
Abstract
BACKGROUND:
The coronavirus disease 2019 (COVID-19) pandemic may cause significant anxiety among healthcare professionals (HCPs). COVID-19-related psychological impacts on HCPs in Western countries have received relatively little attention.
OBJECTIVE:
This study aims to assess the levels of anxiety in HCPs working in the province of Quebec (Canada) during the first wave of the COVID-19 pandemic and identify factors associated with changes in anxiety scores.
METHODS:
An exploratory online cross-sectional survey was conducted among Quebec HCPs from April to July 2020. The Spielberger’s State-Trait Anxiety Inventory (STAI) was used to measure state anxiety among HCPs. Descriptive and multivariate analyses were performed.
RESULTS:
A total of 426 HCPs completed the survey. Anxiety scores ranged from 20 to 75 points, with 80 being the highest possible value on the STAI scale. Being a female HCP [B = 5.89, 95% confidence interval (CI): 2.49–9.3] and declaring having the intention to avoid caring for patients with COVID-19 (B = 3.75, 95% CI: 1.29–6.22) were associated with increased anxiety scores. Having more years of experience was associated with decreased anxiety scores [B = –0.2, 95% CI: –0.32–(–0.08)].
CONCLUSION:
Organizational strategies aimed at preventing and relieving anxiety should target junior female HCPs who express the intention to avoid caring for patients with COVID-19. Seniority could become an important criterion in selecting frontline HCPs during pandemics. Further studies are needed to comprehensively examine the impacts of the COVID-19 pandemic on Canadian HCPs and identify evidence-based coping strategies.
Introduction
The first case of coronavirus disease 2019 (COVID-19) in Canada was diagnosed on January 25, 2020 [1]. The first cases in Quebec, a French-speaking province of Canada, were identified by the end of February 2020 [2]. As of March 30, 2021, thirteen months later, Quebec has reported the second-largest number of cases in Canada with 310,066 people diagnosed with COVID-19 and 10,658 related deaths [3]. Healthcare professionals (HCPs) are at significant risk of contracting the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19, due to repeated exposure to patients, colleagues, and infectious materials, lack of personal protective equipment (PPE), or failure to comply with infection prevention guidelines [4–9]. A higher incidence of the disease has been observed among nurses and female HCPs while higher proportions of deaths have been reported among male and older HCPs [10–15]. Fear of contracting, spreading, and dying from COVID-19, inadequate knowledge of the disease, organizational issues (lack of PPE, ventilators, or intensive-care unit beds, increased workload, rapidly changing protocols . . .), and changes in personal life may cause anxiety and other deleterious psychological impacts (stress, depression, burnout, and post-traumatic stress disorder) among HCPs [16–18]. A recent umbrella review of seven meta-analyses revealed a pooled prevalence of anxiety in HCPs that ranged from 22% [95% confidence interval (CI): 12.7–35.8] to 33% (95 % CI: 24–45) [19].
Studies that have examined human behavior in fearful or anxiety-provoking situations have suggested that fear and individual values can influence decision-making [20–24]. Exposure to infected patients, fear of contracting the infectious pathogen and contaminating family members and friends have already been major stressors for HCPs during previous outbreaks [25–29]. Such stressors have fueled reluctance to care for affected patients in pandemic times among HCPs and may lead to absenteeism or defection [29, 30]. Anxiety in HCPs may also negatively impact the quality of care to patients [31]. Time spent with patients suspected of or diagnosed with COVID-19 and the nature of the exposure to such patients (performing droplet/aerosol-generating procedures, for instance) may vary from one HCP or professional group to another [32–35]. These factors can influence HCPs’ perception of their risk of contracting the SARS-CoV-2 and their anxiety levels [36–38]. Anxiety prevalence and severity may also vary by organization [39], or health jurisdiction [38]. Thus, it seems relevant to further investigate anxiety in HCPs to inform tailored management approaches. Very little research has examined COVID-19-related anxiety in non-Asiatic HCPs [40]. Previous Canadian studies have reported an anxiety prevalence ranging from 47% to 67% among HCPs, and anxiety risk factors included concerns for personal and family wellness and perceived inadequacy of protective equipment and strategies [41–45]. However, these studies targeted HCPs seeking psychological support [41] or physician and nurse subgroups [42, 43]. They involved relatively small samples [42, 43], did not always use validated tools to assess anxiety levels [43] and restricted their analyses to a single anxiety risk factor [44], or did not examine the statistical relationship between anxiety scores and risk factors [42]. In addition, these studies surveyed very few to no HCPs from the province of Quebec despite the important burden of the pandemic in this province [41–45]. Therefore, this study was undertaken to assess the levels of anxiety in Quebec HCPs during the first wave of the COVID-19 pandemic and identify the socio-professional characteristics of HCPs that are associated with changes in anxiety scores. Given the exploratory nature of this study, no a priori hypothesis was formulated.
