
Abstract
BACKGROUND:
Chronic pain conditions such as low back pain, knee pain and cervical pain are highly prevalent among female teachers. Chronic pain significantly affects the mental health, sleep and quality of life among teachers.
OBJECTIVE:
This study is intended to investigate the impact of a workplace yoga intervention on musculoskeletal pain, anxiety, depression, sleep, and quality of life (QoL) among female teachers who had chronic musculoskeletal pain.
METHOD:
Fifty female teachers aged between 25–55 years with chronic musculoskeletal pain were randomized to either the yoga group (n = 25) or the control group (n = 25). The yoga group received a 60-minute structured Integrated Yoga intervention (IY) four days a week for six consecutive weeks at school. The control group received no intervention. Outcome measures: Pain intensity, anxiety, depression, stress, fatigue, self-compassion, sleep quality, and quality of life were assessed at the baseline and six weeks.
RESULTS:
A significant (p < 0.05) reduction in pain intensity and pain disability in the yoga group was observed after 6-week compared to baseline. Anxiety, depression, stress, sleep scores and fatigues also improved in the yoga group after six weeks. The control group showed no change. Post score comparison showed a significant difference between the groups for all the measures.
CONCLUSION:
Workplace yoga intervention is found to be effective in improving pain, pain disability, mental health, sleep quality among female teachers with chronic musculoskeletal pain. This study strongly recommends yoga for the prevention of work-related health issues and for the promotion of wellbeing among teachers.
Introduction
Teachers help to shape young minds and turn them into responsible citizens of society. In addition to teaching, teachers are involved in various other activities such as participating in meetings, committees, assignments, assessments, and counseling in the school which contributes to increased burden. Evidence indicates that a significant number of teachers experience stress and burnout. Particularly female teachers find it more challenging compared to male teachers as they have added responsibilities of household activities, including caring for children and/or the elderly at home. Such stressors often contribute to increased burnout, stress and poor mental health, contributing to chronic musculoskeletal problems (cMSP) [1, 2].
The pain related to muscles, bones, ligaments, tendons, and nerves is called musculoskeletal pain. cMSP is one of the frequently reported health issues among teachers contributing to significant disability and distress [3]. Teaching involves task such as standing for long hours, blackboard activities, talking, monitoring, and mentoring, and teachers are expected to stand for a long time [4, 5]. Such activities often lead to pain in the wrist, low back pain, neck pain, shoulder pain, and pain in the knees and hip, which are common cMSP sites among teachers [6].
The prevalence of cMSP among teachers varies between 50–84% and and it ranges from 50–70% among Indian teachers [7, 8]. In a survey study of 525 Brazilian teachers (452 females teachers), a 73% prevalence of cMSP was reported [9]. In another study, teachers from 15 primary schools were followed up for six months. The study revealed that 80% of teachers had musculoskeletal disorders during the study period, and the musculoskeletal problem was associated with increased depression [10]. In another study among 1482 teachers in Malaysia, 40% teachers had low back pain, and 60% had neck pain in the past 12 months [11].
cMSP among teachers is found to be multifactorial in origin. Factors such as mental health, social factors, individual habits and lifestyle, physical activity, and gender (females are more prone) are found to be common causes. Evidence suggests that female teachers have a heightened risk of cMSP compared to their male colleagues; this could be due to lower pain thresholds and pain tolerance among females [12–14]. Furthermore, teachers are often paid less compared to the amount work load they have. cMSP has a negative impact on sleep quality. A study among 242 teachers reported that teachers who had poor sleep quality have two times greater pain compared to teachers who had better sleep quality [15].
Evidence suggests that psychological factors contribute to increased incidences of exacerbation of cMSP [16, 17]. Psychosocial factors such as increased stress, poor social support, low job satisfaction, and increased workload are found to be associated with an increased risk of cMSP among teachers [18–20]. Depression and anxiety are highly prevalent psychopathologies among individuals with chronic pain [21]. Both contribute to increased pain and pain-related disability among such individuals [22]. Evidence also suggests that female teachers have higher anxiety and depression compared to male teachers [23]. In a study, self-reported low back pain was found to be associated with anxiety, depression and stress among teachers, and in the same study, self-reported neck pain was associated with anxiety, depression, and poor mental health [24]. Teachers with cMSP tend to opt for more sick leaves, absenteeism, and early retirement more often than controls [25]. cMSP affects work efficacy, enthusiasm, and concentration. Disability due to chronic pain also has a negative impact on the quality of life [26].
