
Abstract
BACKGROUND:
Local anaesthesia is the anaesthetic technique most frequently used in dentistry. Advanced anaesthetic treatments like conscious sedation and/or general anaesthesia are required for major dental surgical procedures. Although general dentists are capable of administering local anaesthesia, additional training is needed for advanced anaesthetic procedures. It is generally disputed whether advanced anaesthetic techniques should be related to one or two dental specialties or whether they should receive a separate degree.
OBJECTIVE:
This paper aims at introducing the field of ‘dental anaesthesiology’ in routine dental practice as applicable within laws laid down for dental and medical specialities.
METHODS:
Publications, articles and mouthpieces relevant to the topic of dental anaesthesiology were identified using various search engines like MEDLINE (via PubMed), EMBASE, and Web of Science. The terms used for the search were ‘Dental anaesthesiology’, ‘General anaesthesia’, and ‘Dental care’. Articles about dental treatment done under anaesthesia were only considered describing various anaesthesia techniques. Additionally, the authors being regular caregivers of dentistry including oral and maxillofacial surgeon have shared their personal experiences and information on the said theme.
RESULTS:
In total, 127 articles were found of which 33 were available as full texts. Unrelated articles from the available full text were excluded. Finally, 17 studies were incorporated into the review. Majority of dental anaesthesiologist has a positive and favourable attitude towards the profession. Pediatric dentistry, oral and maxillofacial surgery, and special needs dentistry are the fields with the highest service demand. Also, the field is lucrative if the practitioner is refined and provides sophisticated services. It is easier and time saving to train the dentists, especially the ones with oral and maxillofacial surgery background.
CONCLUSION:
A degree of dental anaesthesiologist will open new doors to the budding dentist seeking for jobs or wanting to provide the best outcome.
Introduction
Anaesthesia has been one of the pillars of the dentistry, thanks to Dr. Horace Wells who himself was a dentist and is credited for laying a foundation stone for anaesthesia in surgical practices. Since then, dentistry has advanced significantly, while the anaesthesia puzzle has grown more complicated. There is no denying the fact that a practitioner must have a sound medical knowledge before delivering anaesthesia, a task made more challenging by the extremes of age. Both age groups, viz. children and old adults, are also hesitant and worried about the several treatment options that dentistry has to offer. Seldom, many patients might have underlying systemic diseases posing a challenge for the dentist to provide local anaesthetics with vasoconstrictors. Majority of the dental procedures can be conveniently carried out under local anaesthesia, but still a sizable population needs care under more extensive anaesthetic techniques and this is where a chasm of trained personal is felt the most. The dentist and the anaesthesia staff should be careful regarding the probable systems of handling and their complexities. It has been repeatedly demonstrated that the anatomic system and procedures, including the poor selection of the armamentarium, can significantly increase the incidence of serious allergic cases and complicated situations [1]. As professionals, dentists are well-versed in anaesthetic techniques, but in more complex techniques, the lack of minimal monitoring, such as a pulse oximeter to keep a watch on vitals while the procedure is being performed, and the absence of a standby anaesthesiologist, could raise an alarm before the occurrence of serious complications. Here comes the role of dental anaesthesiologists, who are very well versed with the local anatomy and have sound knowledge about the complications that can occur in these regions [2].
For such challenging patients, a dental anaesthesiologist is a crucial prerequisite to avoid treatment plans being compromised. The development of “painless dentistry” and “minimally invasive dentistry” has made patient and dentist cooperation essential for the optimum outcome [3]. Additionally, general dentists are not qualified to do procedures like conscious sedation and general anaesthesia because they lack the expertise necessary to manage the difficulties that may arise. The infection control in dental anaesthesia has been one of the most overlooked aspects. Numerous initiatives have been made to contextualize infection control in dental settings, and it has been established that dentists are particularly exposed to the rapid advancement of contemporary changes to personal protective equipment and infection mitigation techniques specific to sedation and anaesthesia in dentistry [4].
This paper aims at introducing the field of ‘dental anaesthesiology’ in routine dental practice applicable within dental and medical specialities. The purpose of this paper is to introduce the harsh less methods of dental treatment and realise how important it is to deliver atraumatic treatment whether mentally, emotionally or physically based on the sound professionalism related to anaesthesia. Objectives of our piece is to spread the awareness of the need to have specialised care for patients to prevent any untoward sequelae and to provide a sound and professional anaesthetic platform on which dental treatments can be carried out without any hesitations.
