmful represents a necessary hurdle, especially with pluripotent stem cells, which are capable of forming teratomas. The risk of tumorigenesis following stem cell transplantation is a major safety consideration because reliable methods to eliminate undifferentiated ESCs from culture are yet to be established (11), and current preclinical and clinical studies lack long-term follow-up to draw firm conclusions (225). It is likely that the more specific and extensive the therapeutic application, the longer the stem cells may have to remain in vitro. During this extended period in culture, there is a greater likelihood of the occurrence of genetic or epigenetic changes in the stem cells (20, 95). Extensive in vitro proliferation or other manipulation of cells prior to infusion, whatever the source of the cells, may be presumed to carry a greater risk of tumorigenesis than the use of untreated cells, though such a risk has been shown more convincingly for ESCs (47, 128, 173) than for adult stem cells. Improvement in our understanding of the changes that occur during in vitro cell manipulation will better enable researchers to address the risk of tumorigenesis in stem cell therapy.
The short-term and long-term safety of stem cell-based therapeutics in humans is largely unknown, although there have not been any reports of significant adverse reactions thus far. The use of stem cells in regenerative medicine is likely to continue and expand in the near future, and the establishment of a safety or adverse effects body, to which unexpected clinical outcomes can be reported, is encouraged. Until clinical efficacy has been proven, such an institution would be able to assess whether these procedures “do no harm.” Collectively, safety concerns to consider include, but are not restricted to, aberrant cell development and tissue or vehicle contamination with infectious agents or foreign biological and nonbiological substances used in the laboratory processing of the stem cells (40). Secondary diseases should be considered before the implementation of allogenic-based therapies. Overwhelming cell death of the injected cells could potentially impair tissue repair or, in more severe cases, trigger a significant inflammatory response. Therefore, regulatory agencies will have to define new criteria by which to evaluate the risk associated with specific stem cells and their differentiated progeny (122). This process is often delayed because of the difficulty to define what is an acceptable risk/benefit with stem cell-based therapy in a specific pathological condition. It is impossible to address this issue before the clinical application of advanced therapies, including stem cell therapy and tissue engineering. As noted previously in this review, clinical trials play essential roles to clarify key advances and identify hurdles that require deeper investigation. Translational research will improve the likelihood that the use of stem cells will become clinically routine. The application of stem cell therapy in dental practice is still problematic and limited due to various parameters that are not yet under control. Nonetheless, the development of biological approaches for periodontal reconstruction through the use of stem cells is promising and remains one of the greatest challenges in the dental field for the years to come.
When?
Although the enhancement of periodontal regeneration with stem cells derived from dental related tissues is about to become a clinical reality, we are still far from performing routine clinical procedures (81, 143). Many exciting findings have been obtained following stem cell implantation in animal models, but these findings have not yet offered rewards for treating human disease (157). Despite the large amount of interest in this field, no clinical trials have been performed and very limited clinical applications are available in stem cell-based periodontal disease treatment (52, 89, 119, 134). Given the explosion of research on stem cell therapies for regenerative medicine, two frequent questions are as follows: when should stem cell treatments begin to be tested in patients and when might we witness successful clinical application(s) of those stem cells in the treatment of degenerative diseases such as periodontitis (28)? Clearly, any answer must be subjective, and as other reviews in the literature indicate (21, 85, 119, 212, )224, some such studies are already underway. The brief consideration outlined above of the practical issues does allow a personal view. In the specific case of the autologous infusion of unmanipulated dental tissue-derived stem cells, we believe we already have sufficient information to move into the clinical arena (38, 52, 134, 217, 218), and indeed, we have commenced a small-scale pilot/feasibility study in China.
Stem cell-based approaches have opened up the possibility for the development of a restorative treatment for large numbers of patients with moderate/severe periodontitis. On the basis of the available experimental and preclinical data (15, 41, 43, 44, 145, 155, 207, 213, 219, 221), it is now possible to define a road map that includes the main steps toward the clinical application of stem cells in patient periodontal therapies (Fig. 5). Given the outcomes of preclinical research, we have already approached the final stage of the blueprint (clinical studies), although much more still can be achieved throughout the road map (Table 1).

There are five main (nondefinitive) steps and their dynamic feedback in translational research to determine cell-based therapies for clinical use in periodontal regenerative medicine (PDL, periodontal ligament). Safety and efficacy may change during the translational research process (from in vitro to in vivo, from animal to human), and so continual feedback will be needed to improve the design of a stem cell-based therapy from bench to bedside.
