
Abstract
BACKGROUND:
Worksite health promotion programs (WHPP) aiming to reduce presenteeism are rapidly increasing. However, program-efficacy seems impaired by lack of conceptual understanding and theoretical frameworks related to presenteeism.
OBJECTIVES:
To study (1) the concept of presenteeism, (2) the causes of the phenomenon and (3) which WHPP affect presenteeism.
METHODS:
We followed the PRISMA 2020 guidelines for mapping relevant literature in seven databases. The main search-terms were “worksite”, “WHPP”, “presenteeism”, “employee productivity” and “interventions”. Reviews and review of reviews were included and analysed according to research questions and ecological theory.
RESULTS:
Of 2196 studies identified, 14 reviews were included, comprising 1390 single studies. Conceptually, presenteeism was poorly defined, mostly related to productivity/performance limitations due to ill health. Factors causing presenteeism addressed individual health or lifestyle (78%), and, to a lesser extent work and organisational factors (management/job stress) (22%). Forty-five highly diverse WHPP were identified, about 90% focusing health outcomes. 22/45 WHPP affected presenteeism/productivity positively. Multi-component WHPP implemented at multi levels accounted for 55%. Single-component programs, implemented at individual level, were mostly targeting health-risk subgroups. No specific WHPP seems preferable. Methodological quality seems highly associated with worksite intervention-efficacy.
CONCLUSION:
Increased telework opportunities due to COVID-19 experiences has affected working conditions worldwide, for better and worse, requiring adaptions at employee, management, organisational and socio-cultural levels. Our results showed high program diversity, several adaptable to future needs (e.g., digital solutions), however hampered by narrow focus on individual health. Future research should focus on theory-based high quality multilevel WHPP comprising contextual, work, and organisational factors.
Keywords
Introduction
The increasing incidence of unhealthy lifestyle e.g., sedentary behaviour, poor nutrition, and lack of stress management, has resulted in mental and physical health problems [1], also affecting the labour force, and often resulting in sickness presenteeism (e.g., attending work while ill) [2–5]. This emerges as a growing problem worldwide, with prevalence rates of presenteeism varying from 30% to above 90% [4, 5], showing even higher rates lately due to the extensive short- and long-term consequences of the COVID-19 pandemic on people’s family and private lives, health, work, and social security [6–8].
Most often sickness presence is about reduced work capacity of employees and productivity loss, due to psychological and physical health problems, not necessarily leading to health-related absence from work (i.e., absence from work due to illness or disability) [4]. However, a common agreement on definition, framework and tools used to measure its impact is not yet established [5, 9]. Our focus of interest is to further explore how the concept and causes of presenteeism are described in the scientific literature. The theoretical basis and conceptualisation of presenteeism influence efficacy of worksite interventions [4, 9], the latter, which is of particular interest in this study.
The term presenteeism is understood and used differently in scientific research [4, 9]. Firstly, it is closely related to individual lifestyle and health [10]. Secondly, presenteeism is related to environmental and psychosocial work factors (e.g., work demands, work control, social support) [11–13], including leadership [14] and finally, to productivity loss and financial cost (e.g., estimations of economic impact of presenteeism) [9, 15]. Economically, presenteeism seems far more challenging than health-related absence [5, 16] and more complicated to determine as it is not formally registered, being both invisible and subjective. Accordingly, it is often a hidden cost in businesses [16]. Due to its consequences for both employers and employees, the interest of the phenomenon has grown substantially during the last decades. Employees that frequently exhibit presenteeism are at greater risk of developing health issues in the future, which in return may lead to health-related absence [4, 10]. Absenteeism and presenteeism share a common ground, as they are both types of absence [17]. Meta-analytical data show strong correlations between health-related absence and presenteeism, also indicating that the relationship varies with contextual factors [9, 18]. This seems particularly true for employees in front occupations (e.g., hospital staff, teachers, public transport drivers) [6–8, 11].
The interest in the concept of presenteeism seems mainly to represent two distinct sources [3, 4]. One tradition, mostly American, assessed the productivity consequences of presenteeism as a function of various health conditions (e.g., musculoskeletal pain or mental health problems), while ignoring the causes of showing up ill. This resulted in a focus on measurements on productivity losses, individually oriented wellness and medical interventions aiming at reducing these losses [3]. In the other tradition, mainly European, research focused on presenteeism as a behavioural pattern of going to work with impaired health. Studies have investigated the causes, consequences, and the motives for this behaviour, frequently measured as the occurrence of presenteeism, and often reflecting job demands and other occupational characteristics causing stress and illness [3, 9]. Interventions related to this tradition may reflect e.g., job redesign and reduced job stress, as well as occupational health and rehabilitation programs [9]. Hence the concept of presenteeism is a complex phenomenon influenced by several factors.