Materials and methods
To maintain a codified organization of the study, this review adheres to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) 2020 Statement [5]. The primary outcome was the scope of dental anaesthesiology.
Publications, articles, and other materials pertinent to dental anaesthesia were evaluated as suitable for inclusion in this review after considering the eligibility criteria. Furthermore, articles about dental treatment done under anaesthesia were only considered describing various anaesthesia techniques. Only articles written in English and published within the last five years (30 September 2016 to 30 September 2021) were taken into consideration. Also, studies that did not address the primary outcome were also excluded.
MEDLINE (via PubMed), EMBASE, and Web of Science were among the databases used for the searches. ‘Dental anaesthesiology’, ‘general anaesthesia’ and ‘dental care’ were the search terms used. Additional searches were conducted in the literature reviews on the subject of interest and the reference lists of pertinent studies.
All the studies found through the search strategies were imported into an Endnote library and duplicate studies were deleted. The articles that met the eligibility requirements were chosen after two reviewers (the first and second authors) independently evaluated the records (title and abstract). A third independent reviewer (3rd author) was consulted to resolve any type of disagreement. Following this initial screening, the chosen records were analysed in their full-text version, and two other reviewers (1st and 2nd authors), working independently, decided whether they should be considered for the review. A third author was consulted in the event of a disagreement (3rd author). The data was extracted using a standardized data form by the same two reviewers. Additionally, the authors being regular caregivers of dentistry including oral and maxillofacial surgeon have shared their personal experiences and information on the said theme.
The articles that met the eligibility requirements and those that were excluded during the study selection process were reported using the PRISMA flow diagram (Fig. 1).
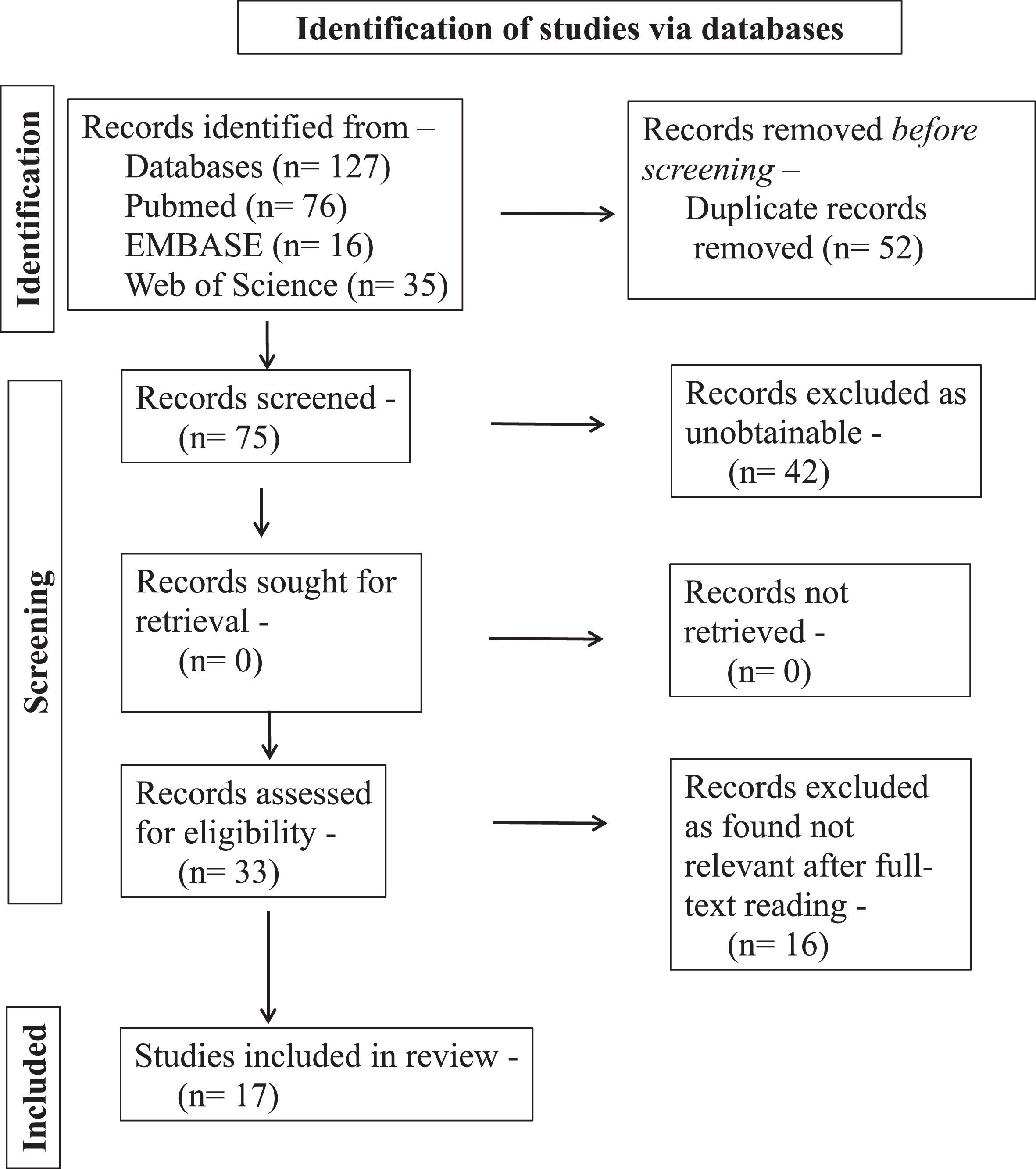
PRISMA flowchart of the study selection process.
Using the search strategy described in the “Materials and Methods” section, 127 articles in total were found of which 33 articles were available as full texts. Unrelated articles from the available full text were excluded. Finally, 17 studies were incorporated into the review.
In total, 127 articles were obtained from the analysis of the databases, adopting the search strategy described in the “Materials and Methods” section. Unrelated articles from the available full text of 33 articles were excluded. A total of 17 studies were finally included in the review.