In terms of the successful clinical practice of cell therapy, we would be foolish to ignore that extensive experience in the collection and delivery of bone marrow cells offers an invaluable endorsement of this form of potential cell therapy for leukemia patients. There exists an efficient, effective, and highly evolved clinical infrastructure that includes practical techniques for cell harvesting and infusion, dedicated transplant units, controlled and approved cell-handling facilities, and streamlined and user-friendly patient pathways. Added to this is experience that offers reassuring long-term safety data following autologous mesenchymal cell infusion, information that has now been amplified by the increasing experience of cardiologists in the use of bone marrow cells to aid cardiac repair (8, 124, 125, 159, 176, 192), and the longer-term data that are emerging from other branches of (mostly oncological) medicine (92, 106, 200). Provided that intravenous rather than intraparenchymal delivery is first used, the cells are autologous and are not manipulated prior to reinfusion, and the treatment takes place in a clinical environment experienced in bone marrow transplantation, it is difficult to envisage any predictable adverse effects.
Nonetheless, unpredictable consequences are by no means impossible, and early clinical work to treat nonlifethreatening diseases such as periodontitis must commence with small-scale pilot studies that only recruit individuals who have already accrued some measure of progressive periodontal disease (217). At this stage of development, most clinicians would most likely argue that the periodontal reconstruction of cell therapy in animals is unlikely to transfer to clinical regeneration in patients and that even the potential benefit most likely does not outweigh the cost, effort, and risks of a large-scale clinical trial (59, 84). Keeping this in mind, it seems that we are far from using the full potential of stem cell therapy in the treatment of periodontal disease. As outlined elsewhere, we are aware that there is already a significant body of work that attests to the potential efficacy of these cells in periodontal defect models (38, 52, 134). The mechanisms are by no means clear, but it can be argued that a complete understanding of modes of action is not an absolute prerequisite for the introduction of new treatments. For example, we still do not know how interferons work in multiple sclerosis or how immunoglobulins work in inflammatory neuropathies, but these therapies have already delivered substantial benefits for patients. Questions of cell delivery, cell numbers, preferred state of differentiation, and the optimum phase of the disease can most likely only be answered by future clinical studies in patients—not by basic research or experimental studies. These considerations, particularly the safety aspects, indicate that it is better to commence a small study of locally delivered autologous PDLSCs in a small group of patients with chronic periodontitis, with clinical and biological assessments before and after infusion (38, 52, 134). In terms of periodontal regeneration, a report of three cases that used PDL progenitors for in vivo periodontal tissue regeneration has demonstrated clinical and experimental evidence that supports the potential efficacy and safety of the use of autologous PDL cells in the treatment of human periodontitis (52). Keeping this in mind, we hope to present a call for action to develop more clinical studies that introduce these therapies for clinical use.
Over recent years, there has been increasing interest in funding opportunities for initiatives that aim to bridge the “translational gap” between basic and clinical research, where a common buzzword is “translational medicine” (28). We have all heard it: it is what the national institutes are funding, it is what scientific congresses advocate, and it is what the clinician/patient/public wants. To obtain funding support, basic scientists must demonstrate and articulate how their research findings can lead to the improvement of human health. As periodontists, we are fortunate because we study an area that is inherently interesting to most people. Many of us engaged in translational medicine long before the term became fashionable, such as with the development of EMD and the introduction of GTR and PRP biotechnology for periodontal therapies (6, 70, 169, 180, 222). We have pursued an area of research that will someday lead to the development of new advanced therapies, whether pharmacological, biological, or genetic, to treat periodontal disease. It is well recognized that translational research is an iterative or cyclic process: the bedside-to-bench component is just as important as bench-to-bedside (28). Research from the clinic should be available to the scientists that develop animal models so that they can improve the relevance of their model to the human condition (or at least better understand its limitations). Translational research requires expertise in many different areas, which means that teamwork is required. Collaborations should be forged at the earliest stages of project planning so that basic scientists working at the bench can plan the most relevant experiments and clinicians can harness the best and newest techniques to maximize the information they collect from their patients.
Future Perspectives
Periodontitis is an inflammatory disorder with widespread morbidities that involve both oral and systemic health. In the face of mounting clinical demand and armed with reconstructive techniques that are technically challenging and frequently result in suboptimal patient outcomes, increasing focus is being placed on tissue engineering and regenerative medicine as potential sources of novel periodontal reconstructive approaches. Built on emerging discoveries in stem cell biology, cell transplantation therapies have begun to define the scope of future clinical practice (23, 25, 26, 28). Specifically, evidence is accumulating that highlights the potential of stem cell-based reconstructive strategies to overcome the limitations associated with existing periodontal therapies and their promise to meet the needs of an expanding patient population (119, 185, 212). The use of stem cells in the clinical arena has gathered tremendous momentum over the last decade, advanced with varying levels of success in clinical trials for several pathological conditions, and increased our understanding of the mechanisms by which stem cells exert their seemingly favorable effects on the predictable regeneration of supporting alveolar bone, PDL, and cementum. Although there are several barriers that need to be broken down before this novel therapy can be translated from the lab to clinics for routine dental care, it is certain that the future is going to be exciting for periodontists and their patients. Our current need is high-quality translational research coupled with collaboration between basic scientists and clinicians. It is of paramount importance that our clinicians who aim to undertake stem cell therapies understand the potential risks following cell transplantation and the associated regulations that are established for the control of stem cell therapies (40, 122, 224).