Johns [3, p. 251] developed a theoretical framework containing elements of both traditions above, defining presenteeism as “attending work while ill”. He emphasized the importance of merging organisational theory with those of occupational health and epidemiology. This view has received special attention and is further developed in recent research [4, 9, 18]. For example, Lohaus and Habermann [4] presented a comprehensive framework for understanding presenteeism, integrating Johns’ [3] work. They emphasised environmental influences (e.g., culture, policy, legislation), organisational (e.g., absence policy), work – and person-related variables (e.g., workload and health) as the foundation for decision-making ability and the individuals’ possibility to choose either presenteeism or health-related absence. Most researchers in the field have focused on the negative consequences of presenteeism, however, presenteeism may also have positive outcomes [13, 19, 20]. Karanika-Murray and Biron [20] developed a framework representing four varieties of presenteeism, referred to as functional, therapeutic, dysfunctional, and overachieving presenteeism. Whether to choose presenteeism rather than sickness absence, is influenced by the availability to perform and the severeness of health impairment [20]. Functional and therapeutic presenteeism evolve positive outcomes. Employees managing work performance at a high level despite health impairments and simultaneously regaining one’s health, is described as functional presenteeism. Therapeutic presenteeism behaviour benefits health, but not necessarily enhancing performance. However, to facilitate these choices, a conscious and supportive management is required as well as resources to adjust related to work demands and psychosocial work conditions (e.g., reduced working hours) [19, 20]. Considering the occurrence of the different varieties of presenteeism is particularly important due to increased telework, lack of on-site management and changed health rules and regulations as a consequence of the COVID-19 pandemic [21].
Several researchers have investigated consequences of increased telework [21–23]. Steidelmüller et al. [22] reported associations between homebased telework and increased self-endangering behaviour, e.g., sickness presenteeism, during the pandemic. Gerich [24] further explored and elaborated these associations in a path-analysis on survey data from three economic sectors. Employees with pre-pandemic telework experience more often used telework for work intensification (e.g., working in weekends and days off) to meet changed work demands, (partly) resulting from new or changed leader behaviour (goal directed management/indirect work control). Indirect work control was associated with increased sickness presenteeism, indicating the importance of work organisation and leader behaviour on employee presenteeism [24]. Based on this research, it is reasonable to assume that both negative and positive effects of presenteeism will increase in most occupations in the future, depending on organisational, managerial, and individual adaptations to changes (e.g., more telework, increased indirect work control, changed social support, increased health impairments) [9, 20, 21, 25]. Hence, strategies to manage or reduce presenteeism behaviour are in demand [9]. Such interventions are still scarce [5], and characterized by conceptual differences, incomparable instruments to measure the phenomenon and lack of tailoring the programs to context, the program outcomes, or participants [26]. To meet the complexity and the many unforeseen challenges in the field, the current theoretical knowledge should be taken into consideration, focusing on complex, multilevel interventions concerning environmental, organisational, and individual determinants of health and health behaviour [27]. Lack of systematic implementation and process evaluation also seems to influence the outcome effects of WHPP [28]. Poor implementation affects methodological quality and impair transfer of evidence-based programs to real life worksite settings [29].
The purpose of this review is to increase knowledge of presenteeism and its significance. To thoroughly explore our main aims, we investigate (1) how the concept of presenteeism is described in the scientific literature, (2) what factors influence the concept and (3) which WHPP affect presenteeism. To address the complexity in the field of theory and interventions, we chose to analyse our results according to ecological theory, which include the numerous causes and levels of implementation [30, p. 41], specifically the individual (I), organisational (II) and socio-political (III) levels.
Methods
Literature search and study selection
To answer the research questions, a systematic review was conducted [31] and scientific literature systematically searched in seven databases (Business Source Elite, the Cochrane Library (Systematic Reviews and Trials), EMBASE (Ovid), MEDLINE (Ovid), PsycINFO (Ovid), Sport Discuss and Web of Science). In January 2019, a professional librarian along with the authors conducted the targeted search of literature in the databases from 2010 to the current date at the point. An extended track down of articles consecutively published throughout 2020 were executed. Inclusion criteria were worksite setting, employees aged 18 to 70 years, both sexes, employed and attending health promotion programs provided in work settings. The outcome variable of interest was presenteeism and/or productivity loss. We included systematic literature reviews as well as review of reviews from a North American-, European and Australian / New Zealand context written in English. Grey literature was omitted due to our interest primarily in peer-reviewed effect-studies and experimental designs. Exclusion criteria were studies published before 2010, not written in English, non-review designs and settings other than worksite. Asian, South American, and African studies were excluded due to different working environment legislation and labour laws.