Yoga is a traditional system of mind-body practice that aims to correct bio-rhythms through a harmonious connection between mind, body, and breath. Yoga practice reduces stress and relaxes the mind and body. It also enhances autonomic balance, metabolism, and endocrine functions [27–29]. Studies have demonstrated that yoga improves pain, spinal flexibility, and quality of life in patients with chronic musculoskeletal pain, such as low back pain [30]. Previous studies have demonstrated the feasibility and efficacy of workplace yoga among different working professionals. Workplace yoga is found to be effective in improving the physical and mental health of employees [31, 32]. Studies have reported a positive impact of spiritual practices and prayers among teacher with stress and burnout [33, 34]. Literature suggests a lack of yoga studies on cMSP among teachers.
Thus, the current study intended to investigate the effect of 6-week workplace yoga intervention on pain intensity, severity, and sleep quality, and mental health measures among female teachers with chronic musculoskeletal pain.
Methods
Participants
Participants in this study were female teachers with cMSP working in secondary schools.
Ethics compliance
The study was approved by the Institutional Ethics Committee (IEC) of Swami Vivekananda Yoga Anusandhana Samsthana (SVYASA University) (IEC No. RES/IEC-SVYASA/135/2019).
Inclusion and exclusion criteria
Consenting female teachers within the age group 20–50 years with pain disability index score > 30 were recruited into the study. We chose only female teachers because we intended to study the impact of yoga exclusively among female teachers as their there stress levels are completely different and they are more vulnerable for cMSP compared to male teachers.
Participants who had uncontrolled diabetes, thyroid function disorders, uncontrolled hypertension, heart disease, psychiatric medications, morbid obesity, pregnancy, or abdominal surgery within the past 1-month were excluded from the study. In addition, participants who had previous exposure to any form of yoga in the past one year (with regular practice for more than one month in the past one year) were also excluded from the study.
Procedure
Two private English-medium schools were selected for the study. An advertisement about the study was published on the notice board of the two schools and interested participants were interviewed for eligibility. A total of 98 teachers were screened for eligibility criteria. Forty-eight participants were excluded; of these, 38 had exclusion criteria, five refused to participate, and five were not convinced with intervention. Fifty were randomized into either yoga group or control group.
Randomization
Randomization was done in two stages using a computer-based random number generator (https://www.google.com/search?q=random+number). All participants’ names were arranged in alphabetical order, and then they were numbered from 1– 50. Two groups were formed (consisting of 25 members in each group); group A and group B were obtained using a computer-based random number generated. The toss method was used to assign one set for intervention and the other for the controlgroup.
Randomization was done by an independent computer expert who was not associated with the study and was blind to the groups. Allocation concealment was followed during randomization.
Intervention
Participants in the yoga group received a 60-minute integrated yoga session each day, four days a week, for six continuous weeks. Participants in the yoga groups were advised to attend either enter every day’s or daily yoga session between 4:30–5:30 PM at the school. Participants were advised to come for a yoga session on an empty stomach/minimum of 2 hours after the meal. They were encouraged to wear stretchable and comfortable clothes for yoga practice. After yoga sessions, participants were encouraged to ask the yoga expert to address their yoga practice queries. A certified trained yoga expert administered yoga sessions. A structured yoga module consisting of loosening practices, yoga poses, breathing practices, relaxation techniques, and meditation was used (Table 1).
Yoga module
Yoga module
The control group participants did not receive yoga intervention, and they were advised to follow their routine activities. No major change in diet and physical activity were noted in the control group during the study period.
The assessments were performed by a team consisting of a psychologist and two assistants. This team was blinded to the groups. All the assessments were performed twice: at baseline and after 6-weeks. Baseline assessments were performed prior to randomization. Scoring and data entry were done by the assessment team.
