
Abstract
BACKGROUND:
Today, 24% of college and university students are affected by a chronic health condition or disability. Existing support programs, including disability services, within colleges and universities are often unaccustomed to addressing the fluctuating and unpredictable changes in health and functioning faced by students with severe chronic illnesses. This situation is especially difficult for students with lesser-known, invisible diseases like Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), a complex disease affecting up to 2.5 million Americans which often begins in late adolescence or young adulthood.
OBJECTIVE:
Educate occupational therapists (OTs) about ME/CFS and steps they can take to assist students.
METHODS:
This work is based on a review of the scientific literature and our collective professional/ personal experiences.
RESULTS:
ME/CFS’ effects on multiple organ systems combined with the unusual symptom of post-exertional malaise frequently and substantially decrease function. Currently, no effective disease-modifying treatments have been established. Nevertheless, OTs can help student maximize their participation in university life by identifying potential obstacles, formulating practical solutions and negotiating with their institutions to implement reasonable, environmental accommodations.
CONCLUSIONS:
Through understanding this disease, being aware of possible support options, and recommending them as appropriate, OTs are in unique position to greatly improve these students’ lives.
Keywords
Introduction
Medical advances over the last four decades have led to increased life expectancy and function of children with serious, chronic medical conditions. For example, the median age of death for children affected by cystic fibrosis increased 85%, from less than 20 years of age in 1980 to 37.5 years of age by 2006 [1]. At the same time, conditions like attention-deficit/hyperactive disorder (ADHD) are being increasingly diagnosed [2]. Today, 24% of college and university students may have a chronic health condition or disability [3].
One mission of universities is to provide a pipeline of educated, skilled workers who can contribute to the future productivity and sustainability of a society. Higher educational attainment is associated with a host of significant outcomes including improved health, higher mean incomes, lower incarceration rates, and increased civic engagement [4]. Yet, compared to their healthy peers, chronically ill young adults are half as likely to graduate from college and work full-time and face twice the risk of depending on public financial assistance [5]. Thus, whether from an economic, legal, public health, social equity, or other perspective, it behooves universities to seek out and adopt methods to accommodate chronically ill students.
Over the years, universities have attempted to respond to these challenges by creating disability services offices, where “disability” is traditionally conceived of as permanent, fixed physiological changes, such as blindness, deafness, or spinal cord injury necessitating the use of a wheelchair. Accommodations that have been designed for students with “traditional” disabilities typically do not address the waxing and waning and unpredictable demands faced by students with chronic illnesses (e.g., relapses, unexpected hospitalizations, medication changes, sudden stimulus overload) that come up against the rigid timelines of degrees and regimented grade/competency requirements [6–8]. Failing these, in turn, affects students’ eligibility for financial aid and merit scholarships. This situation is especially aggravated when students with lesser-known, chronic medical conditions arrive on campus. Overall, existing efforts have fallen short of transforming disabling environments into usable and inclusive environments in higher education [9].
Who is affected by Myalgic Encephalomyelitis/Chronic Fatigue Syndrome?
Among such conditions is Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), a chronic, complex, disabling medical condition which, according to the National Academy of Medicine, affects between 836,000 and 2.5 million Americans [10]. This condition affects men, women, and children of all races, ethnicities, and socioeconomic backgrounds [11]. Some studies suggest that certain people of color and people from financially impoverished backgrounds might be at higher risk of ME/CFS although they are less likely to be diagnosed and treated properly [12].
ME/CFS often begins between the ages of 10 and 19; additionally, about 10% of people afflicted with Epstein-Barr virus (EBV) mononucleosis (“mono”) will develop this condition [13–16]. In 2015, the American College Health Association found that 1.5% of college students were diagnosed with EBV mononucleosis each year, which corresponds to 0.15% potentially developing ME/CFS annually [17]. Applying this to the 2017 estimated college student population of 18.4 million, this translates into at least 27,600 students affected annually [18]. Actual figures may be higher due to enrollment of already-sick students, affected students continuing to be sick, and development of ME/CFS following other infections or events [19]. Consequently, universities are likely to encounter students with ME/CFS.