To reflect the issue precisely and avoid bias, a customized Population-Intervention-Comparison-Outcome (PICO) -search was performed to identify and organise keywords. Terms were based on MeSH indexing and thesaurus’ as well as free text terms. The searches were mainly based on the following terms and procedures; (workplace* OR worksite* OR “white collar” OR employ* OR occupation*) AND (“physical activity” OR exercise OR “stress management” OR “health promotion” OR “organisational intervention*” OR “occupational health intervention*” OR “worksite health promotion program*” OR leader* OR “life skill”) AND (absenteeism OR “sick leave” OR presenteeism OR “employee productivity“ OR “productivity loss“ OR “cost“ OR “work while ill” OR “work while sick”). Furthermore, the results from the PICO-search were transferred to EndNote, a reference-mapping tool. Duplicates were removed prior to screening. The literature review was completed using The Preferred Reporting Items for Systematic Reviews and Meta-Analyses – PRISMA 2020 checklist. This checklist guides the researcher through all parts of the literature review that need to be considered and explained [32]. As the flow diagram (Fig. 1) shows, 2196 publications were identified in the main search. Both authors worked independently in separate Endnote files, and performed a blind title, abstract and key words screening, and evaluation of relevance before comparison of results. After the individual inclusion and exclusion processes, the results of both authors were compared and discussed. All titles identified were manually examined for relevance. Relevant titles lead us to consider the abstracts for applicability and eventually inclusion. Fifty-six articles, rated to be of importance, were retrieved in full-text and underwent scrutiny according to the inclusion criteria. Any doubt or disagreement about inclusion was resolved by discussion and consensus. Fourteen articles met the inclusion criteria. Periodic updating of the search between 2019 and 2020 did not identify additional publications (see PRISMA 2020 flow diagram, Fig. 1).
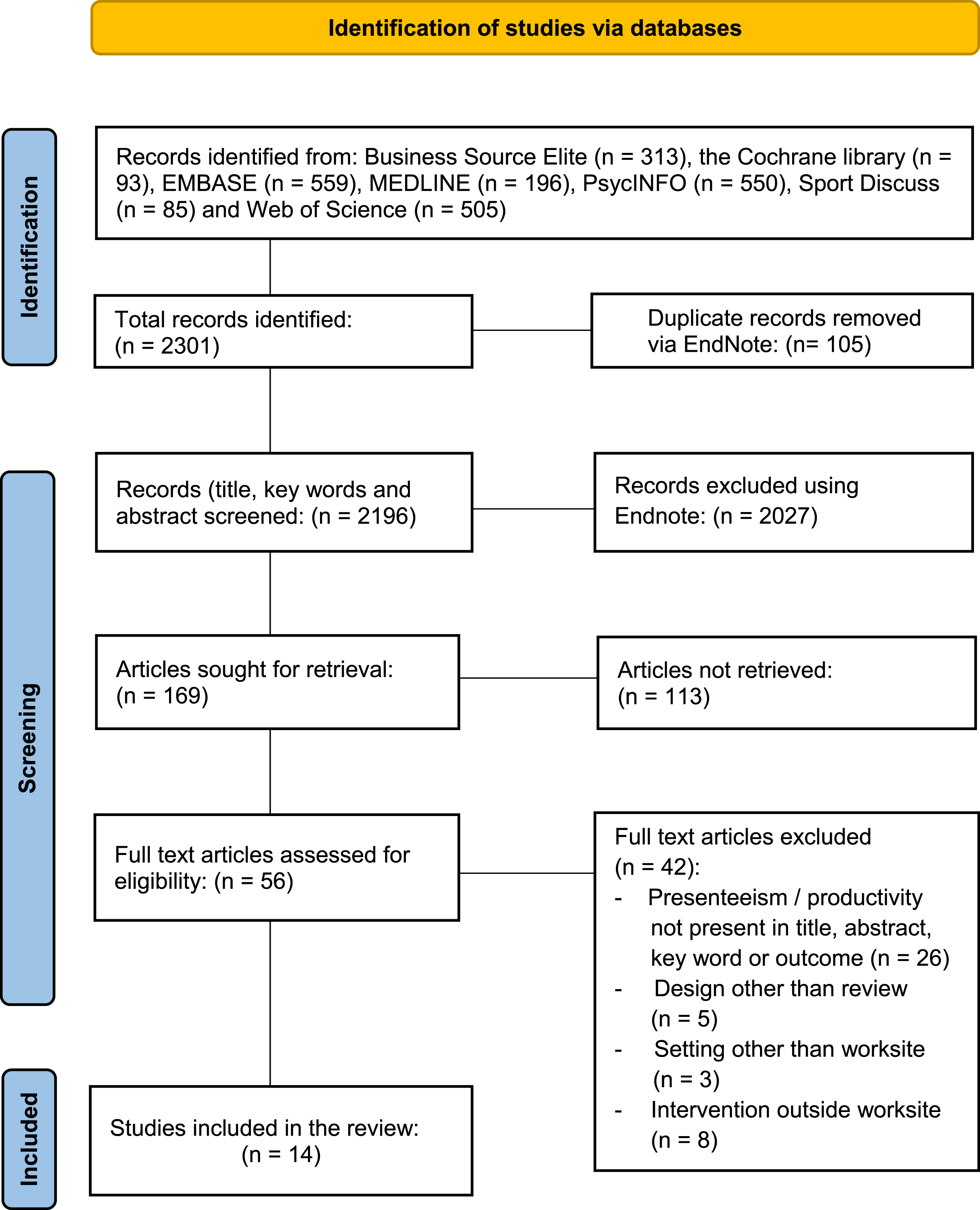
PRISMA 2020 flow diagram of the literature search.