Materials and methods
Study design, setting, and participants
A web-based cross-sectional survey was conducted among Quebec HCPs working in all healthcare settings. An invitation to participate in the study was sent to regional health organizations, professional societies, the Collège des Médecins du Québec (Quebec College of Physicians), and the Ordre professionnel des inhalothérapeutes du Québec (College of Respiratory Therapists of Quebec). The invitation message contained a link to the study website (http://www.recherche-covid-19.com). The webmaster of each organization was responsible for disseminating the invitation to members via Facebook and mailing lists. According to the snowball sampling technique, the respondents were further encouraged to forward the invitation message to colleagues who might be interested in participating in the study.
Collection tool
The study questionnaire was developed by the research team based on the study objectives, expert opinions, and literature data. Since profession and exposure to infected patients were risk factors for anxiety in previous pandemics [25–29] and some HCPs are said to be reluctant to work during health crises [29, 30], the survey questionnaire was built not only to estimate anxiety scores in HCPs regarding the COVID-19 pandemic but also to document their socio-professional characteristics, assess their degree of exposure and willingness to provide care to patients with COVID-19.
The questionnaire was divided into three sections. The first section included 9 items and allowed respondents to provide their first and last name, profession, postal code, and affiliation. The respondents could also report the presence of COVID-19 cases in their department and whether they had been caring for such patients.
The second section contained 16 items and focused on the respondents’ sociodemographic information (age, gender, relationship status, number of years of work experience, number of dependents), previous diagnosis of COVID-19, previous experience in critical care, and current diseases and medication. Two items asked respondents about their intention to avoid caring for patients with COVID-19: “Are you thinking about or are you looking for means to avoid caring for patients with COVID-19?” hereafter item 22; “If a situation allowed you to avoid caring for someone infected with COVID-19, would you take this opportunity?” hereafter item 25. The first item was dichotomous: “Yes” = 1 and “No” = 0. The second item had three possible values: “Yes” = 2, “not at the moment” = 1, and “No” = 0. Also, two questionnaire items asked respondents about actions taken to avoid caring for patients with COVID-19: “Have you ever taken a measure, which has not worked, to try to avoid caring for someone infected with COVID-19,” “Have you taken any successful action to avoid having to intervene with people with COVID-19?” Both items were dichotomous with two possible values: “Yes” = 1 and “No” = 0.
The third section of the questionnaire consisted of 20 items from the Spielberger’s State-Trait Anxiety Inventory (STAI-Y) (Table 1) [46]. These items constitute a subscale called STAI-Y-1 that is intended to measure state anxiety [47]. STAI-Y has good psychometric properties and has been widely used in research [48–51]. A validated French version of the STAI-Y-1 was used in this study as it is considered to be statistically equivalent to the original version [52]. STAI-Y-1 items are scored on a 4-point Likert scale (1 = “not at all,” 2 = “somewhat,” 3 = “moderately,” 4 = “very much so”). Ten items refer to the presence of anxiety (anxiety-present subscale). Another ten refer to its absence (anxiety-absent subscale) and are reverse scored, 4 meaning “not at all” and 1 meaning “very much so.” The STAI-Y-1 scores can range between 20 and 80, higher scores indicating higher levels of anxiety. The study questionnaire was available online from April 7, 2020, to July 31, 2020.
