
Abstract
BACKGROUND:
Psychosocial work factors and general recovery experiences are hypothesised to influence the risk of low back pain (LBP) occurrence by influencing the acute recovery-stress state. So far, however, direct links between the acute recovery-stress state and LBP occurrence have not been investigated in detail.
OBJECTIVE:
The aim of this study was to investigate differences in low back pain occurrence between four distinct recovery-stress groups over a period of 6 month.
METHODS:
A prospective cohort study with a 3-month and 6-month follow-up measurement was conducted in a sample of administrative employees (N = 271). First, the sample was divided into four distinct recovery-stress groups by cluster analysis. Subsequently, differences in LBP occurrence between these four groups and the Relative Risk (RR) were analysed.
RESULTS:
Overall, groups with higher stress than recovery scores showed a higher risk of LBP occurrence compared to those groups with lower stress than recovery scores. Furthermore, the group with the highest stress and lowest recovery scores showed a significant higher proportion of LBP occurrence after six months than the group with the lowest stress and highest recovery scores (RR = 7.29).
CONCLUSION:
The results indicate the relevance of the acute recovery-stress state for LBP occurrence.
Introduction
In recent years, psychosocial stressors and resources have been identified as relevant risk factors for low back pain (LBP) occurrence [1, 2]. Research in this field has focused on work-related factors such as social support at work or work demands, although it seems as if high leisure time stressors and low resources also raise the risk of LBP [3, 4]. There is evidence that these risk factors increase the risk of LBP occurrence by influencing stress experience and associated physical load reactions; for example, through alterations in muscle activity or hormonal and inflammatory responses [5–7].
Whereas the examination of general risk factors related to LBP might be a useful approach to identify key aspects especially for occupational health management and global prevention programmes this approach has one major drawback; it overlooks the fact that influences of these risk factors strongly depends on recovery processes, experiences, and the recovery state [8–10].
Work-health models emphasised the moderating influence of recovery processes on the influence of work factors on general health [11, 12] and LBP occurrence in detail [13]. According to these models, recovery processes buffer the negative effects of stressors on health in two distinct ways: a well-recovered person perceives work stressors as less demanding and the physical load reactions are thus less strong; and recovery processes are necessary to stop the physical load reactions after confrontation with a stressor and return the physical system into the initial state. Persons with a high need for recovery showed an increase in health issues and more sickness absence [14–16]; moreover, an association with musculoskeletal complaints was also reported [17]. Similarly, employees with insufficient possibilities to recover during leisure time showed a decrease health status [11, 18] and had even an elevated risk of cardiovascular death [19]. Furthermore, neuroendocrine markers of the acute recovery-stress state – such as cortisol or adrenaline – have been associated with the occurrence of health complaints [20, 21].
Only few studies have investigated the association between of recovery and psychosocial risk factors with musculoskeletal diseases in further detail. Mierswa and Kellmann [22] identified a moderating effect for the recovery experience detachment, a process of physically and psychologically distancing from work stressors, on the influence of psychosocial work factors on LBP occurrence. These results are in line with theoretical assumptions as detachment reduced harmful influences of work stressors on the back and promoted protective effects of high work resources. Gawke, Gorgievski, and van der Linden [23], reported a partly mediation effect of need for recovery on the relation between work demands and musculoskeletal complaints. This result supports the assumption of work demands to being harmful by depleting resources and adequate recovery after work might be helpful to prevent health complaints. The acute stress and recovery state is thus associated with the occurrence of musculoskeletal complaints and seems to have a more direct link to LBP than general psychosocial risk factors. Investigating the influence of the acute stress and recovery state on the chance of developing LBP in long-term could lead to further insight in the processes that are relevant to decrease the risk of work related health complaints.
According to the concept of Kallus [24], recovery is not only the absence of stress but also a process of refilling or expanding personal resources; for example, strength, will, or energy. Given that both states – being stressed and being recovered – are not two extremes on one scale, but are rather individual, it is important to take into account both – the recovery and the stress states as well as possible interrelations between them [25].
Kellmann and Kallus [26] propose a division of study samples into four distinct recovery-stress groups (RSG) depending on their recovery-stress state: low recovery – high stress, low recovery – low stress, high recovery – high stress, and high recovery – low stress. This differentiation into distinct RSG takes into account the non-linear interaction between the recovery and stress state. Gathering more information about the immediate influence of the acute recovery-stress state on the LBP risk might help to identify people at an acute high risk of LBP development, individualise prevention programs, and design the programs in a more demand-oriented manner.
