
Abstract
BACKGROUND:
Computers are ubiquitous in the workplace and facilitate prolonged sitting, which has adverse health consequences. Various computer-prompt software programs are designed to decrease sedentary behaviors and increase physical activity in the workplace. However, specific guidelines that would improve research in this area have not been published.
OBJECTIVE:
The objective of this article is to present recommendations for improving computer-prompt software research, to decrease sedentary behaviors and increase physical activity in the workplace.
METHODS:
Ten domains were identified based on deficiencies in the current literature combined with quality assessment tools to reduce the risk for bias. The ten domains include composition of the research team, behavioral sciences theoretical frameworks, research design, alert types, outcome measures, confounding factors, intervention duration, carryover effects, racial/ethnic composition, and organizational culture.
RESULTS:
Specific recommendations are presented for each domain. The research team should include all stakeholders contributing as copartners in designing the intervention. For theory, a systems science framework was presented. Clustered randomized controlled trials were recommended, rather than randomization at the individual level. Distinct types of alerts (visual, auditory, or both) and frequency of alerts (hourly, randomly generated, or based on prolonged sitting patterns) are described. Outcome measures include average duration of sitting bouts, longest sitting bout, and number of sitting bouts.
CONCLUSION:
Prolonged sitting and physical inactivity at work lead to major health problems. Adherence to the recommendations presented here should facilitate high-quality research and improve the health of desk-based workers by decreasing sedentary behaviors and increasing physical activity.
Introduction
Computers are ubiquitous in today’s workspaces, including traditional offices, home offices, and coworking spaces. It is estimated that more than 50% of workers in the United States are required to spend part of their workday at a computer [1], given that computers are a requirement for almost every kind of office task, from email communication to document production, presentation development, and so on. As such, computers are one of the main culprits facilitating prolonged sitting.
Sitting has been characterized as the “new smoking” because of its adverse health consequences. Evidence suggests that sedentary behaviors are distinct health behaviors that have their own risks and are not simply the absence of physical activity [2]. For example, prolonged sitting increases the risk for obesity, type 2 diabetes, metabolic syndrome, cardiovascular disease, and premature mortality, even when moderate-to-vigorous physical activity is accounted for [3— 7].
Ironically, a computer that facilitates prolonged sitting can also be used to interrupt this health hazard. Computer-prompt software programs can sound an alarm or present a visual cue on the screen every 30 or 60 minutes. These alerts are a signal to stop working and “get up and move” or “walk the hallways and climb the stairs” [8— 10]. Some software programs will even lock the keyboard and provide educational messages. These programs are simple, easy to install, and low-cost or free; they need no ergonomic adaptations, can be equitably distributed, and are user friendly, requiring minimal practice [11, 12]. Frequent interruption of sitting has been linked to a range of improved health indices [13–15].
Nonetheless, a recent systematic review suggests that the promise of computer-prompt software programs to interrupt prolonged sitting and promote physical activity remains unrealized because more high-quality research is needed [16]. The systematic review identified gaps and weaknesses in the literature that underscore the absence of comprehensive, systematic approaches for initiating, implementing, and evaluating computer-prompt software programs to decrease sedentary behaviors and increase physical activity during the workday in a work setting [16]. The deficiencies in the literature and the absence of guidelines for rigorous research diminish and hamper the efficiency, effectiveness, and value of installing and using computer-prompt software programs to decrease sedentary behaviors and increase physical activity.
Especially lacking are guidelines and recommendations for systematic research to rectify the deficiencies in the literature. The present article is unique because it includes recommendations for addressing and remedying the deficiencies in this important literature. Improving the published research with high-quality studies can ensure that the full potential of computer-prompt interventions is realized. Because computers are so universal, using them to increase physical activity and decrease sedentary behaviors can affect the health of workers worldwide.
The aims of this article are to present guidelines and recommendations that will foster rigorous computer-prompt software research. Based on deficiencies in the literature and quality assessment tools to reduce the risk of bias in research, ten domains have been identified: composition of the research team, behavioral sciences theoretical frameworks, research design, types of alerts, outcome measures, confounding factors, duration of the intervention, carryover effects, racial and ethnic composition, and organizational culture. Recommendations are presented for each of these ten domains.