Items of the STAI-Y subscale intended to measure state anxiety
Items of the STAI-Y subscale intended to measure state anxiety
Categorical variables were reported as proportions and continuous variables, as means and standard deviations (SDs). Complete case analyses were conducted. A variable named “Intention-to-avoid” was created by merging items 22 and 25 which relate to HCPs’ intention to avoid caring for patients with COVID-19 (Table 2). This variable was scored on an ordinal scale ranging from 0 to 3 where 0 means that the respondent answered “No” to both items (no intention at all to avoid caring for patients with COVID-19), and 3 means that the answer was “Yes” to both items (strong intention). The intention-to-avoid score was 2 (moderate intention) when the answer was “Yes” to item 22 and “Not at the moment” to item 25, or “No” to item 22, and “Yes” to item 25. The intention-to-avoid score was 1 (mild intention) when the answer was “yes” to item 22 and “No” to Item 25, or “No” to Item 22 and “Not at the moment” to item 25. The variable “Avoidance” was also created by combining the two variables related to actions taken by respondents to avoid caring for patients with COVID-19, yielding a dichotomous result: “Yes” = 1, “No” = 0.
Components and potential values of the intention-to-avoid score
Components and potential values of the intention-to-avoid score
The STAI-Y-1 anxiety scores are calculated in three steps. First, the aggregate scores for the anxiety-present subscale and the anxiety-absent subscale are calculated by adding up the scores of the items within each subscale. Secondly, the aggregate score for the anxiety-absent subscale is subtracted from that of the anxiety-present subscale. Thirdly, a constant value of 50 is added to the resulting score to obtain the final anxiety score. A multiple linear regression analysis was performed to identify factors that are associated with anxiety scores. The associations between the factors included in the model and the anxiety scores were presented as mean differences in anxiety scores. These differences were reported as unstandardized (B) and standardized Beta coefficients (β) (Table 3). A correlation analysis was performed, and no collinearity issue was found between the factors considered in the model (Supplementary Table 1). A one-way ANOVA was used to compare the means of anxiety scores of the professional groups represented in the study. A 2-tailed p-value < 0.05 was indicative of statistical significance. Statistical analyses were performed using R software (Version 4.0.3, The R Foundation for Statistical Computing, Vienna, Austria).
Factors considered in modeling the anxiety scores, and their coefficient
This study was approved by the Research Ethics Review Board of Laval University (Approval number: 2020-122/16-04-2020). Participants consented electronically to the study before starting the survey. They were provided with all relevant study information and were informed that they could leave the study at any time and that their answers were to remain confidential. The collected data were stored in a secure server at Laval University (Quebec City, Canada) and anonymized before being analyzed.
Results
A total of 557 HCPs answered the questionnaire among whom 131 were excluded as they did not answer all the survey questions. Thus, the analytic sample consisted of 426 HCPs (Table 4). They were mostly female (88%), and aged 18 to 80 with a mean of 13.67 (SD = 9.68) years of experience. Just over half of respondents were nurses or nursing assistants (53%). They worked in various departments mainly in internal medicine (12%), community health (10.33%), emergency (9.62%), and residential and long-term care centers (8.69%). The majority (58%) reported working or having worked in critical care services. Just over half of HCPs (53%) confirmed the presence of patients with COVID-19 in their department and caring for such patients. Almost 6% declared having been diagnosed with COVID-19. Most HCPs lived as a couple (78%) and had children or elderly dependents (62%). Twenty (5%) reported suffering from mood disorders before the pandemic.
Characteristics of the study population (N = 426)
Characteristics of the study population (N = 426)
*Physiotherapist (18), occupational therapist (5), kinesiologist (2), Pharmacist (3), nutritionist (5), speech therapist (2), social worker (2), Management and clerical staff (12), technician (laboratory, cardiology, and medical imaging) (5).