The aim of this study was thus to investigate differences between the mentioned RSG with respect to LBP occurrence. It can be hypothesised that people at a high stress state and a low recovery state have an increased risk of LBP, whereas those at a higher recovery and low stress state should have a reduced risk. Furthermore, a higher recovery state is presumed to reduce the LBP risk between groups with comparable stress states.
Method
Participants
All participants of the initial study sample (N = 821) worked as administration employees of 13 German universities from North Rhine-Westphalia. A more detailed description of this study sample can be found in Mierswa and Kellmann [22]. In the present analysis, only those participants with no LBP at the baseline measurement (N = 271; 32%) were included to investigate the influence of their recovery-stress state on future LBP occurrence. Further exclusion criteria were being aged under 18 years (zero participants excluded) and less than half-time employment (nine participants excluded). Finally, 262 participants (74% women; M Age = 42.97, SD Age = 11.37) were included in the analyses.
Procedure
The researchers sent study information via e-mail to the staff councils of all universities in North Rhine-Westphalia and asked for their support in the study. Those staff councils providing permission to consult the employees of their university received another e-mail including a link for an online survey and basic study information. The staff councils forwarded this e-mail – including the link – to the administration employees at their universities for the baseline measurement (T0). Possible recipients were all employees in the offices of the central administration, the department administration as well as those of additional facilities; for example, libraries or university sports. After three (T1) and six months (T2), another link was sent to the staff councils and forwarded to the employees for follow-up measurements. The online survey was compiled by using the online software SoSciSurvey and it comprised four parts: first, further study information and the informed consent; subsequently, one page generating an individual code for pseudonymisation; followed by the questionnaires as described in the following section; and finally, a closing screen with the author’s contact information. The follow-up measurements were identical to the baseline, aside from questions regarding socio-demographic facts which were excluded to reduce survey length andduration.
Materials
First, the socio-demographic facts age and gender as well as basic work related information (working hours per week, overtime per week in the previous three months, proportion of computer work indicated in percentage) were examined. Subsequently, parts of the Nordic Musculoskeletal Questionnaire [27] were used to indicate the existence of musculoskeletal complaints. Participants had to answer the question “Have you at any time during the last three months had trouble (such as ache, pain, discomfort, numbness) in” for nine body regions (neck/shoulder/elbows/wrists or hands/upper back/lower back/hips or thighs or buttocks/knees/ankles or feet) with yes or no. All pain regions were indicated on a drawing of the human body to avoid faulty allocations of the body regions. The time span of the questions was adapted to the follow-up rhythm of three months, as already conducted in previous studies [5, 29]. The assignment of participants into a non-LBP and LBP group was based upon their answer regarding trouble in the lower back, whereby those who indicated yes were assigned to the LBP group.
Furthermore, those participants who indicated suffering from LBP were asked to answer the Chronic Pain Grade Scale (CGPS;30) in the third section to receive detailed information about their average pain intensity, highest pain intensity, and the perceived disability caused by LBP in work, social and family activities, as well as everyday activities. In addition, participants had to specify the number of days they had been unable to follow their usual activities due to back pain in the previous three months. Overall Pain Intensity (α= 0.93), Overall Disability (α= 0.74), and Chronification Grade were computed according to descriptions of von Korff, Ormel, Keefe, and Dworkin [31].
Finally, participants were asked to complete the Recovery-Stress Questionnaire (RESTQ), measuring the current recovery-stress state by gathering the frequency of certain activities related to current recovery or stress experiences [32]. Participants indicated how often they had been involved in stressful or recovering activities in the past three days and nights on a Likert scale ranging from 0 (never) to 6 (always). Overall, the RESTQ comprises 48 items measuring the recovery state on five distinct scales (Success, Social Recovery, Physical Recovery, General Well-being, Sleep Quality) and the stress state on seven scales (General Stress, Emotional Stress, Social Stress, Conflicts/Pressure, Fatigue, Lack of Energy, Physical Complaints). High scores on the stress scales/dimension indicate a high stress state, whereas high scores on recovery scales/dimension imply that the participant felt well recovered. The internal consistency of all scales in the final sample (N = 262) reached a sufficient value (Cronbach’s α ≥ 0.70), aside from the scale Conflicts/Pressure (Cronbach’s α = 0.63). These lower values for the internal consistency of the Conflicts/Pressure scale have also been reported in previous studies. The Conbach’s α values of the Overall Recovery and Overall Stress dimension were above 0.80 in the present studysample.