Scope of dental anaesthesiology
The majority of dental anaesthesiologists have a good and favourable attitude toward their work, according to a recent survey study by Young AS et al. [6]. Oral and maxillofacial surgery, pediatric dentistry, and special needs dentistry are the fields with the highest service demand [6]. If the professional is skilled and offers high-end services, the field is also lucrative. The amount of money an anaesthesiologist earns depends on the following factors [7].
The anaesthesia pay value is calculated by: anaesthesia pay out=(basic value unit+time value unit+modifier unit) * conversion factor [4]. The conversion factor varies from states to countries, for e.g. in USA its $20. An average annual income a dental anaesthesiologist earns in US is approximately $241,500 [3]. Dentists come under the 10% income group in US. In Indian subcontinent, anaesthesiology is essentially a medical specialisation with a pre-requisite of 5 years of medical school training. However, an anaesthesiologist does not have the insight of dentistry and the procedures offered, as they study the body in general and are trained for general medical procedures [8].
Oral intubations and spinal anaesthesia are mainstays in the vast majority of general surgical procedures, and general anaesthetists rarely administer regional head and neck anaesthesia. For general anaesthetists, managing difficult airways while treating patients who have had head and neck injuries and odontogenic infections can be extremely challenging. It is important to note that dentists have specialized and in-depth training on the anatomical features of the head and neck, which have significant implications for the management of challenging airways. Dentists who are experts of the local anatomy can readily master cutting-edge procedures like nasal intubations and fibre optic intubations, occasionally incorporating tracheostomy to by-pass the upper airway to obtain anaesthesia. Not only will it be easier to train dentists, especially those with backgrounds in oral and maxillofacial surgery, but it will also be more efficient and comprehensive. In addition to criteria for selecting cases for dental general anaesthesia, a certain amount of dental practitioner judgment is essential to reach the appropriate conclusions. Instructions given to caregivers prior to and after surgery reduce the possibility of problems. A dual-trained dentist with expertise in resuscitation, meticulous monitoring, and cutting-edge equipment will therefore undoubtedly minimize negative results [9].