The STAI-Y-1 anxiety scores ranged from 20 to 75 points among respondents, with a quarter of them having scores ranging from 51 to 75 points (Supplementary Table 2). The mean anxiety score for the whole sample was 42 (SD = 11.8). Female HCPs had a mean anxiety score of 43 points (SD = 11.61) and males had a mean of 37 points (SD = 12.03) (Supplementary Tables 3 and 4). The mean anxiety scores in female HCPs ranged from 42 to 45 points across professional groups, with paramedics having the highest mean score. The mean anxiety scores in males varied from 32 to 46 points across professional groups, with orderlies having the highest mean score. There was no statistically significant difference in mean anxiety scores between professional groups whether disaggregated according to gender or not (Figs. 1 2) (Females: F(5,367) = 0.16, p = 0.98; Males: F(5,47) = 1.04, p = 0.40; Both genders: F(5,420) = 0.35, p = 0.88). Thirty-two percent, 13%, and 7% of HCPs expressed, respectively, mild, moderate, and strong intention to avoid providing care to patients with COVID-19. Few HCPs (6.57%) stated having taken steps to avoid caring for patients with COVID-19.
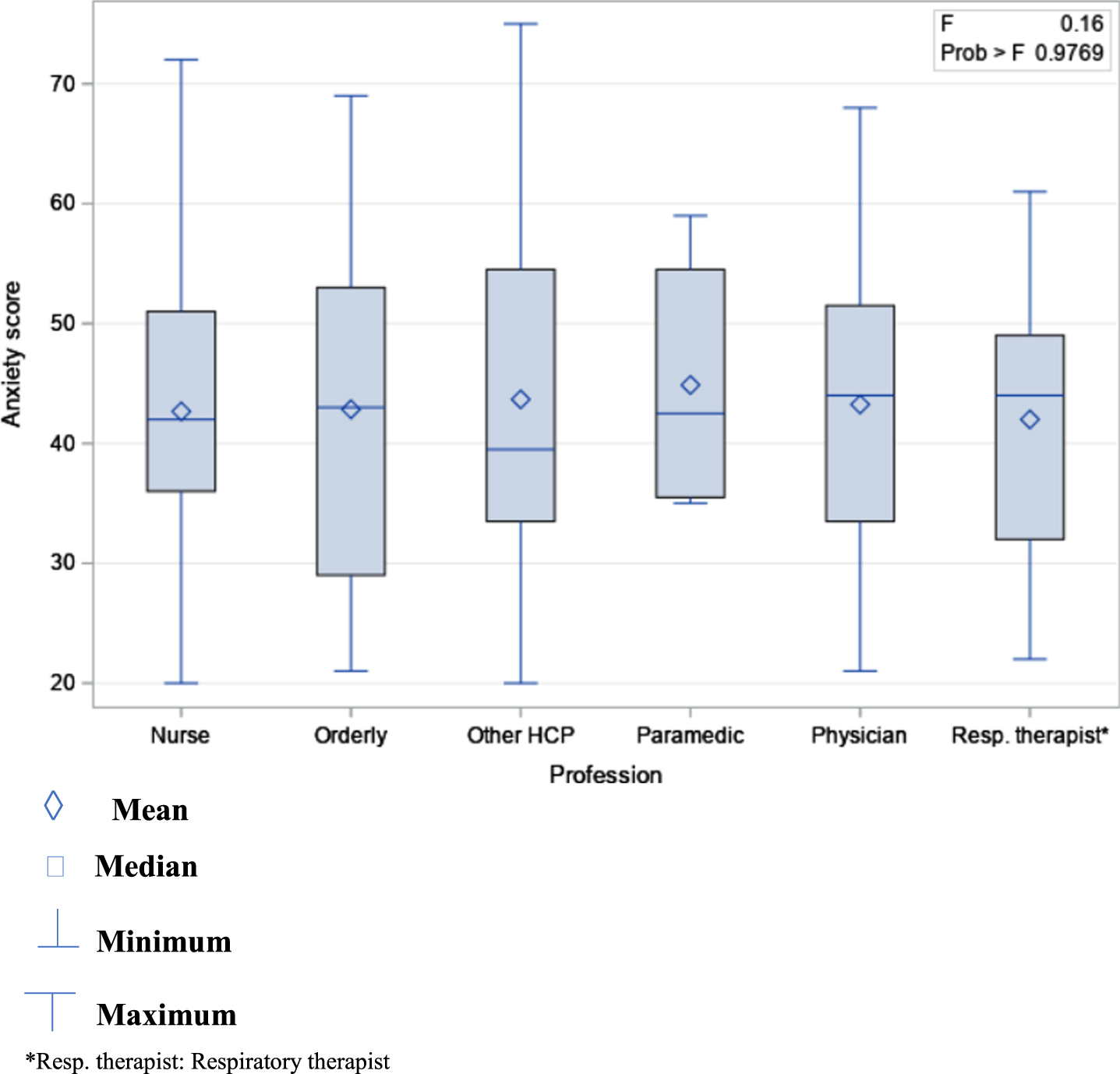
Means of anxiety scores in women by professional group.