Data analysis
First, occurrence and strength of LBP at T1 and T2 was descriptively analysed. Afterwards, recovery-stress groups (RSG) were formed based upon the twelve RESTQ scales. According to the concept of Kellmann and Kallus [26], four groups of recovery-stress states could be formed by dividing the Overall Stress and Overall Recovery scores with median-split and then combining the two stress groups (low/high) with the two recovery groups (low/high). As the median-split method has been subject to methodological discussion in scientific research [33, 34] a 4-means cluster analysis with the twelve scales of the RESTQ and an iteration-maximum of 20 was conducted to form the four RSG.
A 4-group solution was chosen based upon the theoretical assumptions and previously formed groups, as described by Kellmann and Kallus [26]. The RSG were compared regarding age, gender, working hours, overtime, and RESTQ scores, by using either parametric or non-parametric group comparisons with post-hoc analyses, including Bonferroni-correction.
Differences in LBP occurrence at T1 and T2 between the RSG were identified by use of the Chi-Square test with the RSG as independent and LBP occurrence as dependent variable. Subsequently, single-group comparisons with Bonferroni-correction were examined to specify the differences between the individual RSG. Furthermore, the Relative Risk (RR) of developing LBP was analysed for all combinations of the four RSG to analyse the predictive power of the RSG on LBP occurrence. RR analysis was given preference over a regression approach because regressions tend to overestimate the effect size when the outcome variable is quite common [35]. Standard errors and 95% confidence intervals for the RR were calculated according to the work of Altman [36].
Results
The number of participants who completed the online survey dropped from 262 at T0 to 113 (43%) at T1 and further down to 76 (29%) at T2. At T1, 30 (27%) of the 113 participants and 26 (34%) of the 76 participants at T2 indicated a phase of LBP in the previous three months. Socio-demographic details of the participants and LBP-incident numbers for all three measurement points are presented in Table 1.
Of those who reported LBP at T1, 27% (n = 8) also reported a phase of LBP at T2. Pain intensity and disability of all participants with LBP at T1 or T2, as well as the Chronification Grade as classified by von Korff et al. [31] are summarised in Table 2. Most of the participants with LBP only reported low to medium pain intensity and disability scores. Consequently, about 80% of them were classified as Chronification Grade 1 and only six participants at T1 and four at T2 as Chronification Grade 2 or 3, no one was classified as Grade 4.
Characteristics and Number of Low Back Pain (LBP) Cases in the Study Sample at Baseline (T0), 3-Month (T1), and 6-Month (T2) Follow-Up Measurement
Characteristics and Number of Low Back Pain (LBP) Cases in the Study Sample at Baseline (T0), 3-Month (T1), and 6-Month (T2) Follow-Up Measurement
Pain Parameters at 3-Month (T1) and 6-Month (T2) Follow-Up Measurement
Note. LBP = low back pain.
The 4-means cluster analyses (15 iterations) led to four distinct RSG, as summarised in Fig. 1. The first group (RSG-1; n = 28; 11%) revealed high scores (> 3) on all stress scales and low scores on all recovery scales. The second group (RSG-2; n = 56; 21%) was characterised by stress scales at a medium level (2 –3) and low recovery scores, comparable to those of RSG-1. The third group (RSG-3; n = 75; 29%) showed low stress values (< 2) and medium recovery scores (2 –4). Most participants (n = 103; 39%) were assigned to the last group (RSG-4), with four out of seven stress scales lower than ‘1’ and high recovery scores (> 3). There was thus a decrease of the stress scores and an increase of the recovery scores from RSG-1 to RSG-4.
