
Abstract
Preliminary results were measured by electromyography monitoring (electromyoscan) on three subjects suffering from spinal cord injury and who underwent a double therapy. The aim of this study was to evaluate regained voluntary activity below the injury in subjects who received a double therapy: 1) an olfactory ensheathing glia (OEG) transplantation using procedures developed by Dr. Hongyun Huang at the Xishan Hospital and Rehabilitation Centre, Beijing, China, and 2) LASERPONCTURE® developed by Albert Bohbot, Laboratoire de Recherches sur le LASERPONCTURE®, La Chapelle Montlinard, France. Materials uses were the LASERPONCTURE® device developed by Albert Bohbot; the PROCOMP5™ equipment with softwares BIOGRAPH INFINITI 5® and REHAB SUITE™; the sensors MYOSCAN-PRO™ EMG (SA9401M-50) to record muscle activity, and FLEX/PRO™-SA9309M to record skin conductance were fixed on the skin. An infrared laser, whose frequencies and power settings cannot be disclosed due to its proprietary nature, was applied after an OEG injection performed according to Dr. Hongyun Huang's procedures. Three cases, two males and one female, were selected for this study. Presentation and comments of the graphs recordings of voluntary muscle activity below the injury are provided. This preliminary study suggests that the double therapy restores some voluntary muscle activity as measured by electromyography monitoring.
Keywords
Introduction
The aim of this preliminary pilot study was to evaluate regained voluntary activity below the injury in subjects with spinal cord injury (SCI) who received a double therapy: 1) an olfactory ensheathing glia (OEG) transplantation using procedures developed by Dr. Hongyun Huang at the Xishan Hospital and Rehabilitation Centre, Beijing, China, and 2) LASERPONCTURE® developed by Albert Bohbot, Laboratoire de Recherches sur le LASERPONCTURE®, La Chapelle Montlinard, France, where more than 500 SCI individuals have already received this technique. The restored voluntary activities were confirmed by electromyography monitoring. OEGs were transplanted in three individuals with SCI using the procedures developed by Dr. Hongyun Huang (9–12). An animal study suggested that transplanted olfactory ensheathing cells may ameliorate the functional deficits associated with injuries to the nervous system, especially the spinal cord (7).
All three cases later underwent LASERPONCTURE® therapy. The procedure consisted of applying 10 infrared laser heads that are computer-piloted and fixed either on the front or on the back of the subject. The frequency was two sessions of 20 min every day, one in the morning and one in the afternoon. Laser heads were not necessarily applied on the injury. Other studies have documented the potential function-restoring benefits of combining cell transplantation with laser irradiation either on humans or animals (5,6,8).
Materials and Methods
Material
The LASERPONCTURE® device was developed by Albert Bohbot with the assistance of the French engineering school École Nationale des Arts et Métiers, and funded by Bourgogne Innovation, a public agency, and the Laboratoire de Recherches sur le LASERPONCTURE®. Due to its proprietary nature, specific frequencies and power settings of the LASERPONCTURE® device cannot be disclosed as well as the accurate charts illustrating where the laser heads are fixed.
The softwares BIOGRAPH INFINITI 5® and REHAB SUITE™ of the PROCOMP5™ equipment were modified by us to fit these specific type of examinations and subjects. Muscle sensors MYOSCAN-PRO™ EMG (SA9401M-50) were fixed on the surface of the skin with hypoallergenic adhesive disks. Electromyography monitoring records muscle activity without sending any electrical impulse. It is an exterior measurement of underlying muscle activity.
Procedures
Informed consent was obtained from the patients in this study and the Ministry of Health of the Popular Republic of China approved the procedure.