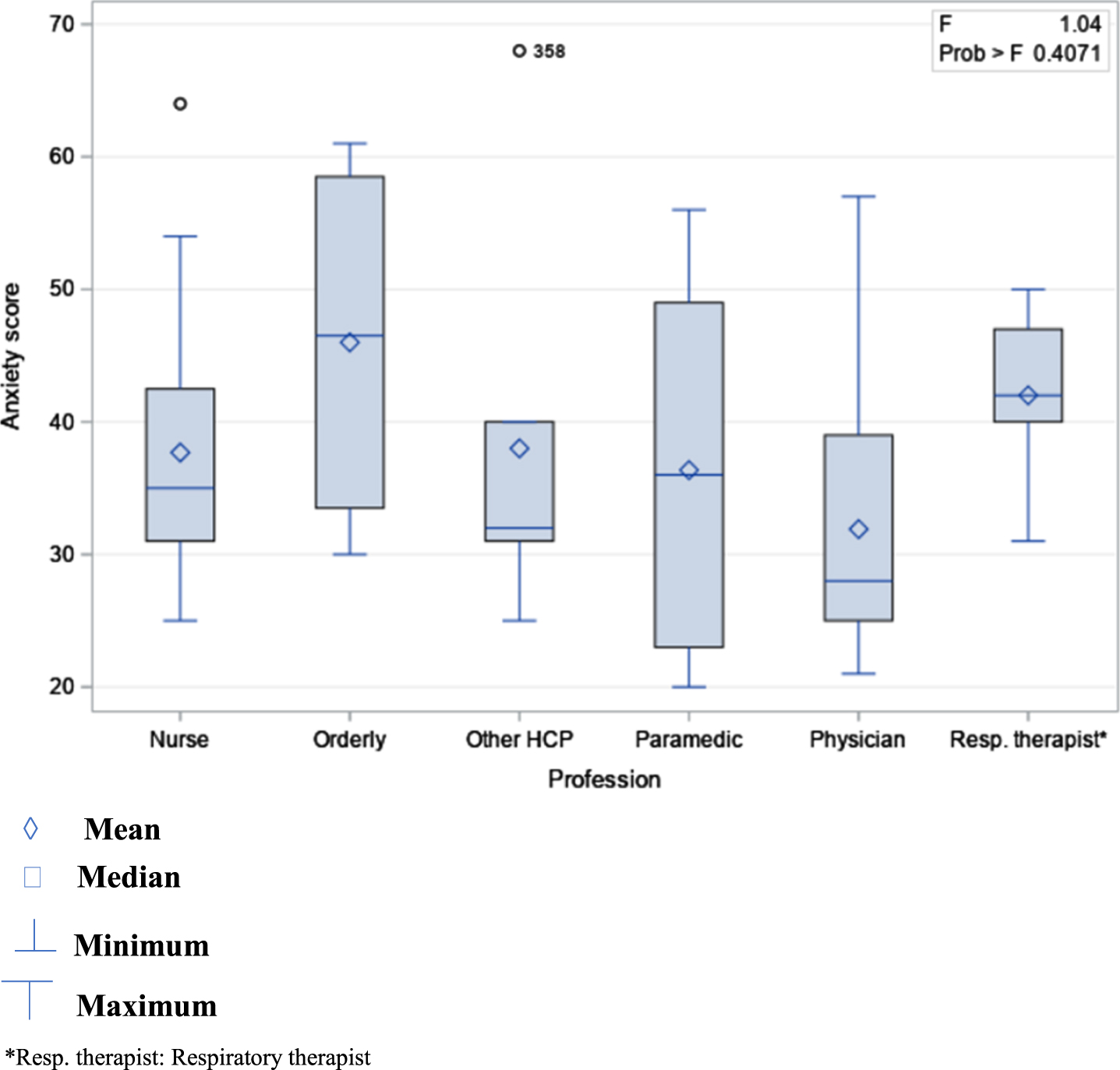
Means of anxiety scores in men by professional group.