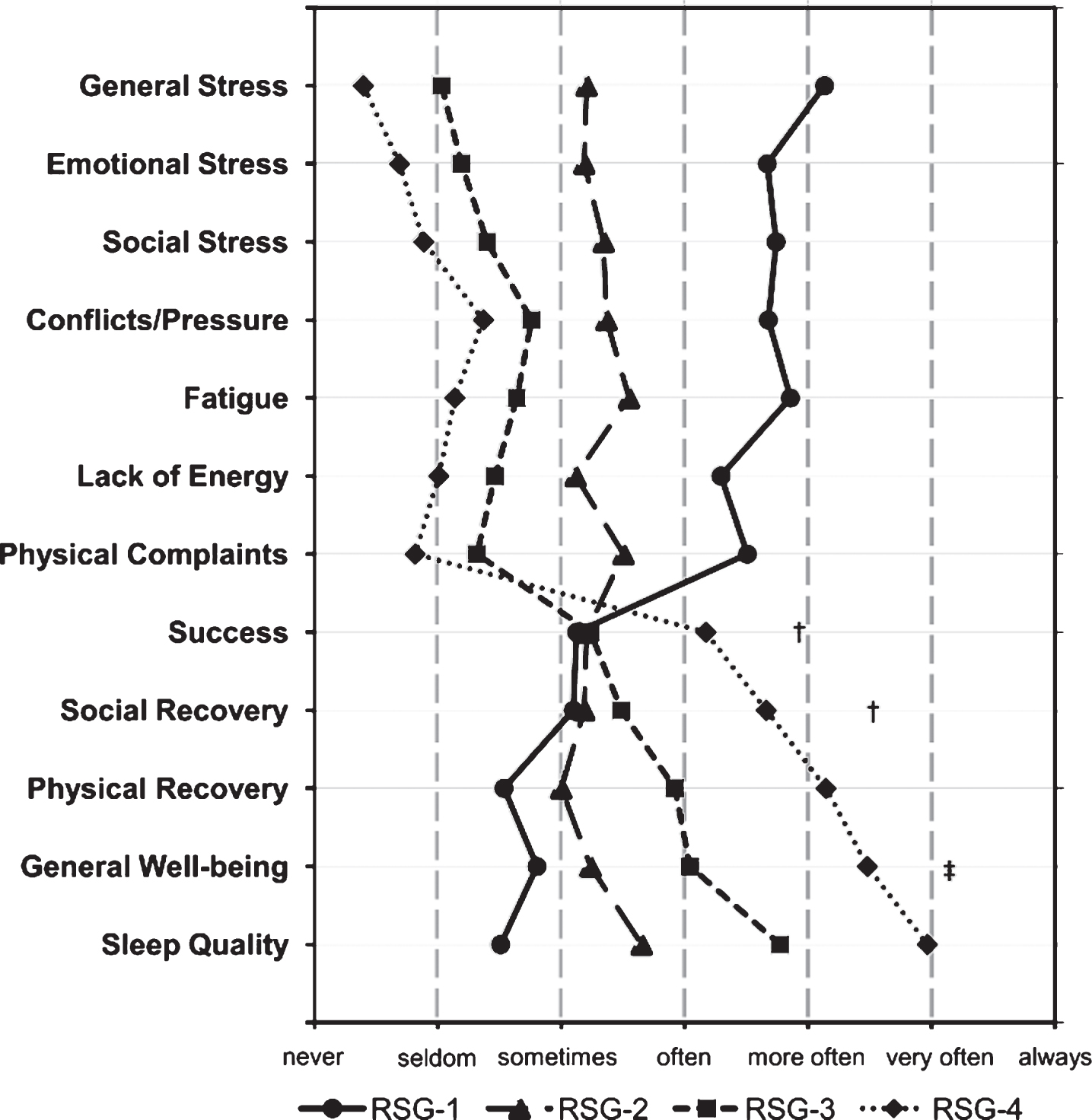
The profiles of the four Recovery-Stress Groups (RSG) formed by cluster analysis of the Recovery-Stress Questionnaire scales, N = 263. All groups differed significantly on each scale (p < 0.01), if not indicated otherwise. † No significant differences between the groups RSG-1, RSG-2, and RSG-3. ‡No significant differences between the groups RSG-1 and RSG-2.
Group comparisons between the four RSG revealed no significant differences in age, gender, computer work, and working hours at the baseline measurement, but a significant difference in overtime per week (χ2 = 10.45, df = 3, p < 0.05). RSG-1 (M = 4.43, SD = 6.09) showed more overtime per week compared to RSG-4 (M = 2.28, SD = 4.84). Furthermore, the RSG significantly differ (p < 0.01) on nearly all RESTQ scales, as could be expected due to the chosen cluster method. However, on the Success and Social Recovery scales, only RSG-4 showed significantly higher scores than the other RSG. Moreover, the two groups – RSG-1 and RSG-2 – did not significantly differ on the General Well-being scale, as indicated in Fig. 1.
Regarding possible differences in LBP occurrence between the four RSG, the χ2-test showed a trend for the 3-month follow-up (χ2 = 6.46, df = 3, p < 0.10, V = 0.24) and significant effects at the 6-month follow-up (χ2 = 7.89, df = 3, p < 0.05, V = 0.32). No effects were found for single-group comparisons at T1, while at T2 a significant difference in LBP occurrence was identified between the two extreme groups, RSG-1 and RSG-4 (χ2 = 7.45, df = 1, p < 0.05, V = 0.42).