Lack of education and accurate information among healthcare professionals
Unfortunately, most of the public and even medical professionals are unaware of this condition and rely on inaccurate/outdated information and practices. Only half of medical textbooks and one-third of medical schools even superficially mention ME/CFS [20]. According to one research group, occupational therapists (OTs) appear to be no better informed [21]. When surveyed, most healthcare professionals stated that they felt uncomfortable diagnosing or treating the illness [22]. Thus, up to 90% of people affected by ME/CFS remain undiagnosed, or they are misdiagnosed, often with depression, anxiety, or even malingering [10]. Perhaps because some information on ME/CFS is based on obsolete, limited, or flawed studies, patients continue to report negative attitudes and inappropriate treatments from medical providers [23].
The valuable role of occupational therapists
A major goal of occupational therapy is to help individual patients live life to its fullest despite injury, illness, or disability [24]. OTs possess the unique skills and experience to assess the obstacles facing students, formulate possible solutions to overcome them, and advocate for those solutions to be put in place. According to one definition of advocacy carried out by OTs, “Advocacy is a client-centered strategy involving a variety of actions taken by the client and therapist, directed to the client’s environment to enact change for the client such that engagement in occupation is enhanced through meeting basic human rights or improving quality of life” [25]. OTs also bring professional authority that students, families, and caregivers may not possess when advocating for and negotiating accommodations with professional staff and faculty of higher education institutions.
This document is intended to serve as a brief, practical resource for OTs working with adult students afflicted by ME/CFS. We will describe what ME/CFS is, basic principles of medical treatment, and how OTs can help. This document is also relevant and helpful for university staff and faculty members as well as students who suffer from ME/CFS.
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
2015 National Academy of Medicine diagnostic criteria
