
Abstract
Grafts from non-heart-beating donors (NHBDs) are used because of the limited availability of heart-beating brain-dead donors. These grafts sustain ischemic damage, and the severity of this damage varies among different areas of an organ. This study determined whether the results of islet isolation were correlated with the clinical outcomes of kidney transplantations in cases where both grafts were harvested from the same NHBD. Islets we isolated from the pancreata of 23 NHBDs between February 2004 and March 2007. Forty-six kidneys were also harvested from these NHBDs. The recipients of kidney transplants were divided into the successful isolation (n = 14) and failed isolation (n = 32) groups depending on the results of islet isolation. The clinical outcomes of kidney transplantation were compared between the recipients in these two groups. The immediate graft function rate and the 1-year graft survival rate after kidney transplantation in both groups were similar. Hemodialysis after transplantation was required for 6.0 days (SD, 5.2 days) in the successful isolation group and for 12.7 days (13.1 days) in the failed isolation group (p < 0.05). The serum creatinine concentrations at 1, 3, 6, and 12 months after transplantation were elevated in the failed isolation group (p < 0.05). The islet yield was inversely correlated with the requirement of hemodialysis (days) and the serum creatinine level at 1 month after transplantation. However, hemodialysis was required for only 7 days in the recipients of six kidneys that were obtained from NHBDs from whom <40,000 IEQ were obtained (extreme failure of islet isolation). The results of islet isolation were found to correlate with the kidney function after transplantation when both grafts are harvested from the same NHBD. However, the marginal conditions of NHBDs affect the results of islet isolation more than they do the posttransplantation kidney function.
Introduction
Grafts from non-heart-beating donors (NHBDs) are now used for kidney, pancreas, liver, and even lung transplantation because of the limited availability of heart-beating brain-dead donors (3). Grafts from NHBDs sustain ischemic damage before and after cardiac death, and the severity of this damage may vary among the different areas of an organ. Islets are usually not harvested from heart-beating brain-dead donors in Japan. NHBDs are the only source of islets for transplantation. The technique of procuring pancreatic grafts and isolating islets from damaged pancreatic grafts has been improved (5) and has yielded promising results: 7 of 23 isolations (30.4%) were successful. The results of islet transplantation were compared with the clinical outcomes of kidney transplantation in cases where both grafts were obtained from the same donor. This study was undertaken to determine whether the clinical outcomes of kidney transplantation could be predicted on the basis of the results of islet isolation.
Materials and Methods
This study retrospectively analyzed the isolation islets from 23 pancreata and the transplantation of 46 kidneys harvested from the same NHBDs between February 2004 and March 2007. All the NHBDs had sustained serious brain injuries such as intracranial hemorrhage, trauma, and hypoxia, but did not meet the diagnostic criteria for brain death or the criteria for organ donation upon brain death (in Japan, donation from brain-dead donors is strictly regulated by law). The aorta was cannulated before the occurrence of cardiac arrest in 13 donors. Withdrawal of ventilatory support prior to cardiac arrest was performed in only two donors; cardiac arrest occurred prior to the withdrawal of ventilatory support in the case of the other donors. The abdominal aorta was perfused with cold University of Wisconsin (UW) solution or Euro Collins (EC) solution after the declaration of death if the cannulation had been performed before death. If not, the donor was transferred to the operating room, and closed chest massage was performed until the operation was initiated. A laparotomy was then performed, and the abdominal aorta was cannulated from the iliac artery and perfused with cold UW solution or EC solution. Crushed Ringer ice was placed around the kidney and into the omental sac to facilitate local cooling of the kidney and pancreas. The pancreatectomy was performed after the removal of both kidneys. The warm ischemic time (WIT) was defined as the interval from cardiac arrest to the start of cold perfusion. The cold ischemic time (CIT) of the kidney was defined as the time from the start of cold perfusion to reperfusion with an arterial flow in the recipient. The CIT of the pancreas was defined as the time from the start of cold perfusion to the injection of collagenase into the pancreatic duct.