The distribution of participants with and without LBP in the RSG for T1 and T2 are presented in Fig. 2a and b, respectively. At T1, the proportion of participants with LBP was highest in RSG-1 (47%) and lowest in RSG-3 (17%). At T2, an almost linear decrease of LBP occurence was found, declining from 64% for RSG-1, over 46% (RSG-2), to 35% (RSG-3) and 19% in RSG-4.
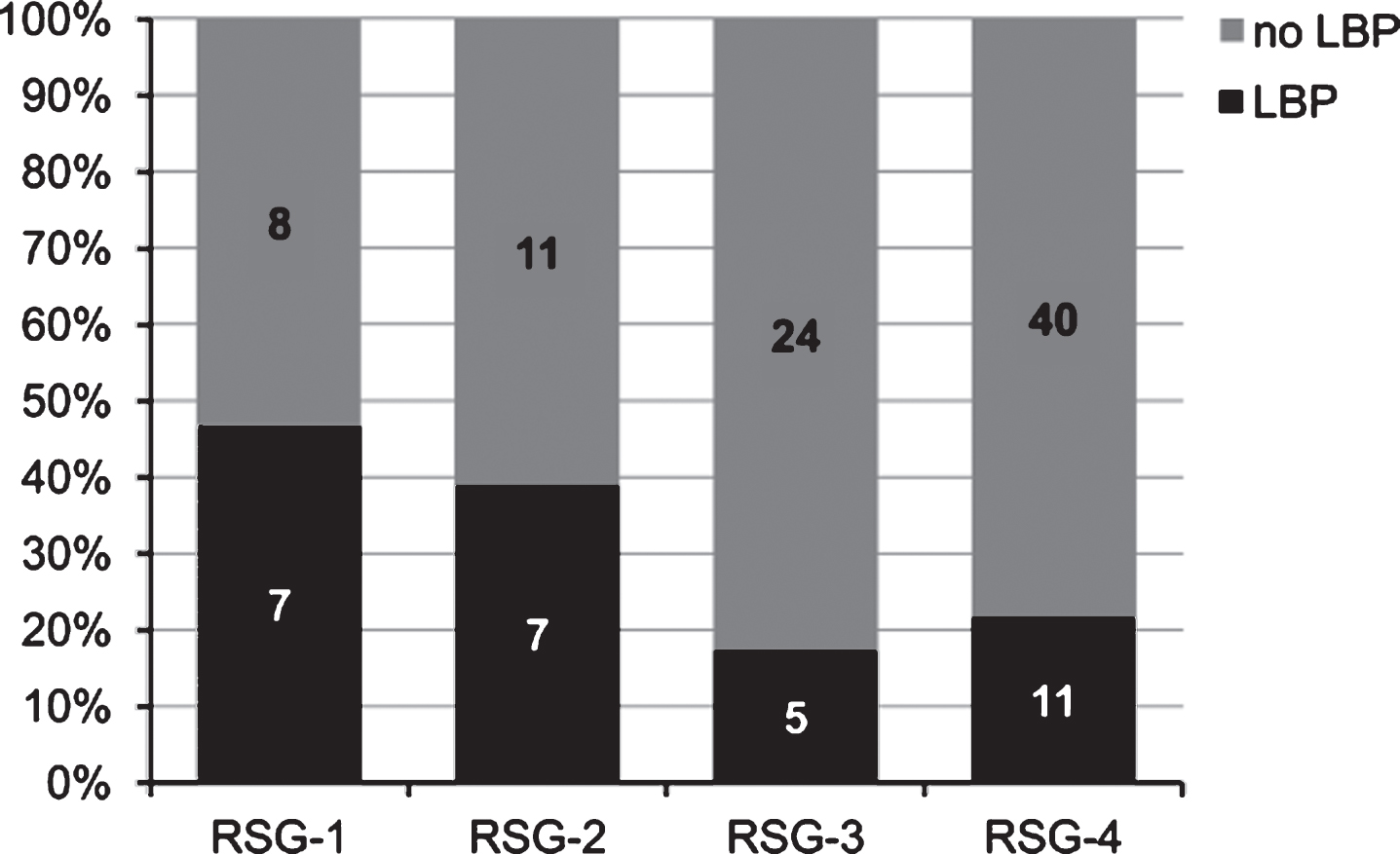
Distribution of employees with and without low back pain (LBP) in the four Recovery-Stress Groups (RSG) at 3-month follow-up (T1), N = 113.