In 2015, the National Academy of Medicine published new diagnostic criteria for ME/CFS, highlighting and mandating the hallmark symptom of post-exertional malaise (PEM) (Fig. 1) [10]. PEM is an exacerbation of some or all of an individual patient’s baseline symptoms following physical and/or cognitive activity. The other symptoms that must be present for a ME/CFS diagnosis are a substantial decrease in function accompanied by fatigue, unrefreshing sleep, and either problems thinking or orthostatic intolerance (difficulty maintaining an upright standing or sitting position without experiencing fatigue, confusion, lightheadedness, nausea, etc.). All symptoms must be of at least moderate intensity and have occurred regularly for at least 6 months.
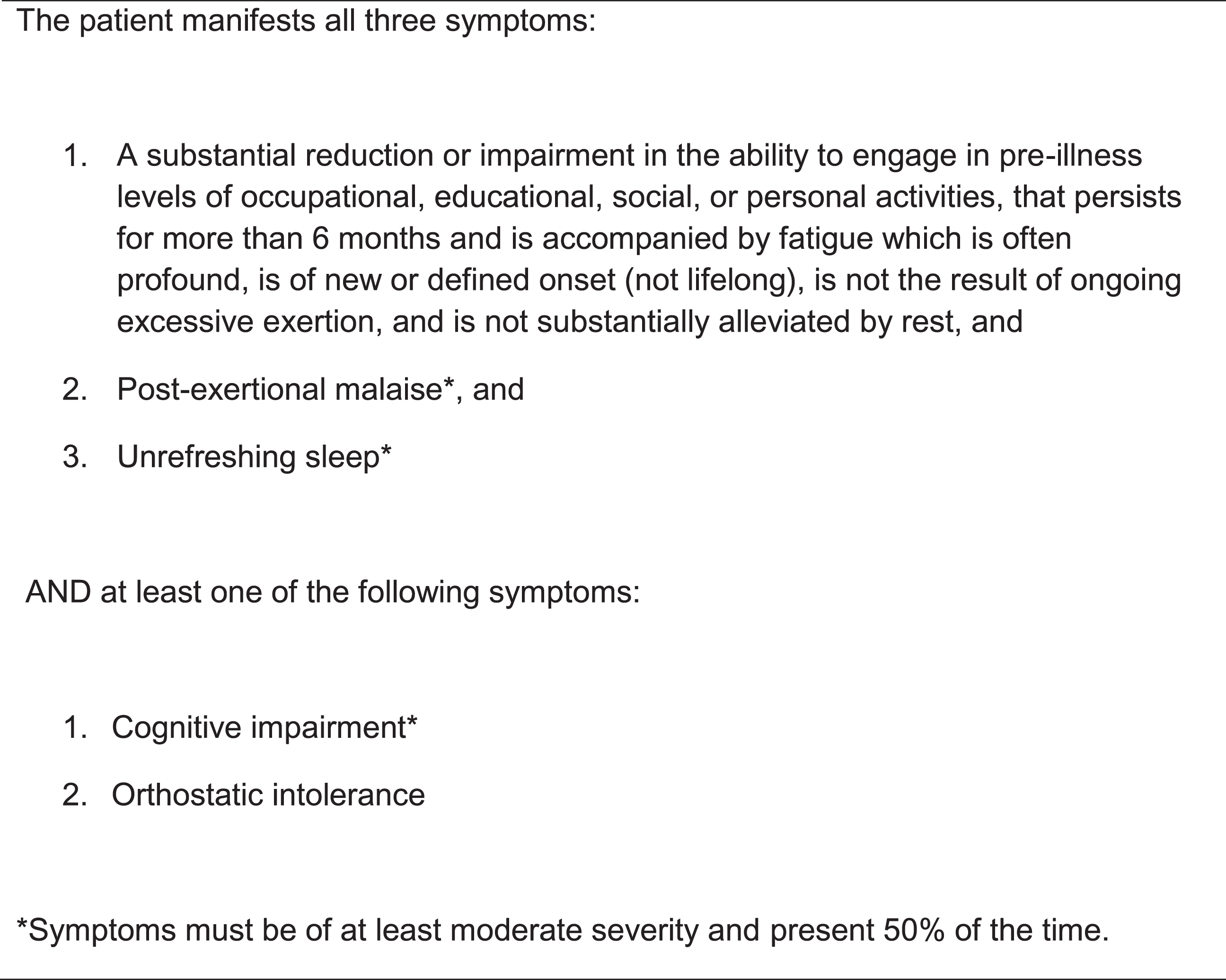
2015 National Academy of Medicine diagnostic criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.
Previous ME/CFS definitions, like the 1994 Fukuda CFS criteria, emphasized chronic fatigue [26]. Although patients do suffer from severe exhaustion, it is not the only symptom nor is it always the most disabling one. Chronic fatigue is also ubiquitous among sleep-deprived, overextended but healthy university students and students affected by other conditions so focusing primarily on fatigue will not help healthcare professionals distinguish this illness. Instead, assessing for and identifying PEM, unrefreshing sleep, cognitive issues, and orthostatic intolerance will increase the likelihood of a timely, accurate diagnosis. Currently, diagnosis of ME/CFS relies on a careful history and physical examination [27]. There is no singular test to diagnose ME/CFS although certain tests can be used to confirm the diagnosis and eliminate other similarly presenting conditions such as anemia [28–30].
A typical story is that of a student who comes down with infectious mononucleosis or a non-specific infection and then fails to recover over subsequent weeks and months. Others become sick after a stressful life event, vaccination, or recent travel [31]. In some cases, no specific inciting event can be identified but the student clearly remembers a time when he/she was physically well and then became sick.
Students will often complain of severe exhaustion, problems thinking, and sleep disturbances impacting their ability to attend school, work, socialize, exercise, and even take care of themselves. These symptoms may occur at rest but are also exacerbated by mental and physical activity as part of PEM. However, typically, students will not recognize and mention PEM unless explicitly asked. Keeping a diary of symptoms and activities for 1–2 weeks can help the student and OT recognize PEM [27].