Based on a narrative synthesis [31], key points of eligible studies were summarized in an overview of the included studies. Each study was examined for independent information about first author, publication year, nationality, aim and study outcome. In addition, we included information about method (study design, included number of databases searched, number of studies, designs, participants, setting and use of theoretical framework). To appraise risk of bias, methodological quality in each included review was assessed according to a questionnaire customized to this study. The form consisted of six questions (see Supplement 1). Each study was given a number: yes = 1, no = 0, and maximum total score was 6. The 14 studies were graded: high (score 6), moderate (score 4-5), or low methodological quality (score < 3). Studies lacking methodological information were termed inconclusive (IC). In addition, each single study identified (n = 44) reporting on relevant outcomes for our study, was appraised for reported internal methodological quality based on the review-authors own descriptions. A simple cluster analysis on reported positive/negative outcome effect versus reported graded methodological quality was completed for each study.
To answer our research questions, the results were analysed according to research questions and health promotion theory [30] emphasizing categorization into three implementation levels: (1) individual level, (2) organisational level and (3) socio-political level.
Risk of bias
Selection: The very few studies reporting on relevant outcomes (3%) and only considering studies written in English may both represent a selection bias. During the selection of the 14 reviews, misinterpretation can occur and the decision to retain or discard articles may fail.
Interpretation: Lack of a unified established framework and divergent definitions of presenteeism lead to different interpretations and varying quality of measurements. It requires valid narrative analysis. The absence of a valid and clear definition of central terms may lead to interpretation errors. Work-norms, social security and insurance systems worldwide vary extensively, and overall cultural and political guiding principles also influence how individuals interpret presenteeism. A literature review is a qualitative study that requires subjective interpretation. This is illustrated by Cancelliere et al. [35] and Jensen [36] reporting differently from the same included studies, see e.g., Mills’ intervention [37].
Measurement: An additional source of bias is the measurement of presenteeism. It is measured both objectively and subjectively, by costs and questionnaires [33]. There is no standard universal measuring method for presenteeism, and standardised objective measurement tools are lacking [9]. Authors measure and assess presenteeism differently. The construct validity is low and apparently affecting in particular measuring methods negatively. Therefore, valid measurements on presenteeism are still missing [4].
Methodological appraisal: The quality evaluation of included studies is based on customized selection criteria, e.g., number of RCTs, their methodological assessment and own reported quality grading of studies. In addition, quality appraisal of the single studies included in our analysis are based on review-authors own grading of these studies; hence the report of methodologically quality might be difficult to interpret and thereby associated with some uncertainty [34].
Duplicates: As literature reviews, and review of reviews, are included, some reviews and single studies are evaluated more than once. To avoid double processing, we excluded two reviews [36, 38] from the analysis of Schröer et al. [48], one review [35] from White et al. [49] and one [39] from Wagner et al. [50]. In addition, several single studies were excluded from the rest of the material (see Supplement 3). However, the review-authors presents their results in different detail, the possibility of double processing of information cannot be ignored.
Results
Description of the material
In the main search, 2196 eligible publications were identified, of which 56 studies were retrieved in full-text and underwent detailed assessment according to the inclusion criteria. Finally, 14 studies were included in this analysis (see Fig. 1). Eleven studies were systematic reviews containing 262 single studies [35, 36, 38, 40–47]. The remaining three studies were review of reviews [48–50] (see Table 1). After elimination of duplicates, the material comprised 53 reviews and 1390 single studies. However, we were only able to identify 44 single studies (3%) reporting on presenteeism or productivity as an outcome variable.
Description of included studies
Description of included studies
BP: back pain, LBP: low back pain, PA: physical activity, (R)CT: (randomized) controlled trial, RTW: return to work, WHPP: worksite health promotion program(s).
About two-thirds of the single studies comprised a RCT or quasi-experimental design. Other frequently used designs were controlled trials (CT), cohort or observational/epidemiological designs and some cross-sectional studies. The included reviews originated from Australia [38, 44, 45], Canada [35, 49, 50], USA [46] and Europe [36, 40–43, 47, 48] (see Table 1). The participants were employees from a variety of worksite settings, both public and private, in health, educational and service settings. Two studies focused specifically on employee subgroups with musculoskeletal pain [40, 45] and Wagner et al. [50] studied employees with mental health problems (e.g., depression and anxiety).
In our material, all studies but two [41, 46] (86%) described the concept presenteeism, however in different ways (see Table 2). 7/12 studies described presenteeism related to health or lifestyle. Of these, 4/12 studies (33%) focused productivity loss due to reduced health or lifestyle [45, 47, 49, 50]. Brown et al. [38] and Cancelliere et al. [35] added a work performance aspect to their concept of presenteeism (e.g., performing below par) and Jensen [36] described presenteeism as attending work while ill, without focusing the consequences of the act. Cancelliere et al. [35] was the only study having presenteeism as the only outcome. 5/12 studies (42%) specified the productivity dimension as a work-related outcome (e.g., job performance), not solely related to health [42–44], while two studies (17%) reported economic consequences of productivity loss [40, 48] (see Table 2).