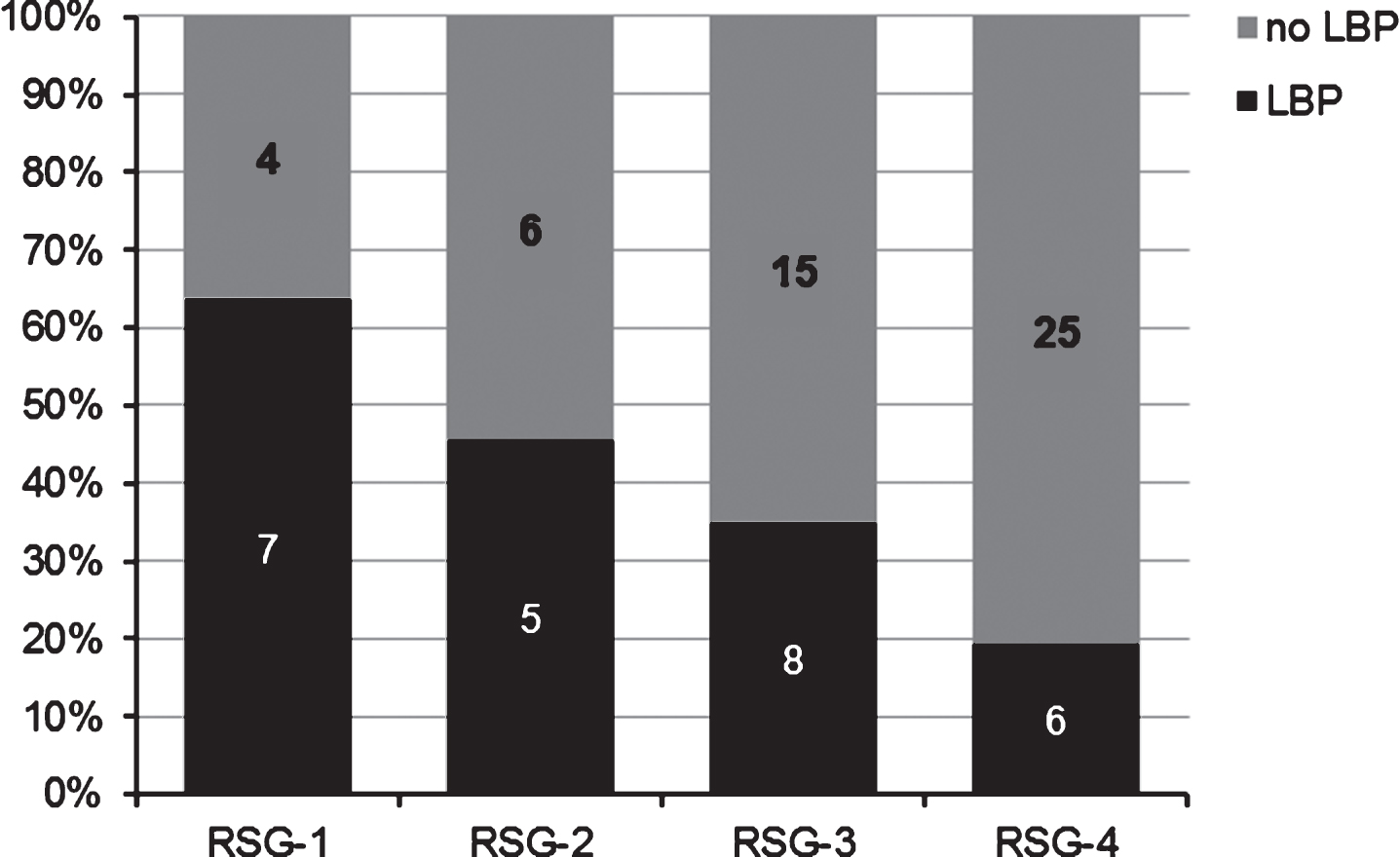
Distribution of employees with and without low back pain (LBP) in the four Recovery-Stress Groups (RSG) at 6-month follow-up (T2), N = 76.
As shown in Table 3, the RR to report LBP at T1 was found to be approximately three times higher for the two groups with low recovery values (RSG-1, RSG-2) compared to the two other groups with lower stress and higher recovery values (RSG-3, RSG-4). Furthermore, no increase in LBP risk was found for the comparison of RSG-2 with RSG-1 – both defined by unfavourable stress and recovery values – and the comparison of RSG-3 with RSG-4. At T2, an increase in the LBP risk can be observed from RSG-4 to RSG-1, whereby the latter had a more than seven times higher risk of reporting LBP compared to RSG-4 and a three times higher risk compared to the participants in RSG-3 (Table 4). Comparisons of adjacent groups led to only small relative risks of developing LBP, ranging from 1.31 (RSG-2 vs. RSG-3) to 1.80 (RSG-3 vs RSG-4).