Fourteen variables including two dummy variables (Profession and Intention to avoid caring for patients with COVID-19) were entered into the multiple linear regression model which was statistically significant (F(20,405) = 4.2; p < .0001) and explained 13% of the variance of the anxiety scores (adjusted R2) (Table 3). More specifically, this model showed that the mean anxiety score in female HCPs was significantly higher [B = 5.89, 95% CI: 2.49–9.3, p < .0007] than in male HCPs when adjusted for all other factors considered in the model. For HCPs, each year of work experience was associated with a 0.2 reduction in mean anxiety score [95% CI: –0.32–(–0.08), p = 0.001]. The intention to avoid caring for patients with COVID-19 was significantly associated with increased anxiety score. Indeed, HCPs with mild, moderate, and strong intention to avoid providing care to patients with COVID-19 had, respectively, mean anxiety scores of 3.75 (95% CI: 1.29–6.22), 7.63 (95% CI: 4.27–10.99), and 14.62 (95% CI: 9.89–19.36) points higher than the mean score of HCPs who did not express the intention to withdraw from care to patients with COVID-19. Standardized coefficients showed a stronger association between the anxiety scores and moderate (β= 0.21) and strong (β= 0.32) intention to avoid caring for patients with COVID-19 compared to the other factors of the model. No association was found between caring for patients with COVID-19 and anxiety scores. The same trend was observed for living as a couple, having dependents, and a previous diagnosis of COVID-19.
This study showed that, during the first wave of the COVID-19 pandemic, anxiety scores among Quebec HCPs varied widely, with a quarter of them showing scores approaching the highest possible value of the STAI-Y scale. Being a female HCP and declaring having the intention to avoid caring for patients with COVID-19 were both associated with increased anxiety score. Seniority at work was associated with decreased anxiety score.
Few studies have used the STAI-Y scale to evaluate anxiety levels in HCPs during the first months of the COVID-19 pandemic. Mean anxiety scores similar to [53–55] or higher [56–58] than those observed in the present work were reported in such studies. The female gender was also found to be predictive of increased anxiety score among HCPs in previous studies [54, 58–61]. Yet, in Karabulut et al., Turkish male HCPs had a higher mean anxiety score than females [53]. Cultural differences were suggested by the authors to explain such a contrast with published studies. Consistent with our findings, previous studies have revealed a statistically significant association between greater work experience and decreased anxiety score [56, 62]. Nevertheless, in Bahadir-Yilmaz and Yuksel, seniority predicted an increase in scores [58].
Although differences in mean anxiety scores have been previously observed between and within professional groups [54, 63], no statistically significant difference was found in the present study between such groups. The high proportion of women (42% to 93%) across these groups in our study might explain the absence of difference. In line with our findings, Liang et al. found no statistical difference in anxiety levels between frontline and non-frontline HCPs [64]. Conversely, Milgrom et al. found a statistically significant increase in anxiety scores among HCPs working in a hospital providing care to patients with COVID-19 [54]. Several other studies reported higher anxiety scores in frontline HCPs [65–69] whereas Mohd Noor et al. found a higher mean anxiety score among non-frontline HCPs [70]. Furthermore, HCPs have expressed the intention to avoid caring for patients infected with COVID-19 in prior studies [71–75]. Fear of getting infected and contaminating family members, lack of PPE, and excessive workload were among the reasons put forward to justify such a stance.
The factors (gender, seniority at work) found in this study to be associated with increased anxiety scores could be included in the classification made by Vindegaard et al. of risk factors for anxiety among HCPs facing the COVID-19 pandemic [76]. Indeed, in a systematic review, the authors grouped such factors into four categories: 1) sociodemographic factors (age, educational level, marital status, number of children); 2) current or past medical history (psychiatric disorders, substance abuse); 3) psychological and social factors (poor self-perceived health status, pandemic impacts on daily life, lack of family and social support); 4) job-related factors (exposure to patients with COVID-19, lack of work experience, high social media exposure).