Descriptions of the concept presenteeism
Descriptions of the concept presenteeism
Only two studies (14%) described presenteeism/productivity loss in a theoretical context. Kröll, Doebler and Nuesch [43] used psychological stress theory (the Conservation of Resources (COR) theory) to predict and understand effects of primary (flexible work arrangements) interventions versus secondary preventive (stress management training) interventions, while Oakman et al. [45] used a macro-ergonomics framework, the Sociotechnical System Theory, to analyse their results on productivity in workers with persistent musculoskeletal pain (PMP) (see Supplement 3).
All but two studies [44, 46] reported different factors affecting presenteeism, in sum 75 factors. In this analysis, we categorized the factors according to three levels (see Table 3).
Factors reported to affect presenteeism
Factors reported to affect presenteeism
Individual level (I): 12 studies (100%) reported factors influencing presenteeism / productivity at this level. Most of the factors (78%) addressed lifestyle (e.g., physical inactivity, unhealthy eating, smoking) [35, 42, 47–50], physical and mental health (e.g., musculoskeletal pain, and depression, anxiety, wellbeing) [35, 36, 38, 40–43, 45, 49, 50] and immaterial, psychological, and biological factors (e.g., money, working age, disability perception) [43, 45, 48–50].
Organisational level (II): 5/12 studies (42%) reported on this level. 21% of the reported factors affecting presenteeism addressed psychosocial and/or physical environmental factors (e.g., job stress factors, poor relations with co-workers) [35, 43, 49, 50] or work organisation and management factors (e.g., lack of resources, poor relation to leaders) [35, 41].
Socio-political level (III): no factors were found at this level (see Table 3).
All studies except two [41, 46] described the intervention programs investigated to influence presenteeism/productivity, in total 45 programs (see Tables 4 and 5), of which 22 (49%) influenced our outcome variables positively. In particular, the study of Cancelliere et al. [34] contributed strongly reporting thirteen programs (31%) impacting presenteeism, of which nine were graded with high or moderate evidence of effect (see Table 4).
Worksite health promotion programs affecting presenteeism positively
Worksite health promotion programs affecting presenteeism positively
CBT: cognitive behavioural therapy, HAD: fully height adjustable desk, HADM: height adjustable desk for monitor only, HES: health environment security, IC: inconclusive, LBP: low back pain, MSP: musculoskeletal pain, SMT: stress management training, PA: physical activity. H: high, M: moderate, F: fair, L: low methodological quality.
Worksite health promotion programs not affecting presenteeism
CBT: cognitive behavioural therapy, HAD: fully height adjustable desk, HADM: height adjustable desk for monitor only, HES: health environment security, IC: inconclusive, LBP: low back pain, MSP: musculoskeletal pain. SMT: stress management training, PA: physical activity. H: high, M: moderate, F: fair, L: low methodological quality.
The programs mostly (90%) focused individual health, lifestyle, or ergonomic conditions, and to a very small extent organisational factors (i.e., changed rest breaks [35]), containing a variety of components and active ingredients. 12/22 programs (55%) showing positive impact on presenteeism/productivity, were multicomponent programs implemented at two or more levels [35, 36, 38, 42, 43, 48, 50]. Mixed programs, involving individual and organisational levels seems to influence presenteeism favourably (e.g., participatory processes interventions implemented as teamwork including several organisational levels [35], digital cognitive behavioural therapy including health risk assessment, tailored feedback, and other actions on three different levels [42]).
The remaining 10/22 programs (45%) reporting positive effect were single component, implemented on an individual level only [35, 44, 45, 47] (see Table 4). Many of these programs were offered to risk populations e.g., exercise rehabilitation for musculoskeletal pain, light therapy for insomnia, telephone therapy for depressed and dietary behavioural interventions. However, 14/45 (31%) both single and multicomponent programs failed to influence presenteeism/productivity significantly. Nine studies (20%) reported inconclusive results [40, 43, 49] (see Table 5).
According to our quality assessment, 8/14 (57%) studies were rated with high methodological quality [35, 40, 42, 45, 47–50], 3/14 (21%) with moderate quality [36, 43, 44], and 3/14 (21%) with low quality [38, 41, 46]. Most of our included studies, we evaluated to be moderate to high (see Supplement 2).
Further analysis revealed 30/45 (67%) single studies rated, by review-authors, as moderate to high in methodological quality. 14/45 (31%) studies were graded with low quality, often due to small samples, inadequate designs, or other implementation weaknesses (see Tables 4 and 5). Most of the studies 19/22 (86%) reporting positive effect on presenteeism were graded with moderate to high methodological quality (see Fig. 2), indicating a strong relationship between positive intervention effect and high methodological quality. Studies reporting no effect on presenteeism showed mixed methodological grading (see Fig. 2), however 8/9 studies reporting inconclusive results were graded with low methodological quality.