Recommendations and guidelines to enhance high-quality research in computer-prompt software studies
Evidence-based weaknesses and deficiencies documented by the recent systematic review [16] and scientific design recommendations for reducing the risk for bias [17] were used to develop a research design flow chart for computer-prompt software research (see Fig. 1). The flow chart is the original work of the author and was designed to reduce the risk for bias, produce rigorous research, and facilitate the establishment of a high-quality evidence base. The unique features of computer-prompt software research include type of alerts (audible, visual, or both), frequency and timing of alerts (every hour, every half hour, after 2 hours of continuous sitting, or worker-determined), and additional alert features (locking the keyboard for a designated time, educational messages about the health effects of prolonged sitting, physical activity recommendations and displays).
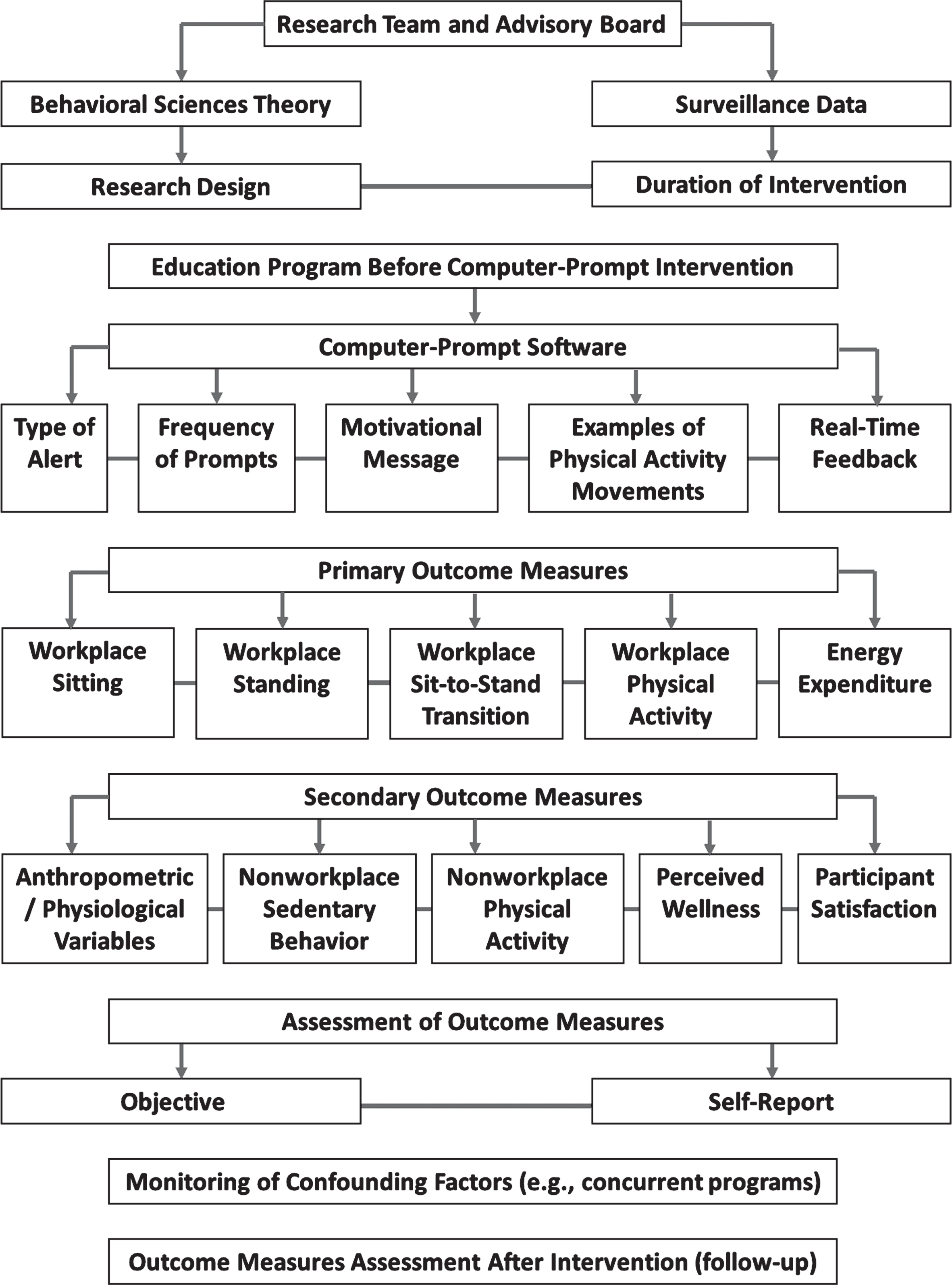
Computer-prompt software research: Workflow of research design.