Higher anxiety scores in female HCPs, as demonstrated in our study, might have a physiological basis. Indeed, Seo et al. used magnetic resonance imaging to investigate the brain’s response to stress-inducing images in 96 healthy men and women [77]. Men’s brain response to anxiety was characterized by greater activation of areas involved in motor functions, including the caudate, thalamus, midbrain, and anterior cingulate cortex [78–81]. Women were found to produce a greater response in the insula, temporal gyrus, occipital lobe, and prefrontal-parietal cortices which are involved in emotional arousal and regulation, and cognitive processes such as the understanding of self, others, and environment [82, 83]. The authors concluded that women might have difficulty controlling hyperactivity in these areas and might tend to be more involved than men in overanalyzing, rumination, and producing negative thoughts in the face of stressful events, which could increase their risk of developing anxiety disorders.
Furthermore, the association observed here between seniority and decreased anxiety scores might result from the skill proficiency of experienced HCPs, their confidence in their skills, or their psychological preparedness to deal with unexpected challenges and a new threat to their health [84]. Given their position, senior HCPs may also have limited exposure to patients with COVID-19, which may reduce fear, stress, and the risk of developing anxiety [85]. In addition, they may have fewer career goals to pursue, and less financial pressure or family obligations [85, 86] since they may have already achieved some stability in their careers and may be experiencing a sense of accomplishment and satisfaction with such aspects of their life.
Based on our results, surveying HCPs’ willingness to provide care to patients infected with COVID-19 may help identify professionals with increased levels of anxiety. Indeed, in the present study, one third of HCPs expressed a mild to strong intention to avoid providing care to patients with COVID-19. Additionally, anxiety scores tended to increase with a higher intention by HCPs to avoid treating patients with COVID-19. Such intention may be part of the continuum from the perceived threat of COVID-19 to job abandonment through anxiety, and psychological withdrawal [87]. Absenteeism has been observed in HCPs during the first wave of the pandemic and might become an obstacle to continuous delivery of health care and services if not appropriately addressed in pandemic times [88, 89].
The absence of association between caring for patients with COVID-19 and anxiety scores could be explained by HCPs’ perception that such experience may help them grow as a person and professional [72]. Better knowledge of the disease and health safety measures [7, 90], the experience gained since the outbreak of the pandemic [91], and the increased availability of PPE [7] may have strengthened the confidence of Quebec HCPs caring for patients with COVID-19, thus reducing their anxiety level.
The strength of this study lies in reaching a relatively large and diverse sample of HCPs among whom more than half were involved in providing care to patients with COVID-19. It also used a validated tool and multivariate analyses to provide a rare description of state anxiety and associated factors in Canadian HCPs. However, this study has some limitations. The invitation to the study was sent to specific professional societies and health organizations through e-mails and Facebook, thus excluding non-members of such organizations and non-Facebook users who did not receive the survey link by e-mail. Besides, some professional groups including pharmacists, social workers, nutritionists, occupational therapists were not adequately represented. Thus, the study sample might not be representative of the entire Quebec HCPs population, limiting the generalizability of the study findings. We also found that 58% of participants were working or had worked in intensive care units. Such HCPs may have dealt with patients with COVID-19 that were critically ill. The associated psychological distress might have motivated them more to participate in the study than their peers who do not work in intensive care units. This potential selection bias could have led to overestimating the anxiety scores and the outcomes of the regression model. Furthermore, the psychometric properties of the questionnaire items related to the intention and actions taken by HCPs to avoid caring for patients with COVID-19 have not been evaluated. Study data were self-reported, and as such, are subject to social desirability which may lead to overestimating or underestimating anxiety scores, or underestimating scores assigned to the intention or actions taken to avoid providing care to patients with COVID-19. Finally, other risk factors for anxiety could have been considered in multivariate analyses including duration of working shifts, workload, the economic impacts of the pandemic [56], the availability, access, and quality of PPE [92], the frequency, duration, and nature of exposure to patients with COVID-19 [32], familial, social, and organizational support, the adequacy of the information provided about COVID-19, and self-perceived competency in caring for patients with the disease [93]. Sets of these factors could better explain the variance of the anxiety scores.