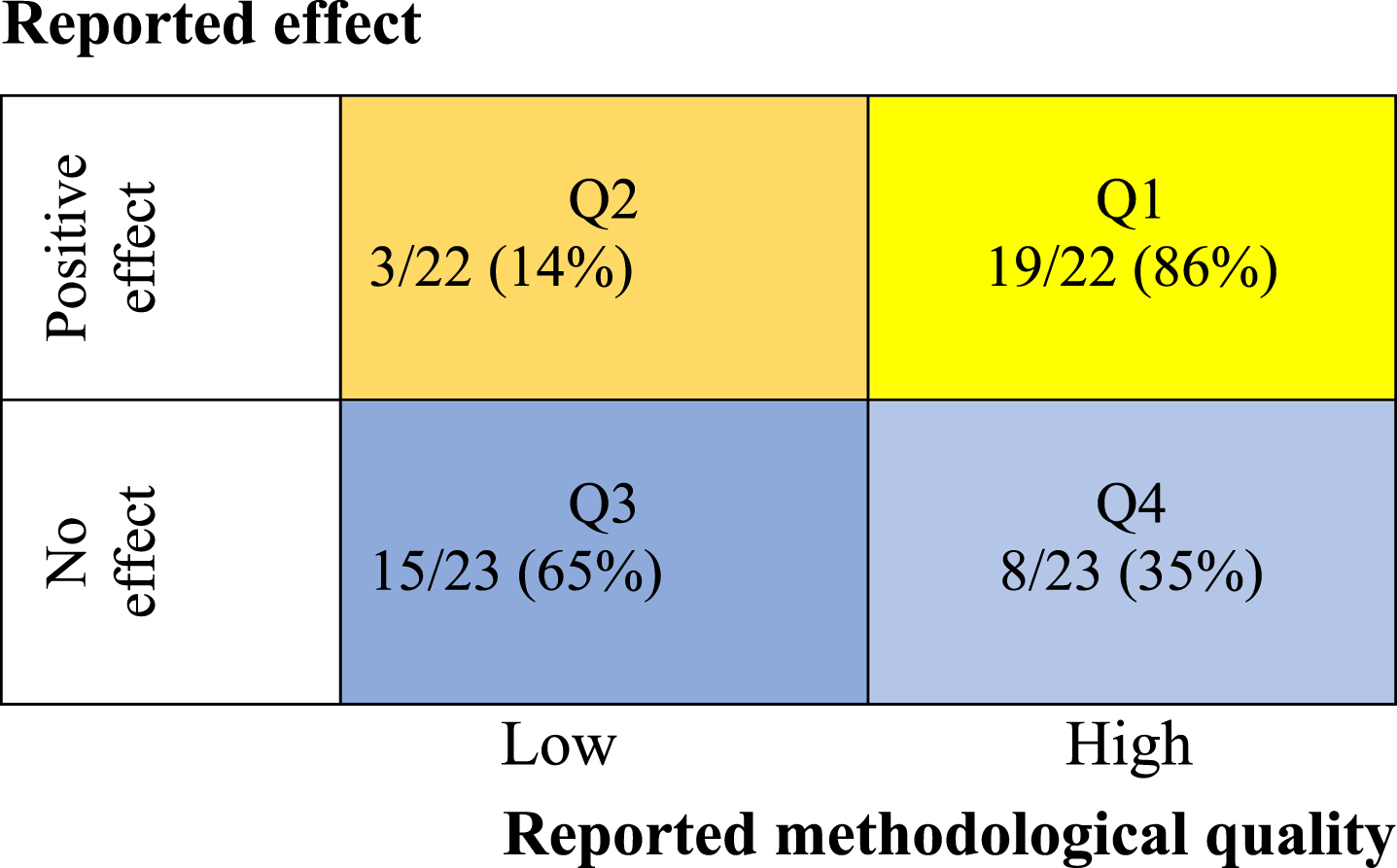
Cluster analysis of studies reporting outcome effect related to methodological quality. N = 45. Q1: positive outcome effect/high methodological quality. Q2: positive outcome effect/low methodological quality. Q3: no or inconclusive outcome effect/low methodological quality. Q4: no or inconclusive effect/high methodological quality.
Definitions of the concept presenteeism
In our material, few studies defined the concept of presenteeism precisely. In more than half of the studies presenteeism were related to productivity loss or performance limitations due to individual health or lifestyle impairments. These findings correspond with previous research in the field [3, 4, 9]. Few studies described presenteeism related to work factors or cost, and none addressed socio-political level e.g., policy or legislation. A major challenge facing this diversity of concept definitions, is low concept validity of presenteeism, leading to different measurements and lack of useful theoretical frameworks. As also shown in former research [3, 4, 13]. However, a significant increase in the research field of presenteeism focusing concept development and theoretically framework building, has emerged lately [3, 4, 13, 18–21, 24]. Fully agreement on the definition of presenteeism is still not received, but increasingly more researchers agree on a definition of presenteeism as a behaviour choosing attending work while ill [3, 9, 26]. The way the concept is defined and measured greatly influences the organisation and facilitation of work and working conditions for employees with impaired health [26]. Although the concept mostly has been viewed negatively [3], positive consequences of presenteeism have increasingly been demonstrated [18, 20]. This duality of presenteeism having both positive and negative consequences, are shown in recent research through different experiences with changed working conditions e.g., increased telework during the COVID-19 pandemic [19, 21, 24]. However, whether increased telework should be experienced positively or negatively depends on a number of factors linked to the severity of the illness, personality factors, type of work, working conditions and organisational factors (e.g., management, job control, job demands) [22, 26]. Karanika-Murray and Biron [20] elaborates this in their recently developed framework stating that presenteeism behaviour is a choice, adaptive in nature balancing health and work performance.