With the emergence of the first reports that adult human stem cell populations reside in the PDL and recent advances in their in vitro and in vivo manipulation (50, 67, 91, 108, 142, 196), the next phase will be to determine the clinical utility of these cells. Although ex vivo cell culture is thought to be elaborate and costly, especially under good manufacturing practice (GMP) conditions, there is tremendous scope for using cell delivery therapeutics for the regeneration of dental systems. The safety and efficacy of cell-based therapies have been demonstrated in large-scale human studies in some cases (such as for the repair of bone and cartilage, in phase I clinical trials) and have therefore been advanced to broad clinical applications (14, 108, 196). However, cells have only been used experimentally in other related arenas (e.g., in dentistry for tooth and periodontal repair). Dental diseases are generally not life-threatening, so safety will be a key issue for any clinical application of stem cell therapy in this field. However, available cell-based therapy strategies based on tissue engineering approaches have solid backgrounds for clinical application in human periodontal defects (170). Once safety issues are addressed satisfactorily, we speculate that stem cell therapy is likely to be added to the dental armamentarium in the near future (119). Before these exciting clinical prospects can be realized, much more still needs to be done to determine how to refine current delivery technology, to identify both the essential stem cells that determine the fate of periodontal tissue and the criteria to establish dosing, to promote long-term survival and integration of stem cells upon transplantation, and to develop tailored cell-based products for each pathological situation (119, 224).
In terms of periodontal reconstructive therapy, cellular therapy remains in the early stages of development but holds promise as a means to restore function after periodontitis. Stem cells have emerged as the starting material of choice for bioprocesses to produce cell and tissues to treat myriad degenerative, genetic, and immunological diseases including periodontal disease. Bioprocessing and commercialization of stem cell/tissue-engineered products in regenerative medicine can translate breakthroughs from the research bench to the patient's bedside. However, translating the biological properties and potential of stem cells into therapies will require overcoming significant cell-manufacturing and regulatory challenges (101, 102). As noted previously in this article, completely successful translation of the stem cell from its context of developmental biology into the adult context of periodontal injury and disease is likely to rely on new insights into the biology of periodontium development and repair. Such insights are required to enhance protocols for the isolation of demonstrably effective stem cell populations and their robust ex vivo expansion in chemically defined conditions.
In the majority of cases, stem cells are used to deliver a space-filling entity via a biomaterial to repair an injured tissue, although in some cases they have been beneficial by themselves (injection/infusion). Scaffold design is likely to play a critical role to bridge the gap between the stem cell and the clinic. Parameters pertinent to stem cell biology that involve the dynamic transmission and/or attenuation of biological, chemical, and mechanical signals will need to be optimized and joined with parameters pertinent to clinical application, such as ease of delivery to the site of injury and use of dynamically durable/degradable 3D structures (45, 126, 130, 199). Process characterization and optimization is the key for any bioprocess. Standardized operating procedures and know-how must be available for a process to be translated into a manufacturing operation. Improvements in the currently available process monitoring systems for bioreactors should be made so that nutrients and metabolites can be monitored continuously and in real time. Future challenges in bioprocessing and manufacturing will include the development of advanced and sophisticated monitoring platforms that allow monitoring at the cellular level (162, 168). Completely integrated, modular, automated, and controlled systems in a fully enclosed bioprocess operation from harvest to delivery will need to be considered. In the view of the authors, scale-up of stem cell/tissue-engineered bioprocesses can be achieved by small-scale modular systems operating in an “in series and in parallel” mode in which overcapacity is considered and the whole process is addressed as a supply chain model. Scale-up can be delivered by lower infrastructure cost systems where integration, modularity, and parallel operation are key (162).
Conclusions
Dentistry is entering an exciting era in which many of the advances in stem cell biology and tissue engineering offer opportunities for the exploitation of novel and more effective regenerative therapies. As discussed in this review, these times are exciting for the field of periodontal regenerative medicine. The current challenge is to harness the regenerative capacity of the periodontium via the development of multidisciplinary approaches that integrate developmental and engineering processes with cellular, molecular, biochemical, and clinical techniques. The rewards of improving quality of care and reducing healthcare costs in an increasingly aged population are immense. The clinical applications of stem cells in periodontics are gradually becoming a reality, and future practices will continue to require a team effort that engages the expertise of molecular biologists, biomaterials scientists, cell biologists, periodontal surgeons, regulatory agencies, and, most importantly, clinical patients. The initiation of clinical trials seems to be the only route that may accelerate the clinical implementation of stem cell therapy and expedite the clinical development of cell therapy products.
Footnotes
Acknowledgments
Funding from the National Natural Science Foundation of China (81071253, 81201205, and 31170912) for some of the work mentioned in the article is gratefully appreciated. This work is supported by Program for New Century Excellent Talents in University (NCET2012). The authors wish to acknowledge the contributors in this field and their work summarized in this review. The authors report no conflicts of interest, and they are responsible for the content and writing of the paper.