Seventeen pancreata were preserved using a two-layer method (6,8), and six pancreata were preserved by simple storage in cold UW solution. Islets were isolated in the cell-processing center in accordance with the Edmonton protocol (10). In brief, the pancreatic duct was cannulated and perfused with cold Liberase solution (Liberase HI; Roche Diagnostics, IN, USA). The pancreas was enzymatically and mechanically dissociated and purified in Euro-Ficoll solution with a discontinuous gradient by using a refrigerated COBE 2991 Cell Processor. The standard islet diameter was assumed to be 150 μm, and the islets were counted twice (9). Islet isolation was considered successful if more than 200,000 islet equivalents (IEQ) with a purity of >30% were recovered after islet purification.
Furthermore, 46 kidneys were harvested from the 23 NHBDs from whom the pancreata were collected using the procedure described above. The recipients of the kidneys were administered immunosuppressive therapy of a calcineurin inhibitor (cyclosporin or tacrolimus), antimetabolites (azathioprine or mycophenolate mofetil), and corticosteroids along with induction therapy involving anti-CD25 monoclonal antibody (basiliximab). The immediate kidney function after transplantation was defined as whether or not there was a need to perform hemodialysis after transplantation. All clinical data related to the kidney transplantations were deposited with the Japan Organ Transplantation Network.
The Institutional Review Board at NHO Chiba-East National Hospital approved all protocols.
The two-sided unpaired t-test or the Mann-Whitney test was used to compare the groups, as appropriate. Pearson's correlation coefficient test was used to evaluate any correlations among the factors.
Results
Donor Characteristics
The median age of the 23 NHBDs was 44.0 years (range 14–69 years). A total of 10 donors (43.5%) died of cerebrovascular disease; seven of brain edema after hypoxia; five of trauma; and one of brain tumor. Cardiac arrest occurred before arrival at the hospital in eight donors. The median serum creatinine concentration was 122 μmol/L (range 53–896 μmol/L), and the median hospital stay was 9 days (range 2–84 days).
Islet Isolation
The median WIT and CIT of the pancreata were 5 min (range 1–30 min) and 309 min (range 211–540 min), respectively. The median weight of the pancreas was 92 g (range 37–134 g). The islet yield and purity were 126,740 IEQ (range 0–369,427 IEQ) and 40% (range 1–80%), respectively. Islet isolation was successful in seven cases, and the harvested islets were used for transplantation in six of these seven cases. Islets could not be harvested, had to be discarded, or were cryopreserved in the remaining 16 isolations. The recipients of kidney transplants were divided into the successful isolation (SI) and failed isolation (FI) groups depending on the results of islet isolation (Table 1).
Islet Isolation Characteristics

WIT, warm ischemic time; CIT, cold ischemic time; IEQ, islet equivalents. N.S., not significant.
Clinical Outcomes of Kidney Transplantation
The overall graft survival at 12 months after transplantation was 87.0%, that in the SI group was 85.6%, and that in the FI group was 87.5%. The difference between the groups was not significant. The immediate graft function rate was 21.4% in the SI group and 6.25% in the FI group (N.S.). Hemodialysis was required for 6.0 days (SD 5.2 days) in the SI group and 12.7 days (13.1 days) in the FI group (p < 0.05).
The mean serum creatinine concentrations in patients with functioning grafts at 1, 3, 6, and 12 months after transplantation were elevated in the FI group in comparison with the SI group (p < 0.05). These values were 92.8, 95.5, 98.1, and 93.7 μmol/L in the SI group and 205.1, 146.7, 149.4, and 147.0 μmol/L in the FI group (Fig. 1).

Serum creatinine concentration after kidney transplantation. Light columns: successful isolation group; dark columns: failed isolation group.
Correlation Between the Islet Yield and Clinical Outcome of Kidney Transplantation
The islet yield (IEQ) was inversely correlated with the number of days for which hemodialysis was required (Fig. 2A) and with the serum creatinine concentration at 1 month after kidney transplantation (Fig. 2B).