In the present study, there is a general lack of theory. Only two studies base their analysis on a theoretical framework [43, 45]. Kröll et al. [43] draw on conservation of resources theory (COR) in their meta-analysis of flexible work arrangements (FWA) and stress management training (SMT) reporting that both FWAs and SMT correlated positively with psychological health and job satisfaction. The COR theory provide a framework for understanding job stress and has proven lately to be an important contributor in the development of a theory of presenteeism [20, 26].
Recently, there has been a conceptual development of presenteeism as a dynamic, adaptive, optional behaviour, which is not reflected in our material describing presenteeism mainly by its negative consequences due to health or lifestyle, e.g., productivity loss. More theory-based research is needed to clarify the many questions still not answered related to the concept of presenteeism.
Factors identified to influence presenteeism
As reported the concept of presenteeism is multifactorial and inherently complex, which may explain the variety of factors affecting presenteeism revealed in this analysis. As expected, most factors addressed individual lifestyle and poor physical and psychological health conditions, also confirmed by others [18]. Meta-analytical findings emphasise in particular the importance of mental health (depression, stress, burnout) and general ill health as important in the decision of presenteeism behaviour [18].
In our analysis, few factors were linked to organisational and/or socio-political level, though many scholars [e.g., 3, 12, 13] highlight the importance of these factors as causes of presenteeism. Miraglia and Johns [18] reported several work factors to be of importance e.g., strict work absence policies, high workload, understaffing. However, some of our studies reported high job stress (e.g., lack of resources, poor relations with co-workers, management, and leaders) affecting the decision to choose either presenteeism or health-related absence. This corresponds with earlier findings, using the COR conceptual framework to analyse and explain presenteeism [20]. Chen et al. [25] showed that different job and personal resources (social support) could buffer the negative effects of job stressors on health-related productivity losses. Personal and contextual factors also become important, as shown in our analysis (e.g., money and power, expectations, knowledge, or physical work environment), being motivational components connected to presenteeism [3, 4]. Contextual factors may be related to work and organisational characteristics, like job satisfaction, expectations, belonging and rewards as well as job stress [3]. All these factors count in the decision of going to work or staying at home.
WHPP influencing presenteeism
The analysis of this review revealed a large number of different WHPP implemented to impact presenteeism or related outcomes. The programs varied widely regarding design, content, duration, outcomes, and implementation, also shown by other researchers [9, 51]. However, the literature investigating presenteeism interventions is scarce [5, 26], mostly targeting physical and mental health and stressful work environments, also found in our study. Half of the programs in our material showed positive effects on presenteeism. Cancelliere et al. [35] accounted for a substantial part of these effective programs, all rated with moderate to high methodologically quality. Other key features mentioned in their study were frequent use of health risk assessments, also reported by others in our sample [36, 42] and tailored programs specifically to the participants needs.
In addition, only multicomponent programs implemented at multi levels showed positive effects on presenteeism also supported in health promotion theory and research [3, 4] and scientifically based recommendations for health promotion programs [30, 52].
Most of our multicomponent studies showing positive effects were rated with moderate to high methodological quality. This is supported in implementation science claiming that high implementation quality increases the outcome effect of interventions [29].
In contrast, less than half of the implemented programs showing positive impact were single component, addressing presenteeism by often targeting individual health and/or lifestyle problems implemented on an individual level. Our study showed mixed results, while Oakman et al. [45] stated that “in general, individually focused interventions are likely to have no significant impact on improving productivity”, Cancelliere et al. [35] and Kröll et al. [43] reported beneficial effect on presenteeism of simple worksite programs addressing depression, job stress or other mental conditions. Both studies focused on simplicity by implementing single component programs, a strategy also supported by earlier research of Hutchinson and Wilson [53], finding that interventions focusing on one main area of change (e.g., health, diet, or PA) were associated with larger mean effect sizes. A reflection to make when focusing single component programs addressing small samples at risk, is the lack of focus on causality in the organisation, and thereby absence of strategies as prevention, maintenance, and sustainability of programs. Several studies did not contain identifiable program factors that were clearly pervasive. Reasons may include a lack of fundamental anchoring at the organisational and management level as well as methodological problems and barriers such as small groups or poor implementation of the programs [29]. Implementation failure might give negative results in an otherwise successful intervention (low participation rate, response rates, and intervention adherence) [35].