This study has implications for health personnel management and research. Health organizations should develop interventions to prevent anxiety, screen HCPs, monitor their mental health, and support and orientate those in need towards specialized resources. Preventive interventions should target potential sources of anxiety and could draw from the five lines of action proposed by Shanafelt et al. that consist in 1) listening and acting on HCPs’ perspectives on issues related to the pandemic; 2) reducing their risk of acquiring and transmitting the virus; 3) providing them with training geared towards high-quality patient care; 4) meeting their family and personal needs, both physical and psychological, and 5) providing appropriate responses to the needs mentioned earlier in the event HCPs get infected [94]. Specifically, the availability of quality PPE, adequate workload, staffing and rest time, timely staff turnover, balanced time treating patients with COVID-19, and the development of recreational and rest areas could all be appropriate measures for the prevention and relief of anxiety [42, 95–98]. Clear and coherent recommendations, validated and updated information, avoiding overwatching news on COVID-19, social and familial support may also contribute to maintaining psychological stability [7, 99]. Health organizations should promote positive coping behaviors such as physical activity, meditation, talk therapy, or virtual support groups [100]. They should also encourage HCPs to pursue psychological support as the latter might be reluctant to do so [66]. Evaluating implemented interventions may lead to adjustments of prevention and support programs and identification of cost-effective strategies [97].
Young age, work experience in a previous pandemic, and skills and knowledge about protective measures have been inconsistently reported as likely to lead HCPs to care for patients infected with COVID-19 [73]. Further research is needed to better understand factors associated with HCPs’ willingness to provide care to infected patients during pandemics. Studies examining other potential psychological impacts of the pandemic on Canadian HCPs such as stress, depression, burnout, and sleep disturbances should also be undertaken. Qualitative studies are needed to identify factors that could predict or explain anxiety and other psychological impacts in Quebec HCPs. Furthermore, it is difficult to compare anxiety prevalence and severity in HCPs across studies that used the STAI-Y-1 scale during the COVID-19 pandemic as different cut-off values have been used, and the clinical significance of scores exceeding these values have not been investigated [54, 58]. Thus, studies are needed among HCPs to find consensus on the normative values of the STAI-Y scale, and determine a cut-off point above which clinical anxiety or anxiety disorders can be legitimately suspected. The extent to which scores exceeding the cut-off value impact the quality of patient care should also be examined. Finally, although there was no statistically significant difference between professional groups in this study, the higher mean anxiety score found in orderlies warrants further investigation to confirm the observed trend and identify its determinants.
Conclusion
This study showed that female HCPs with little experience and expressing the intention to avoid caring for patients with COVID-19 may have the highest anxiety scores. Preventive and mitigating interventions should first target HCPs with such characteristics, with the expressed intention to avoid caring for patients with COVID-19 taken as an indicator of the potential presence of symptoms of anxiety among HCPs. Seniority could be one of the criteria to identify the HCPs best suited to be assigned to the frontline during pandemics. The design and implementation of prevention, screening, psychosocial support programs, as well as appropriate treatment of HCPs could pose financial challenges to healthcare systems. However, during pandemics, such interventions have the potential to help retain HCPs, improve their quality of life and experience as professionals, create a sense of self-satisfaction, and ensure continuity and excellence in health care.
Footnotes
Acknowledgments
The authors thank the healthcare professionals who participated in the study for their time and valuable contribution.
Conflict of interest
The authors declare that they have no conflict of interest to disclose.
Data availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author B. P.
Declaration
The authors confirm that they have reported all measures, conditions and data exclusions relevant to the study. A small sample of study participants was subsequently contacted and invited to provide their perspective on qualitative research.
Funding
This study was funded by the Canadian Institutes of Health Research. P.S. received a scholarship from the Department of Family Medicine and Emergency Medicine at the Faculty of Medicine of Laval University.