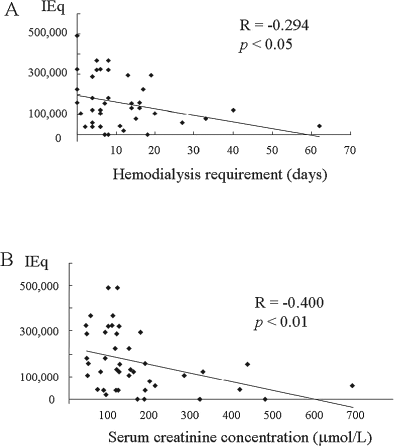
Relationship between the islet yield (IEQ) and hemodialysis requirement (A), and serum creatinine concentration 1 month after kidney transplantation (B).
Discrepancy Between the Islet Yield and Clinical Outcome of Kidney Transplantation
Hemodialysis was required for only 7 days in six recipients of kidneys that were obtained from NHBDs from whom <40,000 IEQ were obtained (extreme failure of islet isolation). The conditions of the donors from which these grafts had been harvested were extremely poor. These donors had undergone cardiopulmonary resuscitation, received high doses of catecholamines, or had high serum creatinine concentrations (Table 2).
Discrepancy Between the Islet Yield and Clinical Outcome of Kidney Transplantation

CPR, cardiopulmonary resuscitation; SAH, subarachnoid hemorrhage.
Discussion
This study presents the relationship between the results of islet isolation and the clinical outcomes of kidney transplantation in cases where both the islet grafts and kidneys are harvested from the same NHBD. The antemortem conditions of the NHBDs varied. Even in the case of heart-beating brain-dead donors, the results of islet isolation depend on several factors (1). The condition of grafts obtained from NHBDs is worse than that of grafts obtained from heart-beating brain-dead donors because of severe warm ischemic damage. Nevertheless, pancreata harvested from NHBDs are now used for islet transplantation owing to the improvement in islet procurement and isolation techniques (7). NHBDs are an important source of kidneys for transplantation. Some large series of kidney transplants recovered from NHBDs have been reported (2,11,12). However, this is the first report to describe the relationship between the results of islet isolation and the clinical outcomes of kidney transplantation in cases where both grafts are obtained from the same donor.
In general, patients who receive kidneys from NHBDs experience long periods of oliguria and require prolonged hemodialysis (2). A large-scale single-center study reported that recipients of grafts obtained from NHBDs experience significantly higher rates of delayed graft function than the recipients of grafts obtained from heart-beating brain-dead donors. Further, the serum creatinine levels in the former recipients are elevated for 7 days after transplantation. However, no measurable difference is observed between the recipients of grafts from NHBDs and those of grafts from heart-beating brain-dead donors by the end of the first postoperative month (12). In this study, patients in the FI group required hemodialysis for longer periods than those in the SI group. Furthermore, the islet yield was inversely correlated with the number of days for which hemodialysis was required. The serum creatinine concentration after kidney transplantation was better in the recipients in the SI group than those in the FI group. Therefore, good results of islet isolation predict a good clinical outcome of kidney transplantation in cases where the kidneys and pancreas are harvested from the same donor. However, in some cases, the results of islet isolation and the clinical outcomes of kidney transplantation were discrepant. Even though the results of islet isolation were very poor in three cases (<40,000 IEQ harvested), the recipients of kidney transplants required hemodialysis for only 7 days. The condition of the donors of these grafts was extremely poor. These donors had undergone cardiopulmonary resuscitation and received high doses of catecholamines. Many think that stringent criteria must be used for the selection of NHBDs for pancreata (4). The pancreatic function is thought to be more severely affected by warm ischemic damage than the kidney function.
In conclusion, the results of islet isolation were observed to correlate with the outcomes of kidney transplantation in cases where both grafts are harvested from the same NHBD. However, the results of islet isolation are more severely affected by the marginal conditions of NHBDs than are the functions of transplanted kidneys. It is therefore difficult to predict the clinical outcomes of kidney transplantation based only on the results of islet isolation.
Footnotes
Acknowledgments
The authors wish to thank Mr. Tomonori Saito, Ms. Mariko Miyazaki, and Ms. Akiko Suzuki for their valuable technical support. This study was supported in part by a Grant-in-Aid from the Ministry of Education, Science and Culture. The authors declare no conflict of interest.