The laser heads are principally applied on the pathways of the following acupuncture meridians: stomach, kidney, Ren Mai, and Dai Mai on the front; Chong Mai, bladder, Dai Mai, and extraordinary points on the back. The laser heads are placed on meridians and also on points that are not part of the classical acupunctural network but situated on dermatomes. A chart of laser-head placement could be read longitudinally and horizontally. For example, five laser heads (Fig. 1) could be placed longitudinally (meridians) on a line going from the sternum to the umbilicus, and the five other laser heads could be placed on each side of this line delineating horizontal lines (dermatomes). The areas outside the acupunctural network correspond to the dermatome chart as established by the American Spinal Injury Association scale. The muscle sensors (Fig. 1) were fixed at 15 cm from the upper edge of the patella and on the anterior face of the quadriceps. Muscle contractions were recorded in microvolt, and skin conductance (Fig. 1) was recorded in microsiemens with a FLEX/PRO™-SA9309M sensor. The skin conductor sensor was fixed at level T10 by measuring three fingers from each side of the umbilicus. The graphs in Figures 2, 3, and 4 show the activity in the tested muscles on the left-hand side and right-hand side using an arithmetic subtraction. Above 0 are the muscles on the right-hand side; below 0 are the muscles on the left-hand side.
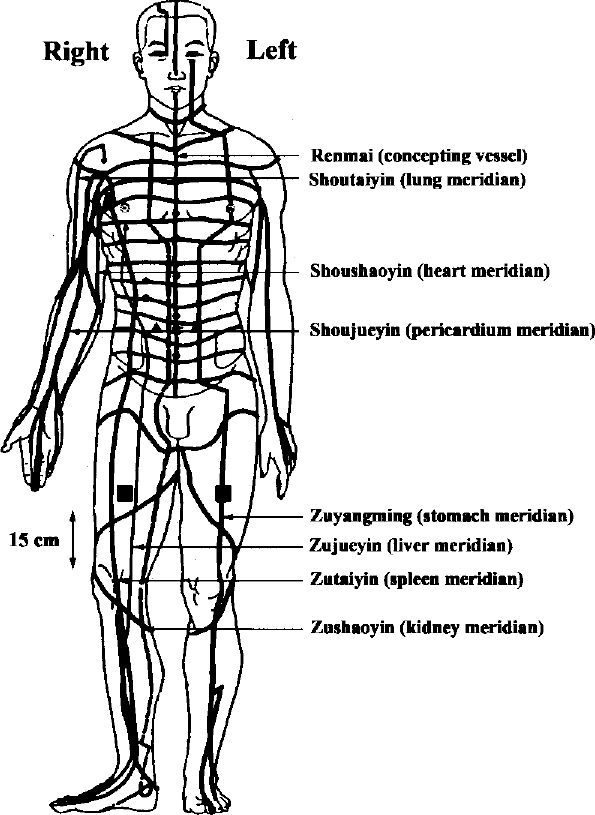
Location of sensors and lasers on a schematic figure of the acupuncture meridians of the human body. Circles: placement of the laser heads, squares: muscle sensors, triangles: skin conductance sensors.

Difference in muscle strength contraction between the right quadriceps and left quadriceps in case 1 from 00:02: 35 to 00:02:45 with LASERPONCTURE® measured in microvolt by electromyography monitoring.