Primary outcome measures
Pain disability
Pain Disability Questionnaire (PDQ): It is considered a valid and reliable tool to assess pain-related disability in patients with chronic musculoskeletal pain [35] with Cronbach’s alpha 0.96 [36]. This is a self-reported questionnaire that evaluates a patient’s perceived disability due to pain. The patient is asked to rate how pain has restricted their routine activity on a 0–10 scale; the higher the score, the greater the perceived disability. PDQ scores between 0–70 indicate mild/moderate disability; 71–100 indicate severe disability, and 101 and above indicate extreme disability. Also, PDQ measures both physical and psychosocial factors indecently.
Pain assessments
a) Numerical Pain Rating Scale (NPRS)
It assesses the pain severity in various pain conditions including cMSP. The patient is expected to rate their subjective pain feeling on a 0 to 10 scale, with 0 being no pain and 10 being extreme pain. NPRS is recognized as a valid tool to assess pain severity in musculoskeletal pain patients. It is a valid tool to measure pain intensity [37]. Its test– retest reliability was found to be varying from 0.67 to 0.96, with convergent validity from 0.79 to 0.95 [38].
b) Sleep quality
PSQI is considered a valid and reliable tool with a test-retest reliability of 0.87. It is a widely used tool to assess subjective sleep quality in both clinical and non-clinical populations. It consists of six aspects of sleep: sleep quality, sleep latency, sleep duration, sleep disturbance, daytime dysfunction, and medication use. A global score of 0– 21 is possible, wherein a score over five is considered sleep impairment [39].
c) Secondary outcome measures
Psychological measures
Stress, anxiety, and depression were measured using the Depression, Anxiety, and Stress Scale 21 (DASS 21).
a) DASS 21
DASS 21 is a valid and reliable questionnaire that assesses subjective depression, anxiety, and stress in both clinical and non-clinical populations. This scale consists of 3 subscales of 7 items; each subscale measures depression, stress, and anxiety. The depression scale measures dysphoric mood states, a feeling of hopelessness, and low interest. The anxiety scale assesses anxious mood, autonomic arousal, and muscle tension. The stress scale assesses emotional vulnerability to stressor and tension [40]. Its Cronbach’s alpha was found to be 0.83 [41].
b) Quality of life was assessed using WHO-QoL-BRIEF
WHO-QoL-BRIEF is considered a valid tool to assess subjective quality of life. It consists of 26 questions, wherein participants rated on a 5-point Likert scale their perception about the quality of life in the past four weeks. WHO-QoL-BRIEF consists of four domains. These domains assess four aspects of life: physical health, psychological health, social relationship, and environment [42].
c) Physiological assessments
Systolic and diastolic blood pressure and pulse rate were also assessed in the morning session between 9– 10 am. Participants asked to relax for 10 minutes before assessment. OMRAN electric BP measuring device was used. Body Mass Index was calculated using height and weight. Formula: BMI = Weight (kg)/Height (M)2.
Ethical comply
The institutional Ethics Committee approved the study (Approval no. RES/IEC/SVYASA/135/2019). The study was conducted in accordance with the Declaration of Helsinki for research that includes human subjects. The study was conducted between August 2019 and January 2020. All participants signed a written consent form, which was explained orally. Participants were explained that they could walk out of the study at any point during the study if they wished, and patients’ information was kept confidential. The group was offered yoga sessions after the study period was over.
Statistical analysis
Continuous variables were represented as mean±S.D., whereas; categorical variables were represented as numbers (percentage). ANOVA model was run to assess the treatment effect across the two study groups. The between-subjects model factor was group, and within-subjects factors were time (pre and post) and interaction of group by time. Paired sample t test was used to ascertain the within-group treatment effect from baseline to follow-up. p < 0.05 was considered as statistically significant throughout the analysis. Stata ver. 13.1 was used for statistical analysis. Independent variable was yoga interventional and pain measures, anxiety, depression stress and quality life were the dependent variables.