The implications of our analysis are highlighting presenteeism as subject to growing interest, practice, and financial control among leaders. In particular the relationship between employers and employees has received attention during the pandemic [14, 24, 26], e.g., Gerich [24] suggests supportive managerial strategies to handle employees’ self-endangering behaviour (sickness presenteeism) in the time of increased telework.
About half of the reported interventions (approximately 45%) in our study were implemented digitally (e.g., telephone therapy, web-based lifestyle programs, exercise programs) or could easily be adapted to a more remote working situation (height adjustable desks, exercise programs). This might be promising in the light of the pandemic, with increased numbers of employees working remote, or with flexible work arrangements.
In summary, our findings support a common assumption, that multicomponent interventions implemented at several levels, shows good evidence of positive effect. However, despite extensive research on WHPP to reduce worksite health problems, there is no consensus as to which WHPP have the best effect on presenteeism or what programs to recommend.
Strengths and weaknesses
This study has several strengths. Search in seven independent sources increase the precision of eligible study inclusion. Reporting all steps in the comprehensive review using PRISMA 2020 guidelines make the process reproduceable. Assessing and appraising methodological quality in included reviews as well as included relevant single studies also seem to be a strength. The in-depth analysis of the material revealing that only 3% of included studies actually define, describe, or measures the concept of presenteeism, seem on one hand, to represent a strength. On the other hand, this finding also represent a selection bias which is a weakness. Due to selection bias, there is not sufficient scientific basis to draw firm conclusions. The included studies cannot be directly compared due to validity considerations. Therefore, the interpretation must be done with caution and in general terms only, also affecting the consequences for both conclusions and ability to generalize our results.
Methodological quality in the included studies was found to be moderate to high, but some single studies within our material may not be of sufficient quality or they lack implementation strategies in accordance with recommended guidelines.
Presenteeism seems to have high “face-validity”, indicating that stakeholders, i.e., leaders, employees, and researchers, consider the concept to be a kind of health-related productivity loss. Our results reveal that few have a clear definition of the concept, and half of the studies describe the concept as “productivity loss due to health or lifestyle problems”. Furthermore, in our material, only two studies contained analysis of data within a theoretical framework, thus challenging internal as well as external validity.
Our sampling was mostly completed before the COVID-19 pandemic, and thus it does not include any reviews of WHPP impacting presenteeism from the pandemic. Recent research on telework, telecommuting and remote work, indicate increased sickness presenteeism and basic changes in working life. Our conclusions may be narrowed due to this.
Suggestions for further research
In the field of research, there are several challenges that invoke thorough elaboration: the first priority being to establish a common understanding and definition of the concept of presenteeism. Then choosing relevant theories appropriate to the context explored. Furthermore, the importance of developing a common unified language, measurements and understanding of what influences presenteeism i.e., competence to use the right interventions, is significant. In the light of the pandemic, changes in work conditions and contextual factors are observed, resulting in an expanding of the concept presenteeism, e.g., positively, and negatively effects of presenteeism. This should be further explored. Since both single-component and multi-component program interventions are of importance, more research is needed on analysis of intervention programs to fully comprehend the concept. The incorporation of proper program designs remains a challenge. In practice, there is insufficient knowledge of how to identify different needs at all levels (e.g., screenings) to enable tailored programs to specific subgroups. Lack of knowledge and competence about implementation of sustainable interventions in complex problem areas and settings, still remains. Single component programs implemented at individual subgroup level can be of great importance to the individual with health problems but must not be understood as “WHPP affecting public health”. Such measures do not bring the field further but should be interpreted as rehabilitation programs. They cannot be up-scaled and sustainable “in the real world”. The field is complex and multileveled. The findings of this review are promising; reinforcement of interventions is to be multi-component and implemented in a multilevel fashion to be sustainable and upscaled from project to operation. To secure sustainability of programs, a stable culture must be created, i.e., implemented into business plans, strategies and into the companies’ operating budget. The employer – employee relationship should be further investigated, acknowledging the development of changed working conditions, requiring new leadership competencies and inherently programs targeting supervisors and leaders.
Conclusion
Our study largely revealed a lack of theoretically informed use of the concept presenteeism, resulting in few clear definitions, and many vague descriptions of the concept. This may affect the validity and generalisability of results. A high program diversity were identified, several adaptable to future needs (e.g., digital solutions), however hampered by narrow focus on individual health. Future research should focus on theory-based high quality multilevel WHPP comprising contextual, work, and organisational factors. Increased telework opportunities due to COVID-19 experiences have affected working conditions worldwide. Hence, adaptions are required among employee and management, in addition to an organisational and socio-cultural level.
Footnotes
Ethical considerations
This study, as a literature review, is exempt from Institutional Review Board approval.
Informed consent
Not applicable.
Reporting guidelines
In this study, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) checklist was used.
Acknowledgments
We would like to thank Atle Hårklau, a professional librarian at the University of South-Eastern Norway for her guidance and contribution during the search process in the different databases of academic literature.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
The authors report no funding.