One of the first decisions is the composition of the research team. The research team should include representatives from employees (stakeholders), employers (the organization’s decision-makers), and public health researchers (experts in behavioral sciences, research design, implementation, and statistics) [18]. The research team is charged with designing and implementing the study. The members of the research team are co-partners in developing the research project. Earlier research has shown the value of a participatory approach at various levels, including formative research [19] and co-production of the intervention [11].
In addition to designing and implementing the research, the research team can be members of the advisory board, which provides oversight for the research initiatives by monitoring progress and suggesting changes throughout the process, as necessary. Advisory board members should have a vested interest in the values, mission, and success of the organization. Thus, the board can include research team members, participants who are not members of the research team, or a combination.
An important early activity for the research team is the surveillance of current sedentary practices, so that the intervention can be tailored appropriately [10, 20]. For employees in the organization, what is the total time spent in prolonged sitting? What is the average duration of sitting bouts? What is the average number of interruptions to sitting time? These data are helpful in developing the intervention and deciding on outcome measures.
Behavioral sciences theoretical frameworks
Research informed and guided by behavioral sciences theoretical frameworks is beneficial for advancing the science base and for replicating and extending previous research. Behavior change is well-documented as being challenging and “tough” [27]. Combining technological tools with behavioral science change theories is important for rewiring human responses [27]. As an example, fitness trackers use behavioral science theory approaches known to decrease sedentary behaviors and increase physical activity [27]. The evidence suggests that using fitness trackers is cost effective. To assess changes in behavioral science theoretical constructs before and after an intervention, mediating variable analyses are recommended [28, 29].
Earlier studies in computer-prompt software literature have used social ecological models of health behavior [11], social cognitive theory [9, 12], and taxonomies of behavior change to facilitate adopting, implementing, and sustaining behavior change [21]. Social ecological models of health behavior emphasize the connection between people and their environments. Multilevel interventions are derived from ecological models to improve population health. The multiple levels of influence that guide interventions include intrapersonal factors, interpersonal processes, institutional factors, community factors, and public policy [22, 23].
Social cognitive theory views human behavior as a set of complex interactions (e.g., triadic, dynamic, and reciprocal models) in which behavior, personal factors, and environmental factors interact. Important social cognitive theory constructs are situation/environment, outcome expectations, self-efficacy, self-regulation, behavioral capability, reinforcement, observational learning, and reciprocal determinism [22, 24, 25].
Taxonomies of behavior change are based on the behavior change wheel, which encompasses three essential conditions: capability, opportunity, and motivation. Using these constructs can lead to more efficient design of effective interventions. Additionally, policies based on these constructs can identify which interventions are effective [26].
Although all of these well-established behavioral science theories have been used with computer-prompt software studies in general, computer-prompt software research designed to decrease sedentary behavior in the workplace has been criticized for the absence of behavioral sciences theoretical frameworks as well as for the absence of a psychology of sedentary behavior [30]. Notably, a psychology of sedentary behavior is not well developed [30]. From another perspective (because computer-prompt software studies are typically conducted at a worksite), a systems science approach for increasing physical activity, decreasing sedentary behavior, and addressing obesity in the workplace has been recommended [31, 32].