The Relative Risk of Low Back Pain Occurrence between the Four Recovery-Stress Groups (RSG) at 3-Month (T1) Follow-Up Measurement
The Relative Risk of Low Back Pain Occurrence between the Four Recovery-Stress Groups (RSG) at 6-Month (T2) Follow-Up Measurement
Previous studies have revealed an impact of work-related psychosocial stressors and resources on the risk of developing LBP [1, 2]. The experience of stress –induced by the interplay of work stressors and resources – was presumed to play an essential role in the process of LBP development by inducing neuroendocrinological and muscular changes in the body [37]. Recent studies regarding the perception of psychosocial work factors and their influence on the stress state have emphasised the importance of general psychological recovery experiences [10, 39]. In line with these results, Mierswa and Kellmann [22] indicated recovery processes in leisure time to moderate the association of psychosocial risk factors at work with the occurrence of LBP.
Psychosocial work factors and general psychological recovery experiences are thought to have an impact on LBP risk by influencing the individual recovery-stress states. So far, however, no study has investigated the immediate link between the acute stress and recovery state and occurrence of LBP. The main aim of this study was to bridge this gap and investigate differences in LBP occurrence between four stress groups derived from the recovery-stress model of Kallus [24].
The results of this study support the assumption of acute stress and recovery state being relevant for occurrence of LBP. Before discussing the results in further detail, a closer inspection of the formed RSG is provided. Whereas Kellmann und Kallus [26] used median-split method to form four RSG (high stress – low recovery; high stress – high recovery; low stress – low recovery; low stress – high recovery) based upon the Overall Stress and Overall Recovery dimensions, cluster analysis including the twelve recovery and stress scales was used in the present article.
The four RSG formed by cluster analysis correspond with these median-split groups for most parts. The existence of the two extreme groups (high stress – low recovery, low stress – high recovery) was confirmed by the cluster analysis (RSG-1 and RSG-4), although the proportion of all participants belonging to the high stress – low recovery group was lower by use of cluster analysis. The proportion of participants in the group with high recovery and low stress scales was similar for both methods. The RSG-2 is comparable to the low stress – low recovery group, because the stress and recovery scores were all at a low to medium level (‘2’ to ‘3’). The proportion of participants in this group was similar by use of both grouping methods, too. The last group (high stress – high recovery) reported by Kellmann and Kallus [26] could not be confirmed by use of cluster analysis. The last group (RSG-3) built through cluster analyses was defined by low stress scores and recovery scores at a medium level (‘2’ to ‘4’). Given that Kellmann and Kallus [26] did not report the exact threshold values used for the median-split, comparison of the two grouping methods is limited to this more qualitative description. Future studies with larger and more inhomogeneous samples are necessary to test for generality of the reported RSG classification, as only LBP-free administration employees were included in this study. Despite this lack of generality, the results indicate that a two-group solution for the recovery-stress state (being stressed vs. not being stressed or being recovered vs. not being recovered) could lead to an oversimplification because over 50% of the participants belonged to one of the less extreme RSG in between.
The examined differences in LBP occurrence at T2 between the four RSG strongly support the hypothesis that the recovery-stress state is associated with LBP risk. As reported in several previous studies, those employees with a higher need of recovery were at a higher risk of illness [16, 40] and those with good recovery experiences in leisure time, increasing the recovery state, reported LBP less often in a cross-sectional study [22] and showed a decreased influence of work demands on LBP in a longitudinal study [13]. This lower LBP risk was also found for those employees with higher recovery scores (RSG-3, RSG-4) in the present study. Likewise, the higher LBP risk of employees with a high stress state (RSG-1) is in line with the theoretical considerations and previous results [16, 42]. Athletes with a high stress state showed a higher risk of injury and illness in previous studies [43, 44] and employees confronted with high work demands developed LBP more often [1, 45, 46].
At T1, no difference in the LBP occurrence could be identified between RSG-1 and RSG-2, even though the latter had significantly lower stress values. This could mean that either stress has only a minor direct influence on the LBP risk at T1 or a decrease in LBP risk is only seen when the stress values are even smaller than those of RSG-3 or RSG-4. More generally, it should be investigated, whether there is a linear or exponential relation between recovery and stress scores and LBP or if there are possible thresholds after which the LBP risk rapidly increases or decreases. The higher RR at T2 for RSG-1 compared to RSG-2 suggests a dose dependent relation between stress state and LBP risk in the long term. However, it must be kept in mind that the RESTQ scores and thus the RSG distribution could change for the participants over the six months period because the RESTQ timeframe only refers to the past three days and nights. Furthermore, only the comparison of LBP risk between the two extreme groups RSG-1 (high stress – low recovery) and RSG-4 (low stress – high recovery) reached a significant level, although the RR for the other comparisons were quite high, too.