PEM can begin immediately or several hours or days after an activity; the intensity and duration of symptoms is often out of proportion to the precipitating activity [32, 33]. For example, in more severely affected patients, walking to the end of a driveway to pick up mail or reading a book chapter may lead to being bedbound for hours to days and possibly weeks or months. For less severely affected people (who are more likely to pursue a college education), more strenuous activity like studying for examinations, walking across campus, waiting in line, or shopping for groceries may be required to trigger PEM, but the outcome –worsened symptoms and reduced function –is the same. Once initiated, PEM can last for hours, days, weeks, and even months. The diversity of symptoms, low-intensity triggers, and delayed/prolonged nature of PEM adds to the unpredictability of patients’ lives.
Almost all patients experience significant sleep disturbances such as problems falling and/or staying asleep, feeling more energetic at night, and/or waking up earlier than they wished. Conversely, some patients sleep many more hours than they desire. Regardless of the sleep issue, the most commonly reported symptom is a level of tiredness equivalent to not having slept at all, a phenomenon called unrefreshing sleep.
Orthostatic intolerance (OI), a frequent symptom, refers to increased exhaustion, problems thinking, nausea, light-headedness, and skipped heart beats while the patient is in an upright position, which is reduced or resolved in a supine position. ME/CFS patients with severe OI will readily report these symptoms; however, OI can also present more subtly. Thus, it is important to ask students if they feel worse when standing or sitting for longer periods (e.g., waiting in line, attending lectures) or in hot settings (e.g., during the summer, while showering) [27, 34].
Decreased information processing speed and cognitive fatigue form the basis of cognitive impairment, which manifests as decreased reaction time, concentration, and memory [35]. Multi-tasking, distracting surroundings, upright positions, and sustained cognitive activity aggravate these deficits [36, 37]. In contrast, global intelligence, vocabulary, and reasoning are not affected [35]. When patients are given adequate time and rest breaks, their cognitive performance can equal that of healthy peers [8].
Other symptoms that patients may experience include flu-like feelings, sore throats, tender lymph nodes, headaches, multi-joint non-inflammatory pain, muscle pain, gastrointestinal upset, and hypersensitivity to stimuli (e.g., sound, light, foods, smells). For some patients, these symptoms rise to the level of a comorbid diagnosis. Fibromyalgia, irritable bowel syndrome, and migraine headaches are common [31].
Despite multiple symptoms, comorbidities, and a substantial reduction in cognitive and physical function, students may still appear healthy to the casual observer. This is a trait shared by many “invisible illnesses” like depression, systemic lupus erythematosus, asthma, and multiple sclerosis, where disability is not signaled by an observable feature like an unusual gait or a hearing aid [38]. This invisibility, coupled with the fluctuating health status and function common to many chronic illnesses, regularly results in university faculty and staff doubting the veracity of students’ concerns [39]. Out of concern for reducing the social, personal, and societal costs of being ill, many people with chronic illnesses also try to conceal their illness and appear like healthy peers, which may compound the lack of understanding and empathy toward them [8].
Pathophysiology
For many decades, ME/CFS was erroneously believed to be a phobia of exercise/activity and/or primarily the result of deconditioning [40, 41]. These ideas are now being overturned. Although the exact cause of ME/CFS is still unknown, numerous, consistent abnormalities have been found in the neurological, immune, endocrine, cardiopulmonary, and metabolic systems of patients. Patients’ bodies are unable to produce energy aerobically in the same way healthy or even other sick people can. During two cardiopulmonary exercise tests (CPET) separated by 24 hours, both healthy, sedentary study participants and participants with other diseases like multiple sclerosis were able to reproduce cardiometabolic parameters. In contrast, parameters such as work generated at ventilatory threshold dropped significantly on the second cardiopulmonary test for people with ME/CFS [42, 43]. Aerobic metabolism supports continuous or repetitive activities, which may explain why patients can engage in some activities rarely or intermittently, but not regularly or for longer periods. These abnormalities may underlie PEM. A dysfunctional autonomic nervous system that reverses the balance of sympathetic and parasympathetic effects nocturnally is associated with unrefreshing sleep [44]. For the same cognitive task, patients need to recruit more and different areas of the brain compared to healthy volunteers [45]. Higher levels of lactate, associated with non-aerobic metabolism, have also been discovered in the cerebrospinal fluid of people with ME/CFS [46]. For a complete discussion of these and other findings, see the 2015 National Academy of Medicine report, Rutherford et al., and Komaroff [10, 48].