Systems science (also referred to as a systems approach, systems thinking, or complexity science) conceptualizes component parts of a system and their interrelationships as emergent properties of that system. Consequently, there is a de-emphasis on attributes of individual components and, instead, a focus on factors that can be observed at the system level. As a metaphor, an individual bird is not the central focus of study; instead, it is the flock— a group of birds flying together. The systems science approach evaluates the holistic nature of heterogeneous and interrelated factors. Given the complex nature of the workplace, with its dynamic, interactive, and interdependent social interactions, systems science is particularly relevant and appropriate for computer-prompt software studies [32]. For example, computer-prompt software alerts and notifications are responded to by individuals, and yet the workplace environment and culture can provide encouragement from coworkers, educational sessions, tips to anticipate alerts, incentives for compliance, penalties for noncompliance, monitoring, and inclusion in performance reviews. This kind of holistic systems approach facilitates the implementation, adoption, and sustainability of behavior change in the workplace.
Research design
Another crucial decision is research design. In computer-prompt software research, randomization at the individual level is not optimal because of potential contamination among individuals in the same department or work area. A clustered randomized controlled trial that is randomized at the office, department, or worksite level is the preferred design, because it enables more precise treatment effect estimates and greater generalizability [9, 21]. The number of units and individuals needed for the research should be based on power analyses.
Before a computer-prompt software intervention is implemented, a well-designed educational program based on behavioral sciences theoretical constructs can be initiated [12]. The purpose of the program is to impart knowledge and create the intention to break up sitting time. The information can include the health risks of prolonged sitting, benefits of breaking sitting time into shorter intervals, and ways to decrease sedentary time at work.
Types of alerts
As shown in the flow chart (Fig. 1), decisions related to the intervention are critical and should be guided by the research team, surveillance data, and a review of the literature. The alert, which is the notification or reminder that a break is needed, can be a small visual in the corner of the computer screen or can cover the entire screen. An audible sound can accompany an alert. One type of alert can lock the keyboard for a designated time (e.g., 15 minutes). Variations include “snoozing” the alert for a specified time (5 or 10 minutes), skipping an alert, ignoring the alert, or pausing the alert until work in progress is complete. The frequency of the alert can be every 45 minutes [33], every hour [9], or randomly generated [12]; other options include allowing participants to set the regularity of alerts according to their own personal preferences [21] or based on prolonged sitting patterns determined by a chair sensor [19]. A motivational message can be part of the alert. In addition, earlier studies have included video demonstrations of appropriate movements for the office environment (e.g., one-leg squat or desk push-up) alongside the alert [34, 35]. Another consideration is real-time feedback to each participant to promote sustained behavior change, such as daily graphic presentations of changes in behavior over time [34, 35]. The intervention should be practical, feasible, evidence-based, and tailored to the needs of the specific organization.
Outcome measures
The outcome measures should be related to the goals of the intervention— i.e., to assess changes in sitting time. High-quality research in the computer-prompt literature includes daily measures of such metrics as total sitting time, average duration of sitting bouts, longest sitting bout, number of sitting bouts longer than a certain interval (>30 minutes; >60 minutes), and number of sit/stand transitions [20]. Other measures to consider are energy expenditure [33], perceived wellness [10], overall sedentary behavior and physical activity (weekday and weekend) [9], participant satisfaction with the intervention [36], and anthropometric and physical assessments (e.g., lipid profile, blood pressure, weight, percent body fat, waist circumference) [9, 34, 35]. The behavioral variables can be assessed by using objective measures (e.g., accelerometers, inclinometers, ActivPAL [PAL Technologies Ltd., Glasgow, Scotland]), subjective assessments (e.g., logs, diaries, recall surveys), or combined approaches [9]. The research team can decide which outcome measures are proper, feasible, and evidence-based.
Confounding factors and external influences
Apart from the intervention, certain external factors should be evaluated. One consideration is confounding factors, such as concurrent programs unrelated to the intervention. For example, is a nutrition or physical activity intervention underway at the workplace or in the community at the same time as the sedentary behavior intervention? To assess external influences, investigators have conducted random telephone checks with their participants to document and monitor other events [33].