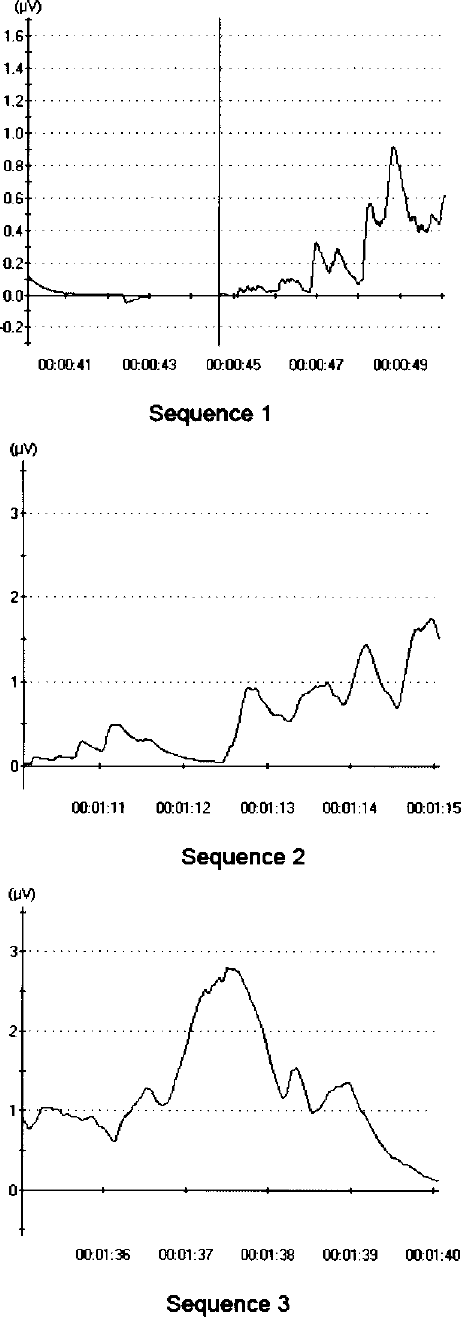
Differences in muscle strength contraction between the right and left quadriceps of case 2. Sequence 1: difference of muscle strength contraction between right quadriceps and left quadriceps from 00:00:40 to 00:00:50 without LASERPONCTURE® measured in microvolts by electromyography monitoring. Sequence 2: difference of muscle strength contraction between right quadriceps and left quadriceps from 00:01: 10 to 00:01:15 without LASERPONCTURE® measured in microvolts by electromyography monitoring. Sequence 3: difference of muscle strength contraction between right quadriceps and left quadriceps from 00:01:35 to 00:01:40 without LASERPONCTURE® measured in microvolt by electromyography monitoring.
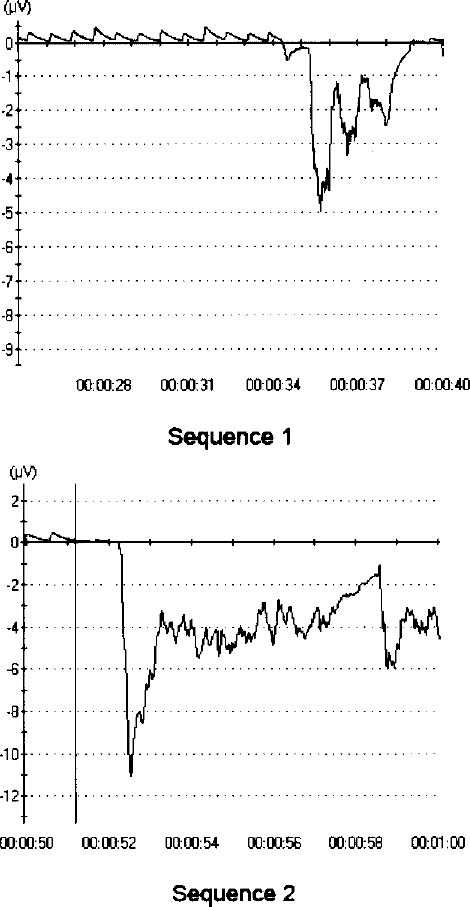
Differences in muscle strength contraction between the right and left upper abdominal muscles of case 3. Sequence 1: difference in muscle strength contraction between the right upper abdominal muscle and the left upper abdominal muscle from 00:00:25 to 00:00:40 with LASERPONCTURE® measured in microvolts by electromyography monitoring. Sequence 2: difference in muscle strength contraction between the right upper abdominal muscle and the left upper abdominal muscle from 00:00:50 to 00:01:00 with LASERPONCTURE® measured in microvolt by electromyography monitoring.