Results
Five teachers in the yoga group and seven teachers in the control group dropped out due to personal reasons (See Fig. 1). Twenty teachers in the yoga group and eighteen in the control group completed the study.
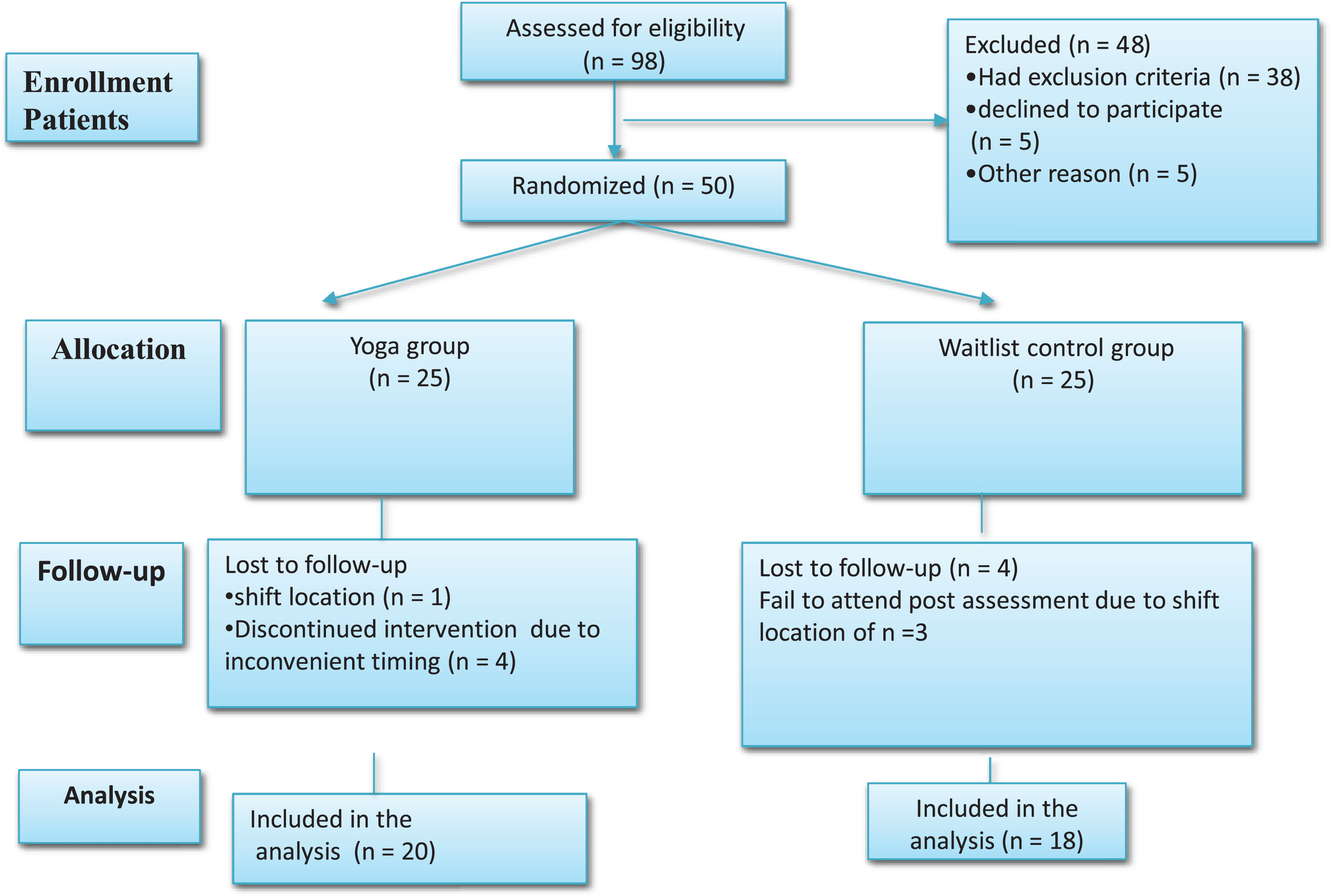
CONSORT flowchart.