One strategy to account for confounding factors is to compute separate analyses for those exposed versus those not exposed to confounding factors. Another approach is to assess the level of participation in simultaneous events and statistically control for the level, rate, or extent of participation in other programs unrelated to the target intervention.
Duration of intervention and carryover effects
To enhance a study’s external validity, a minimum of 8 weeks is recommended for an educational and behavioral intervention [37]. Many studies were excluded from the aforementioned systematic review [16] because the duration of the intervention in those studies did not meet the systematic review’s minimum inclusion criterion of 8 weeks. The longest studies in the computer-prompt software literature were 26 weeks [38] and 24 weeks [9].
In addition to the intervention’s duration, its sustainability is important (i.e., does the intervention continue after the research study period has ended?). In other words, is the computer-prompt software program still being used after the study ends? Are behavior changes supported after the study? It is recommended that 3-month, 6-month, and 12-month follow-ups be part of the research program.
Carryover effects beyond the duration of the intervention are important to document, including evaluating increases in physical activity and decreases in sedentary behavior beyond the workplace during and after the intervention. For example, are there increases in physical activity on the weekend or fewer sedentary behaviors after work hours?
Racial and ethnic composition and organizational culture
Research studies should report the racial and ethnic composition of the study population; diversity enhances generalizability and strengthens claims to causal inferences. It is important to know whether the study population is representative of the work population. Moreover, racial and ethnic composition can be a moderating variable, analyzed separately, or controlled for in the analyses.
Moradi and Wiberg [39] and Taylor et al. [40] report that social context and organizational climate and culture can either enhance or undermine any health-promoting intervention in the workplace. Unequivocal support from senior and middle management is essential. The outcome measures and commitment to the intervention can be influenced by participants’ attitudes (positive or negative) toward management and the organization. An organization’s health-promoting/wellness culture, or lack thereof of, can be assessed and evaluated as a factor contributing to or undermining the effectiveness of a computer-prompt software intervention. An organization may decide that preliminary strategies for developing and enhancing a workplace wellness culture are needed before a computer-prompt software intervention can be implemented.
Recent literature and empirical confirmation for the workflow of research design
The cited systematic review was published in 2021 but was based on literature searches conducted in early 2020 [16]. To find more recent literature, a second literature search was conducted covering the years 2020 to 2022. Based on earlier analyses and systematic reviews, two primary databases, CINAHL and Ovid, were used for the second literature search. The search strategy included the Boolean operators AND, OR, and NOT. The following keywords were used in a variety of combinations and configurations with the Boolean operators: work environment/workplace, software, reminder system, computer-prompt, sedentary behavior, physical activity/inactivity, and desk/office workers. More than 100 publications from 2020 to 2022 were reviewed; only one relevant publication had a computer-prompt intervention to decrease sedentary behaviors among desk-based workers, and one publication had a relevant formative assessment.
In the United Kingdom, a randomized computer-prompt intervention used Exertime (University of Tasmania Active Work Laboratory/Leading Edge Only LTD., Cranfield, UK) as the e-health computer-based software [41]. In this intervention, the computer-prompt software included a prompt bubble that appeared every 45 minutes on the bottom right-hand side of the participant’s computer screen, showing that it was time to take a break from sitting. Participants chose either to engage with or postpone the prompt. When engaging, the participant had to click on the software before regaining control of the computer. If postponing, the participant could temporarily delay the prompt for 5, 10, or 15 minutes. Participants who activated the break system could end the break by clicking to stop the timer, after which the break’s duration was logged in the software. All choices of computer-prompt software features in this intervention are described in the workflow of research design (Fig. 1) under Computer-Prompt Software.
In the discussion section of the study [41], it was recommended that future interventions be co-developed with office-based workers, researchers, and software developers. This recommendation is consistent with the first stage of the workflow of research design, Research Team and Advisory Board (Fig. 1). In the computer-prompt study [41], participants were emailed an educational e-booklet before the intervention. The material described the importance of decreasing sitting time and how to use the software. This part of the intervention is recommended in the Education Program Before Computer-Prompt Intervention of the workflow of research design.