Discussion
Dental anaesthesiology strives to provide patients with mild to moderate anxiety with painless and atraumatic dental care without creating the impression that the procedure is frightening [3]. Strong gag reflexes, which in extreme cases could cause circulatory stroke and neural collapse in anxious settings for medically challenged patients, are a challenge that an operating dentist must occasionally deal with. Similar to this, patients who are uncooperative may experience mental or emotional trauma if their family members force them to receive treatment. Therapeutic restraint, whether physical (a parent holding the child) or mechanical (using a papoose), is frequently effective for children who exhibit behavioral resistance to dental treatment. But as individuals grow larger and stronger, its limitations become more apparent. Restraint may make it impossible to provide effective treatment for patients who are demonstrating strong resistance. In fact, aggressive patients may actually be a danger not only to themselves, but also to the dental professionals who are treating them. General anaesthesia is an appropriate alternative in such cases [9].
Hands over mouth, physical immobilization, restraint, or voice control are typical strategies used to manage the behaviour of mentally challenged or paediatric patients. These techniques occasionally have a more devastating effect on a child’s mental health. This unfavourable perception of a circumstance enters the subconscious mind of some sensitive patients, where it eventually transforms into long-term memory by the hypothalamus. So much so that this might eventually lead to depressive disorders, somatostatic illnesses, panic attacks, anxiety, nightmares, and obsessive thoughts. The dentist may also have difficulties when treating a young child who has respiratory issues such chronic obstructive pulmonary disease and numerous systemic illnesses. Another major challenge faced during dental procedure is providing treatment to patients requiring special needs who require manpower to gain control and stabilize. Such acts are considered to be unethical and many a times not approved by the parents as well.
In some studies, the effectiveness of non-pharmacological interventions in reducing mental distress, pain, and analgesic use in adults undergoing dental procedures under regional or general anaesthesia has been compared to standard care alone or an attention control group. The author advises additional high-quality trials to strengthen the encouraging evidence even though hypnosis showed promising results. Also, the authors warranted it can be used as an adjunct only and not the primary mode of stress management [10].
General anaesthesia is a boon is such patients. Just as Dr. Warren famously mentioned at Dr. Morton’s demonstration, “Gentlemen, this is no humbug.” Dr. Warren was astounded that the patient fell asleep peacefully throughout the procedure as opposed to having to endure the agonizing screams that were the standard in those days [11]. This renowned proverb is still true today, more than 150 years later, especially in fields like dentistry. In addition to helping with behaviour management, general anaesthesia also offers some unsaid advantages, such as in cases of abscess, acute pulpitis, and space infections. Failure of local anaesthesia in these situations, where there is persistent discomfort and acute inflammation, is a proven clinical manifestation brought on by an elevated pH, which inevitably results in non-cooperation [12, 13].
Having said that and procedural and ethical considerations apart, general anaesthesia can be a costly affair. The cost of doing surgical procedures under general anaesthesia is enormous. It goes without saying that with a dentist’s understanding of anaesthesia, the procedure may be completed at a considerably lower cost that will be affordable for both the patient and the operating practitioner. For this reason, we must formally integrate the field into the main stream of dentistry.
The world only started to acknowledge dentistry as a profession until Dr. Horace Wells popularized anaesthesiology, and oral and maxillofacial surgery only established a specialty after a group of early exodontists distinguished themselves from their dental peers by embracing general anaesthesia. Modern Oral and Maxillofacial Surgery anaesthesia educators, researchers, and private practitioners must rigorously and wisely improve the modern Oral and Maxillofacial Surgery anaesthetic model on both fronts— clinically and politically— that it was inspired by surgeons like Hubbell in the 1930 s. It will help to conserve its anaesthetic legacy and secure its future preservation if oral and maxillofacial surgery office-based team anaesthesia continues to advance in both art and science [14].
Developing a model that the dental anaesthesiologists will deliver anaesthesia while another practitioner will perform the dental procedures is an arduous task. As this will demand the change in training methods and the budding dentist will have to be trained and taught a new of patient care [15]. The overwhelming majority of dentists who administer advanced forms of anaesthesia in their offices follow the “operator-anaesthesia team model” of anaesthesia delivery, which has a strong safety record [14]. This is an issue of concern because a recognized specialty of dental anaesthesiology might become critical of an established, time-tested and evidenced-based operator-anaesthesia team model. Being granted specialty recognition potentially would lead to a small group of practitioners advising regulators, insurers, and others that the operator-anaesthesia team model needs to be changed. One can easily imagine bureaucratic regulators preventing dentists from administering sedations and general anaesthesia to their patients while performing dentistry, or lead health care insurers to stop paying for anaesthesia administered by the operator and the operator’s team. Such a move would unquestionably restrict access to care to the point where higher treatment costs and delays in the course of treatment would be inevitable. Also, there can be political and bureaucratic ramifications as the dental anaesthesiologists might emerge as the leaders occupying specialty positions in dentistry and intent to work against dentists who deliver their patients’ anaesthesia.