The average age and baseline score for all the assessments are depicted in Table 2. Both groups were comparable at the baseline in terms of BMI, years of experience, age, duration of the pain, and working hours in the school (Table 2).
Baseline characteristics of the participants
Abbreviations: BMI-Body Mass Index, SBP-Systolic Blood Pressure, DBP-Diastolic Blood Pressure, QoL - Quality of life, PSQI-Pittsburgh’s Sleep Quality Index, FSS-Fatigue Severity Index, PDI-Pain Disability Index, NPRS-Numerical Pain Rating Scale, VPRS-Visual Pain Rating Scale, SC-Self compassion. No significant difference was observed on baseline comparison.
A statistically significant decrease in the SBP, DP, and heart rate was noticed in the yoga group post-intervention compared to the baseline.
At 6-week, in the between groups comparison there was a significant difference in all the variables except pulse, physical domain of QoL, and stress. This suggests a positive impact of 6-week yoga intervention on cardiac parameters, mental health measures, QoL, and sleep quality measures (Table 3).
Physiological measures
Physiological measures
Abbreviations: BMI-Body Mass Index, SBP-Systolic Blood Pressure, DBP-Diastolic Blood Pressure.$Within group pre-post comparison. @Between group post intervention comparison.
A significant decrease in the pain disability and pain intensity in the yoga group compared to the control group was noticed (Table 4) at 6 weeks.
Changes in pain measures
Abbreviations: PDI- Pain Disability Index, D1-, D2-, NPRS-Numerical Pain Rating Scale, VPAS-Visual Pain Assessment Scale. $Within group pre-post comparison. @Between group post intervention comparison.
Anxiety, depression, stress, and fatigue decreased after 6 weeks compared to the yoga group’s baseline compared to the control group (Table 5).
Changes in the psychological measures
Abbreviations: SC- Self Compassion, PSQI- Pittsebrg’s Sleep Quality Index. $Within group pre-post comparison. @Between group post intervention comparison.
In the yoga group, there was a significant decrease in the score of anxiety (–54%, d = 0.78), depression (–54%, d = 0.7), and stress (–34.5%, d = 0.5) of DASS-21 after 6 weeks compared to baseline. Similarly, global sleep quality improved significantly (–32.3%, d = 0.72), among sleep measure daytime dysfunction (–35%, d = 0.44) and habitual sleep efficiency (–88%, d = 0.8) improved significantly.
Significant improvement in all domains of the QoL was found in the yoga group at 6 weeks compared to baseline. No change was noticed in the control group. There was a significant difference in the between-group comparison (Table 6).
Changes in the quality of life measures
$Within group pre-post comparison. @Between group post intervention comparison.
In the yoga group in the first week of the intervention, 5 teachers reported an increase in body ache. This could be in response to stretches during asanas practice, which got resolved after the 2nd week of the intervention. Overall, no serious symptoms due to yoga practice were reported during the 6-week yoga intervention.
This study reports a positive impact of a 6-week yoga intervention on pain measures, anxiety, depression, stress, fatigue, sleep quality, and quality of life among female teachers with cMSP pain. Musculoskeletal problems are the most common problems among teachers that significantly affect the mental health and quality of life of the teachers. This study suggests the usefulness of yoga intervention at school in the prevention and management of cMSP among female teachers.
We observed improvement in physiological measures and anxiety in the yoga group, which is suggestive of improvement in autonomic balance following yoga intervention, as reported in several studies [43].
Previous studies on yoga have reported improved chronic pain [44, 45], mental health domains, sleep quality, and quality of life [46–48] following yoga intervention.
Previously, in an randomized controlled study, Karen et al. compared the impact of a 6-week yoga, exercise, and self-care book intervention on back-related functional status and bothersome among 110 chronic low back pain patients. Thirty-four patients received yoga, 32 accepted activities, and 29 followed self-care [49]. This study reported that yoga intervention was superior to exercise and self-care books regarding back-related functions at 6 weeks. Another study by Cramer et al. reported significant improvement in pain functional disability and quality of life following a 9-week yoga intervention as compared to home-based exercise among patients with chronic neck pain [50]. The findings of the present study also align with the observations of Cramer and Karen. However, neither included teachers.