As the most recent computer-prompt software intervention [41], this study provides support and confirmation that the workflow of research design shown in Fig. 1 is comprehensive and includes the essential elements for developing a computer-prompt intervention. Furthermore, the participants in the study agreed that the prompting feature was a useful cue for breaking up prolonged sitting periods at work [41].
In another study aimed at decreasing sedentary behavior at work [42], the authors implemented an intervention mapping protocol to develop an automated coach-delivered motivational intervention in combination with a wearable accelerometry monitoring device. Although that intervention differed from a computer-prompt intervention (the focus of this paper), both types of interventions are designed to decrease sedentary behavior at work. Therefore, a comparison between the intervention mapping approach and the stages of research development from the workflow design can be illuminating, informative, and instructive.
The first step of the intervention mapping approach was to conduct a needs assessment, which is consistent with the Surveillance Data Stage of the workflow of research design because current sedentary behavior patterns are analyzed. Step two of the intervention mapping approach was to state the program outcomes and objectives, which is comparable to the workflow of research design processes described in Behavioral Sciences, Research Design, Primary, and Secondary Outcomes. Step three was to design the program, which is described in the workflow under the Selection of Computer-Prompt Software. Step four was to develop the intervention program (i.e., program production) which is comparable to the workflow in all the features described under Computer-Prompt Software, including alert type, prompt frequency, and motivational messages. Step five was to plan program implementation, which is incorporated into the workflow’s Education Program Before Computer-Prompt Intervention. Finally, step six was to develop an evaluation plan, which is described in the workflow’s Assessment of Outcome Measures (both primary and secondary outcomes).
Before detailing the six steps, the authors wrote, “An intervention planning group includes stakeholders who can make relevant contributions to the development, implementation, and evaluation, such as members of the target group and future implementers” (42 p2). In the workflow of research design, the first stage is the Research Team and Advisory Board, which is similarly composed of stakeholders, managers, and employees.
In summary, all six steps of the intervention mapping protocol plus the intervention planning group [42] are also recommended components of the workflow of research design presented in this paper (Fig. 1).
Strengths and limitations
One potential limitation of the workflow of research design is that a serious commitment is needed from top and middle management of the organization, as well as from employees. Resources, time, and effort are required to implement the research design. Another potential limitation is the co-partnership with the research team and stakeholders. Sometimes, business owners, supervisors, and managers are accustomed to being in charge and not relinquishing responsibility and power. Working with the research team means power sharing and shared input into the process. As with any new protocol, future implementation and application will determine its value, usefulness, and effectiveness.
This workflow of research design has several strengths. There is a gap in the literature related to comprehensive and systematic approaches to initiate, implement, and evaluate computer-prompt software programs for decreasing sedentary behavior and increasing physical activity during the workday in a work setting. This gap diminishes and hampers the efficiency, effectiveness, and value of installing and using such computer-prompt software programs. Furthermore, the research design was developed based on a recent systematic review documenting deficiencies in the research literature combined with strategies to minimize risk for bias in research. Additionally, the research design is consistent with other recommended frameworks for initiating and implementing new research. The protocol includes monitoring the process and evaluating outcomes at multiple levels during and after the intervention. Importantly, the workflow of research design is flexible and adaptable to the needs, expectations, and preferences of each organization. In other words, the protocol is not a rigid cookie-cutter process with no flexibility. Overall, the workflow of research design has the potential to contribute to the literature by addressing major deficiencies and improving health outcomes.
Conclusions
In summary, the workflow of research design presented in this article was developed to minimize risks for bias in research, help thoughtful decision making, and promote high-quality research to improve computer-prompt software research. Future research is needed to assess the efficacy, effectiveness, efficiency, and value of computer-prompt software interventions. By adhering to the workflow of research design recommendations in this article, the full potential of computer-prompt software interventions can be realized to decrease sedentary behavior, increase physical activity, and thus improve the health of desk-based workers throughout the world.
Footnotes
Ethical approval
Not applicable.
Informed consent
Not applicable.
Conflicts of interest
The author declares no conflicts of interest.
Acknowledgments
Jeanie F. Woodruff, BS, ELS, contributed to the editing of the manuscript.
Funding
The author reports no funding.