Implications for occupational therapists
In their practices, OTs may be referred patients under three scenarios: a) with another diagnosis, like “chronic fatigue” or “deconditioning”; b) with a diagnosis of ME/CFS and prescription for “graded exercise therapy” (GET) or similar words, and c) with a diagnosis of ME/CFS and no specific treatment plan.
In the first scenario, OTs may find that patients do not respond or respond with worsened health to any efforts to increase their activity levels. This worsening is emblematic of PEM. In these cases, the OT will want to test if the patient fits the aforementioned National Academy of Medicine criteria and, if so, discuss with the referring provider a possible diagnosis of ME/CFS [27]. Recall that many medical providers have not been educated about ME/CFS.
In the second scenario, although GET has been the standard of care for decades, accumulating scientific evidence, clinician/patient surveys, and re-analyses of past trials have demonstrated that GET is not only ineffective but may be harmful, due to increasing episodes of PEM. Re-analyses of GET trials like PACE using the original rather than post-trial, modified protocols have shown that the percentage of patients recovering with GET (4%) is not substantially different from those receiving usual care (3%) [49]. Referring healthcare providers may not realize that 50% of thousands of patients, surveyed across countries and years, report that GET worsened their health [50, 51]. Thus, entities like the US Centers for Disease Control and Prevention and Northern California Kaiser Permanente are withdrawing GET as a treatment for ME/CFS [52, 53].
In place of GET, experienced clinicians and patients prefer “pacing,” which employs techniques similar to energy conservation and activity management and is a practice OTs are qualified to oversee. As with other medical conditions, OTs will collaborate with patients to identify obstacles and incorporate behavioral techniques (e.g., planning, prioritization, delegation of activities), assistive devices (e.g., shower chairs, canes), and environmental modifications to overcome loss of function. One major difference is that in “pacing” there is no assumption that a patient will escalate their activity levels. Patients may hit a physiological ceiling and remain at that level for years or decades and yet may still improve their function and quality of life [54]. For ME/CFS-specific, OT-informed resources aimed at all patients, see www.cfsselfhelp.org and the two-part series by Taylor et al. [55–57].
We will concentrate on environmental modifications in this paper. Students may be required by their universities to obtain documentation of medical need for accommodations. Oftentimes, physicians lack the training or time to document these needs. If the OT can recommend accommodations backed by clear medical reasoning, their notes may be directly cited or used by physicians. Although directed at children rather than at university students, Newton et al.’s and Rowe et al.’s papers contain some points to consider in documentation and sample physician letters [30, 58]. Additionally, university faculty and staff are more likely to listen to the suggestions of a healthcare professional than a student or a parent.
There are currently no established, effective disease-modifying treatments for ME/CFS. Existing treatment focuses on managing individual symptoms. The physician or primary medical care provider should be working with the patient simultaneously to educate them about ME/CFS, palliate symptoms such as pain and sleep, and discern and treat co-morbidities. The OT should check that these factors are being addressed as they work in synergy with the OT’s own efforts. Despite optimal medical care, only 5% of patients recover although 40% can experience some degree of improvement [59]. OTs can help patients maximize their function and quality of life even while they remain sick. As university students straddle the divide between pediatric and adult medicine, two excellent, comprehensive references for medical providers are the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis 2014 Primer for Clinical Practitioners and Rowe et al.’s review covering pediatric ME/CFS [29, 30]. OTs may also refer providers to the five-page guide prepared by the US ME/CFS Clinician Coalition [28].