Previous studies on yoga have reported a positive impact of yoga on mental health. A study by Shohani et al. reported a significant improvement in stress, anxiety, and depression following a 4-week yoga intervention of 3 sessions/week [51]. In the present randomized controlled study, we also observed a significant decrease in anxiety, stress, and depression in the yoga group. Further, in our study, we observed that the number of teachers with clinical depression, anxiety, and higher stress at the baseline significantly reduced after an intervention, whereas, in the control group, it significantly increased.
Chronic pain has a significantly negative impact on the quality of life. Yoga has been found to be an effective intervention in improving the quality of life in chronic pain conditions such as chronic low back pain. In a study by Nitin et al., 44 female nurses received a 6-week yoga intervention, and another group of 44 nurses served as a control group. Post-intervention, nurses in the yoga group demonstrated significant improvement in physical, psychological, and social domains of life [52]. Similar results have been found in the present study also.
Similarly, a study by Wieland reported a significant improvement in the quality of life of CLBP patients following one week of residential yoga intervention [53]. There is a negative correlation between pain with sleep quality. Poor sleep quality often worsens the existing pain and contributes to an increase in the need for medication. It contributes to the deterioration of mental well-being.
Yoga has been shown to have beneficial effects on sleep quality in patients with chronic pain. Previously, in a multicenter, randomized controlled trial study, a 4-week yoga intervention produced significant improvement in different sleep domains such as subjective sleep quality, daytime dysfunction, wake after sleep onset, sleep efficiency, and medication in patients with cancer [54]. Further, studies on spiritual practices have reported a positive impact of such practices on the mental health of employees [55].
The present study also confirms yoga’s positive role in stress prevention and the promotion of physical and mental health. To the best of our knowledge, the present study is the first to report yoga’s efficacy among female teachers with cMSP. Previously, Rao et al. reported significant mental health and sleep quality improvements among female teachers following 4-week yoga-based meditation (MSRT) intervention [56]. This study differs from the present study regarding the type of intervention, assessment, and population.
The present study results suggest the potential role of yoga in the prevention of cMSP and associated psychopathology and poor quality of life among female teachers. In addition, yoga may also contribute to enhanced productivity and enthusiasm in teaching.
Improvements in pain following yoga intervention may be attributed to modulation in pain perception, pain tolerance, and reduced muscle ischemia by enhancing micro-circulation. Various yoga postures, breathing practices, and meditation techniques increase the practitioner’s attention to inner sensations and enhance non-reaction to unpleasant sensations such as pain. This contributes to the increased pain tolerance [57]. Further, yoga is known to enhance circulatory endorphins and serotonin levels, which have analgesic effects [58]. It also improves melatonin, GABA levels, reduces sympathetic over activity, and enhances vagal tone; these changes might enhance the quality of sleep and mental health [59]. Improvement in overall activity, mood, and functionality may facilitate improvement in the quality of life. The present study has several limitations, such as small sample size, short-term intervention, and lack of objective assessment methods. Further studies addressing this limitation are warranted. This study lacked the studying of mechanisms of action of yoga.
Conclusion
cMSP is a commonly reported health issue among teachers. It may have significant negative impact on mental health, sleep and quality life. The present study provides beneficial effects of yoga intervention at school in improving cMSP, mental health, sleep, and QoL measures among female teachers with a pain disability. This study recommends yoga practice at workplace to manage musculoskeletal pain and mental and sleep quality among teachers. Further studies with a larger sample size and long-term intervention using objective assessment methods are warranted.
Ethical approval
The study was approved by the Institutional Ethics Committee (IEC) of Swami Vivekananda Yoga Anusandhana Samsthana (SVYASA University) (IEC No. RES/IEC-SVYASA/135/2019).
Informed consent
All study participants were informed about the study protocol and their duly signed written consent form was obtained prior to the study commencement.
Conflict of interest
The authors declare no conflict of interest.
Footnotes
Acknowledgments
The authors thank all the administrative staff of the school for their valuable support and cooperation during the study.
Funding
This study was not funded by any government or private funding agency.