Case 1 is a 25-year-old man injured on September 22, 2006, at level T7 (MRI, Fig. 5). On January 8, 1 million OEGs and 2 million embryonic brain cells (enriched with neural stem cells) were implanted into the spinal cord in a volume of 100 μl. Based on his hospital report, on January 13, 19, and 23, he had an intrathecal injection of 2 million fetal brain cells of 500 μl: 2,000,000 embryonic brain cells (enriched with neural stem cells). Starting on March 2, 2009, a total of 57 LASERPONCTURE® sessions were cumulatively carried out.

MRI of the spinal cord of case 1; the white circle highlights the injury site.
Case 2 is a 32-year-old woman injured on August 26, 2008, at level T4-T5 (MRI, Fig. 6). On September 23, 2008, 1 million OEGs and 2 million stem/progenitor/precursor cells were injected in the spinal cord in a volume of 100 μl. Starting on March 2, 2009, a total of 40 LASERPONCTURE® sessions were cumulatively carried out.

MRI of the spinal cord of case 2; the white circle highlights the injury site.
Case 3 is a 37-year-old man injured on February 11, 2006, at level T9 (MRI, Fig. 7). Dr. Hongyun Huang's therapy was performed on November 28, 2008; no transplantation details were available for case 3. Starting on January 12, 2009, a total of 57 LASERPONCTURE® sessions were cumulatively carried out.

MRI of the spinal cord of case 3; the arrow shows the injury site.
Results
The analysis of the graphs for the three cases studied suggests that there are voluntary muscle contractions. In the first case study, the contraction of the right quadriceps is stronger than the left (Fig. 2). In the second case study, the graphs also suggest that the right quadriceps is stronger with high contractions between 00:00:47 and 00:00:49 min (sequence 1 in Fig. 3) (period during which voluntary orders are sent), between 00:01:11 and 00:01:15 min (sequence 2 in Fig. 3), and from 00:01:36 to 00:01:40 min (sequence 3 in Fig. 3). In the third case study, significant contractions on the left-hand side occurred between 00:00:34 and 00:00:40 min (sequence 1 in Fig. 4), and between 00:00:52 and 00:01:00 min (sequence 2 in Fig. 4).
The aim of LASERPONCTURE® is to promote or enhance the passage of information through the area of injury. If an OEG transplantation helps tissue restructuring, LASERPONCTURE® helps the passage of the orders sent from the brain to the areas below the injury through an electromagnetic wave, and not through an electrochemical conduction. Therefore, it complements the spinal tissue restructuring. In a paradigm-expanding assumption, we believe that the nerve impulse may be mediated either through a biochemical conduction using neurotransmitters or through electromagnetic channels using a wavelength (1–4,13,14).
Discussion
The aim of this preliminary study was to evaluate whether OEG transplantation followed by LASERPONCTURE® may restore some ability to voluntarily contract paralysis-affected muscles. Two men and a woman were evaluated. All three underwent Dr. Hongyun Huang's OEG transplantation treatment followed by a series of LASERPONCTURE® sessions. A LASERPONCTURE® session lasted 20 min and was performed twice a day over a 5-day course, representing 10 sessions a week. At least 8 weeks between two sets of sessions were required.
The different graphs obtained suggest that there is a voluntary muscle activity below the injury. It also suggests that there are some motor recovery processes.
Dr. Hongyun Huang's procedure and Albert Boh-bot's technique have proven to give results separately. A combination of circumstances made that both were combined within the clinic performing LASERPONCTURE®.
The three cases selected for this study successively received Dr. Hongyun Huang's OEG transplantation first, followed by the LASERPONCTURE® technique a few months after. It seems that the positive effects of the two techniques, added to each other, suggest that recoveries seem to appear quicker. Data from the electromyography monitoring seem to confirm this hypothesis.
Conclusion
The results suggest that the combination of both OEG transplantation and LASERPONCTURE® restores some voluntary activity in the tested muscles below the injury in individuals suffering from complete paraplegia.
Footnotes
Acknowledgments
The author thanks Isabelle Aygalenq for the imaging, Laurance S. Johnston for his advice, and Edwige Nault for the translation.