Recommended accommodations
The following recommendations include many accommodations that faculty or university administrators will have to approve or implement. However, OTs can ensure that students are aware of potential accommodations and suggest to students that they negotiate with faculty and administrators to obtain access to them. OTs can use this information when, for example, assessing student functioning in academic settings, and can adapt these recommendations when writing a letter on behalf of a student to explain his/her condition and recommended accommodations. We have also summarized information about ME/CFS and these actionable steps in four infographics (“Who is affected,” “Common ME/CFS symptoms,” “Academic accommodations,” and “Students: Seek help early and often”) that can be accessed online (https://tinyurl.com/mecfsuniversity) and shared with students and universities.
Maintain overall awareness of the fluctuating nature of ME/CFS
(A) Maintain awareness of the waxing and waning nature of ME/CFS and its unpredictability.
Someone with ME/CFS can possess a lot of energy one day and very little the next. PEM can also cause a change in the student’s condition on shorter timescales, e.g., minutes to hours. Emergencies can arise (e.g., hospitalizations, sudden worsening, relapses) which can place a student out of commission for longer periods of time. Thus, the student should be given as much flexibility as possible to design ways to meet his/her academic obligations in the context of academic course and degree requirements. Students should also be allowed to defer accommodations in circumstances where they feel adaptations would have little benefit. Students should designate someone to call who can take over notifying the appropriate professors or other personnel in the event of an emergency.
Advise students to negotiate accommodations in advance
(B) Ensure that affected students are aware of the need to register with the disability office as early as possible.
Up to 50% of students with a disability do not see themselves as disabled because they equate disability with more traditional issues such as vision or mobility problems and 40% thus do not register with their school’s disability office [39]. Disability services can inform students as to what types of accommodations are possible and the process needed to obtain specific accommodations. When working with students prior to college, OTs should advise them to communicate with disability services offices before they apply to or enter a university in order to learn about the services provided and to share information about their anticipated needs. Once enrolled, students should also check in with the student health center regarding their diagnosis and treatment. Center staff may not be familiar with ME/CFS and the OT, as well as the student’s own physician, may need to be involved in briefing them.
(C) Advise students to schedule an appointment with an academic adviser/consultant early in their university years.
Once students have an inkling of what interests, degrees, and/or careers they wish to pursue, they should discuss their goals with an adviser. In some cases, a chosen plan of study or career may not be suitable given the student’s health. Conversely, a flexible schedule (e.g., extended time to finish coursework or obtain degree, ability to avoid taking demanding classes and required internships in the same term and instead spread them out, designating a full course load as nine rather than twelve credits) could be constructed that preserves the student’s health while satisfying degree requirements. Early planning can improve a student’s higher education experience and decrease disappointment, wasted time/effort/money, as well as the number of uncompleted courses.
(D) Encourage students to communicate with instructors prior to beginning a class.
Students can use websites like Rate Your Professor, browse course outlines, and talk to fellow students to get an idea of the way a class is handled and the likelihood that the professor will work with the student. If students have registered with their school’s disability office, some offices will inform a student’s professors automatically. However, to ensure their professors are aware and fully informed of the student’s individual needs and in order to establish a direct relationship, students should initiate a conversation.
(E) Encourage students to request assignment flexibility when possible, emphasizing mastery over quantity of work.
(F) Help students to minimize travel.
Students may want to request: Support for participation from off-campus sites, e.g., home or hospital Provision of teleconference capabilities Online courses and/or placement of class materials online Housing close to campus A dorm room that is private, handicap-accessible, and/or close to shared amenities A handicapped parking permit Transportation to and between classes
Requests directed to disability and other university offices
(G) Request lecture notes and/or recordings when lectures are not online or otherwise available for review. If no recordings are available, allow students to record lectures on their own.
(H) Request examination accommodations ahead of time. Some examples of test accommodation are: Additional time Scheduled and/or spontaneous rest breaks Allowance of food and drink (provided by the student) as needed to effectively manage their condition Alternative testing modalities (e.g., online, oral, etc.) Scheduling exams so students can take advantage of their higher energy times Spacing out examinations (e.g., allowing two two-hour final tests to be taken on separate days rather than the same day) A quiet place to take exams, e.g., the disability office or the use of ear plugs, noise-cancelling headphones
(I) Request flexible scheduling when possible and the ability to miss or leave classes without penalty when medically necessary.