A major limitation of this study is the homogeneity of the study sample and the way how participants had been contacted. Most of the participants were women and the professional activity and the working conditions of administration employees in German universities might differ to those in the free economy. Results of this study could thus not be generalised and have to replicated in future studies. Furthermore participants were recruited by email and no information were available about those employees not participating in the study. It might be that especially those employees experiencing very high stress were not able to take part in the study, due to time constraints at work.
Another limitation of this study – possibly related to the non-significant results – is the small number of participants per group at T2. A larger sample size in the beginning and higher proportions of participants completing the questionnaire at all three measurement points should thus be striven in future studies. Furthermore, the relatively high proportion of drop-outs should also be considered. It is possible, that participants dropped out because of severe back pain experiences. As participants were contacted by work email address sick-listed employees might not be able to take part during the follow ups. This might be one reason for the only low to medium pain intensities and disabilities reported by the participants in this study.
Despite this limitation, the RR between the groups was surprisingly high considering that the RESTQ only measures the actual recovery-stress state of the past three days and nights and is strongly influenced by actual experiences and activities [24, 26]. The stronger differences between the RSG in LBP occurrence at T2 compared to T1 were even more noteworthy. A possible explanation is the chronification of the recovery-stress state. Employees with high stress scores (RSG-1] at T0 might have faced more problems in improving their recovery-stress state in the following months because finding possibilities to recover is more difficult for stressed people due to time concerns and a lack of motivation [26]. Therefore, they might experience an unfavourable recovery-stress state for a longer period than employees in RSG-2, which could improve their recovery over time more easily as they only had stress scores at a medium level. Similarly, RSG-3 might be at a higher risk of experiencing higher stress in the period of investigation compared to the RSG-4 group, given that they already experience a lack of recovery and employees with a lack of recovery have been shown to experience upcoming work demands as being more straining and report a higher need for recovery after work [38, 47].
These hypothetical differences in the stability of the single RSG have to be investigated in future research to further support the predictive power of the group differentiation. The aspect of the duration of the confrontation with stressors is emphasised in several stress-health theories [11, 24] and accumulation of stress over a period of time – as for example during the course of a season in sports – has been identified as a health risk [48]. Unfortunately, the sample used in the present study was too small to reliably analyse the change in the RSG over the follow-up period and its influence on LBP. Future studies are necessary to investigate the influence of changes in the recovery-stress state on LBP occurrence. In addition, it would be interesting to identify the relationship between stress and recovery values and biological aspects, which are associated with LBP occurrence, as for example, inflammatory responses or muscle activation patterns.
Taken together, the identified differences in LBP risk between the recovery-stress states support the theoretical considerations regarding the importance of recovery in relation to stress induced health issues [11, 13]. This study is, to the knowledge of the authors, the first which is investigating the link between the acute stress and recovery state and LBP. Previous studies have mainly focused on the more indirect association of either work condition or recovery experiences with LBP. Those studies had left out one important step as both, work conditions and recovery experiences, are thought to influence the LBP risk by having an impact on the recovery-stress state. The results of this study are a first step to develop a better understanding of the influence of the recovery-stress state on LBP occurrence and they support the idea of stress and recovery as being a central mechanism. Furthermore, the four RSG formed by cluster analysis partly confirmed the groups as mentioned by Kellmann and Kallus [26]. Further studies are necessary to verify the general validity of these RSG and to validate the identified differences in LBP occurrence within different and biggersamples.
In addition to the theoretical significance of the results, they might also be used to individualise LBP prevention programmes for employees. If the presented results could be verified in other professional activities and inhomogeneous samples, this knowledge could be relevant for a pre-screening of employees before taking part in prevention programmes to decide whether they should focus on reducing stress and learn how to cope with work stressors or if they should rather learn how to improve their recovery abilities. Moreover, employees at a high risk of developing LBP might be identified by the use of the RESTQ and the composed RSG, especially if employees remain in an unfavourable recovery-stress state for a longer period.
Funding
The theoretical deliberations of this article have been compiled within the framework of the project “Rückenschmerz” (IIA1-080102B/11-14), initiated and funded by the German Federal Institute of Sport Science and realized within MiSpEx – the National Research Network for Medicine in Spine Exercise.
Conflict of interest
The authors declare that they have no significant competing financial, professional or personal interests that might have influenced the performance or presentation of the work described in this article.