Dental anaesthesia continues to be mostly an unrecognized field even after acknowledged benefits. There are still many concerns among the current population that need to be addressed on various levels if the perception of this field is to alter. There is widespread concern that practitioners of this profession will not add any new knowledge or provide patients with superior care to that provided by current practitioners.
Selection and propagation of a medical specialty is a delicate and meticulous process. The recognition of a new specialty in a health care discipline is and should be difficult to attain and is evident widely wherein lot of hurdles are faced for any field to be called as a speciality [16]. It is imperative that once a profession attains the designation of a specialty, then the training and skills should be in such a way that other professions do not possess. Only then it is appropriate to consider an area of a profession eligible for specialty recognition. For dental anaesthesiology, however, this cannot be said; the skills used by dentist anaesthesiologists are not unique, but are shared by many dentists. As previously said, numerous dentists, generalists and recognized specialists, routinely use advanced ambulatory anaesthesia techniques in their practices. They accomplish this with a safety record that is envious of the few healthcare industries. Additionally, anaesthesia in dentistry is not an end unto itself. Rather, anaesthesia whether local, inhalational, parenteral, or behavioural, is used to accomplish a particular dental goal, like enabling a dental procedure.
It would be overly ambitious to provide support to the needy populace by a very small group of dental anaesthesiologists. Additionally, a small group of dental anaesthesiologists will be given the title of being the leading authority on anaesthesia in dentistry. Individuals within and outside the dental profession will look exclusively to them for advice on issues and topics related to anesthetizing patients in dental offices.
Dentists who prefer to have a dental anaesthesiologist administer anaesthesia for their patients will not be harmed by the lack of a specialty status for dental anaesthesia; such people are and will remain available. The opposite might not be true over time, though. The current system is working well for our patients and ought to be kept in place. Dental anaesthesiologists should continue to think of themselves as dentists who specialize in the administration of anaesthesia, similar to how some dentists in the field of dental implants present themselves as specialists in dental implantology. In these two situations, it is unnecessary to establish a formal specialty and it is possible to minimize the risk of limiting the ability of other dentists to provide related services.
Challenges
As with any worthwhile endeavour, dental anaesthesiology has difficulties that must be overcome. If national health care financing for training programs is reduced, starting new postdoctoral programs or expanding existing ones may face financial difficulties, particularly in developing nations and also in developed countries. Ingenuity will be needed to overcome these obstacles and keep those programs viable despite the ongoing need for services. Additionally, the expense of the institutes is increased by the necessity for significant training facilities for dental anaesthesia students. The financial cost of patients without access to health insurance should not be overlooked. Lastly, in order to ensure that training quality is maintained and to avoid program suspension or closure, rigorous evaluations will be required to help each program make the necessary adjustments.
Limitations
The primary outcome (as mentioned in the “Materials and Methods” section of this review), as indicated in the scope of providing an overall view of dental anaesthesiology, was not described in the literature (therefore in our review), and in some cases it was even missing; The authors have included personal information and experiences in this review that makes the conclusions less reliable; and This review did not take into account the availability of training programs in developing and underdeveloped countries. This was due to limit to any group analysis since only few articles were available in English Literature.
In future, studies are recommended focusing on the scope of dental anaesthesiology in different countries with a special focus on the financial burden on training institutes and patients.
Conclusion
The number of jobs available to new graduates is one reason why many dental graduates are not overly satisfied with the program. Other factors include a lack of government employment, low community awareness of oral health, worry about not receiving the treatment needed, high competition in private practices, and expensive equipment. A dental anaesthesiologist degree will open new opportunities for the aspiring dentist looking for employment or desiring to provide the best outcome. The degree can be earned in two years, which is one year less than the length of time required for the standard postgraduate programs.
Footnotes
Ethical approval
Not applicable.
Informed consent
Not applicable.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
None to report.
Funding
No internal or external funding was received.