(J) Request easily accessible rest areas on campus and the right to take opportunities for rest where and when needed.
(K) Request ergonomic furniture and devices, such as desks, chairs, computers, keyboards, computer mice, etc.
(L) Request as much flexibility as allowable for students who have a work assignment, such as a teaching assistantship, or another type of work-like experience, such as an experiential learning course requirement. Examples of accommodations include: Teaching remotely Scheduling class at a convenient time Facilitating remote office hours
(M) Facilitate the use of wheelchairs, mobility aids, and other power-driven mobility devices (OPDMDs), as provided for in the Americans with Disabilities Act, where legal and consistent with applicable university policies.
Ask students if elevators and automatic doors are functioning properly, ramps are properly placed and clear of hazards, and sufficient handicapped parking is distributed throughout the campus. Ask if free, convenient and handicapped-accessible, campus transportation is available. If these are not available or not functioning properly, report these details in writing to the university so they may address obstacles/potential hazards in the physical environment on campus.
Advocating for students at a systemic level
The next three accommodations are not under the direct purview of OTs. However, if asked, OTs can bring up systemic changes that universities can implement to improve the situation campus-wide for all students with ME/CFS and even students with other chronic illnesses. OTs can also offer to be a resource for the university.
(N) Provide awareness training to relevant university staff. Educate faculty and staff about non-traditional disabilities, e.g., share this document and the associated infographics with staff Prepare orienting information for faculty and student-facing staff who encounter students with ME/CFS Educate campus-based medical providers, psychologists and counselors about the physiological basis of ME/CFS so that inappropriate suggestions for more activity or psychological treatment are not offered. Students may develop co-morbid depression or anxiety due to the challenges of living with a chronic, disabling illness, but mood disorders are not an inherent part of ME/CFS. This information could be included along with information on chronic illness in general
(O) Arrange for support services, ideally: An adviser trained to advocate for students with ME/CFS A guide directed at students with ME/CFS that teaches them self-advocacy, their rights on campus, what accommodations are available, what to ask for and how to ask for them A pamphlet for faculty that the student could provide at the beginning of the term Opportunities for interaction with other students. For example, students who self-identify as having ME/CFS or who are affected by other diseases but face similar struggles may desire to meet each other in person or online Counseling staff who are aware of the needs of students with ME/CFS Health center staff who are familiar with ME/CFS
(P) Ensure that the various university offices that serve students with ME/CFS are working synchronously and in harmony with each other.
For example, students should check with their adviser to ascertain if their financial aid (whether originating from governmental, private, or other resources) is conditional on a particular course load, considering that students with ME/CFS could function much better by lightening the load and taking longer to finish their degrees. Advisers may be able to help the student negotiate such issues.
Conclusion
Given the growing prevalence of chronic illnesses and the specific demands they impose on the sufferers in the context of higher education, leaders of colleges and universities will need to develop a new paradigm which considers the issue from multiple perspectives (objective, subjective, cultural, and systemic) and that offers students chronic-illness-specific accommodations. Along with the aforementioned accommodations, the academic experience of students with ME/CFS and other students with chronic illnesses would improve with compassionate understanding, community acceptance, and a recognized place within the larger university system. This shift would necessitate a multi-faceted, systemic effort of removing environmental barriers in higher education that have been demonstrated to impede academic success.
OTs who understand the realities of their patients’ college and university lives can make a strong, lasting contribution to this positive change by being aware of the many possible support options for students with ME/CFS and recommending them as appropriate. They are also in a unique position to share their up-to-date medical knowledge and their position of professional authority to advocate on behalf of students with severe, chronic illnesses like ME/CFS.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We would like to thank the numerous students and families who shared with us the struggles they encountered and the accommodations they found helpful in obtaining a university education. They have enabled us to be much more specific and detailed in our suggestions.