
Abstract
BACKGROUND:
Persistent postural-perceptual dizziness (PPPD) is a functional vestibular disorder that causes chronic dizziness and limits daily activities. Although pharmacology, vestibular rehabilitation, and cognitive behavioral therapy have been proposed to have some efficacy, they have certain limitations. Some patients with PPPD report that public square dancing can effectively relieve the symptoms of dizziness and instability, and their mood improves.
OBJECTIVE:
To evaluate the effects of combining public square dancing with serotonin reuptake inhibitors (SSRIs/SNRIs) on the subjective sensations of dizziness, balance enhancement, anxiety, and depressive symptom regulation in middle-aged and older women with PPPD.
MATERIALS AND METHODS:
In this trial, 124 patients diagnosed with PPPD were enrolled. Among them, 64 patients were randomly assigned to the experimental group (EG), where they received square dance training combined with serotonin reuptake inhibitors. The remaining 60 cases were randomly assigned to the control group (CG), where they received only serotonin reuptake inhibitors and did not participate in organized sports activities, allowing them freedom in their daily lives. Data from the Dizziness Handicap Inventory (DHI), Hospital Anxiety and Depression Scale (HADS), Active-specific Balance Confidence Scale (ABC), and Vestibular Disorder Activities of Daily Living Scale (VADL) were collected and compared at the beginning, 3 months, and 6 months of the trial to evaluate the effect of public square dancing on middle-aged and older women with PPPD.
RESULTS:
There were no significant differences between the EG and CG before the trial. Compared with baseline measures, DHI, HADS, ABC, and VADL scores improved as the experiment progressed, and the improvements were more pronounced in the EG.
CONCLUSION:
Public square dancing combined with serotonin reuptake inhibitors has a positive impact on the subjective sensations of dizziness, balance enhancement, anxiety, and depressive symptom regulation in middle-aged and older women with PPPD.
Introduction
Persistent postural-perceptual dizziness (PPPD) is a functional vestibular disorder characterized by persistent dizziness (≥3 months), nonrotational vertigo, instability, or both. Symptoms can worsen while standing up, exercising, and in complex visual environments [19, 27].
The history of PPPD can be traced back to the Platzschwindel, Platzangst, and Agoraphobie debates among German physicians. They described syndromes of dizziness and discomfort in motion-rich environments, along with autonomic arousal, anxiety, and avoidance of triggering circumstances. Vestibular disorders are also classified as structural, functional, and psychiatric disorders [2, 14]. As otology, neurology, and psychiatry specialties developed, the observation of the patient’s tertiary balance center and a series of studies demonstrated that PPPD is a functional vestibular disorder rather than a structural or psychiatric vestibular disease. Although the term “PPPD” is relatively new, the disorder is not [31]. It has been estimated that PPPD accounts for 15–20% of all patients presenting to the hospital for dizziness and unsteady walking. This condition makes it the most common diagnosis of vestibular disease in young and middle-aged adults and the second most common diagnosis of dizziness in all adults, trailing only benign paroxysmal positional vertigo [22]. Individuals living with PPPD have been found to exhibit reduced efficiency, as evidenced by increased overall sway and poorer performance. These findings align with the theoretical constructs of high-risk postural control strategies and multimodal spatial integration issues compared to controls [28]. Wuehr et al. [38] found increased co-contractions of the lower extremity musculature during static standing in patients with phobic postural vertigo compared with healthy controls, and normalization of body sway and muscle contraction with the addition of a cognitive task. In addition, patients with PPPD often experience anxiety and depression, and most of their personality characteristics tend to be neurotic and introverted [7].
Since PPPD is a chronic nervous system dysfunction manifested as chronic dizziness or imbalance because of the inability to receive effective treatment and often accompanied by psychological disorders, a multidisciplinary treatment approach should be considered [29]. Although several treatments, including pharmacology, vestibular rehabilitation, and cognitive behavioral therapy, are effective, gold-standard guidelines for PPPD treatment are lacking [23, 29]. However, over 30% of patients treated with SSRIs or SNRIs report no significant benefit. Moreover, while vestibular rehabilitation and psychotherapy are usually recommended for mild to moderate PPPD symptoms, they may not provide adequate relief for severe symptoms. Long-term use of SSRIs or SNRIs may cause a series of adverse effects, making patients less compliant with medication adherence. Furthermore, PPPD may involve complex interactions of multi-system abnormalities, including aspects of sensory information integration and central nervous system regulation, this also shows that a single pharmacologic, psychological, or vestibular rehabilitation treatment may not be able to fully address the problem. Therefore, developing an more effective treatment option is a priority.
Public square dancing has become increasingly popular among middle-aged and older women in China because of increased awareness of its health and exercise benefits [21]. It is a special aerobic exercise that integrates body movement, balance and coordination, music experience, social interaction, and other factors. North American and European square dancing is a choreographed dance routine for four couples organized in a square formation. It is a highly social dance that does not involve individual or free-style dancing, and the music is almost always traditional folk. The key distinctions between the North American/European and Chinese versions of square dancing are that in the former, men and women of all ages perform dance routines in groups of four couples, usually in dance halls. Conversely, the latter is favored by middle-aged to older women who dance in larger groups in public squares. Public square dancing can improve behavioral and cognitive function [25] and plays an anti-anxiolytic and anti-depressant role [9]. In addition, it can play a neuroprotective role by regulating dopamine release, increasing the level of brain-derived neurotrophic factor in the hippocampus, and affecting the secretion of specific steroid hormones [10]. Moreover, participating in public square dancing, which involves high social interaction, can improve participants’ quality of life and enhance their mood. This activity can be particularly beneficial for individuals experiencing dizziness and other discomforts. Participating in public square dancing helps to divert their excess attention from their health conditions, achieving the purpose of diversion and improving their sense of dizziness and instability [38]. In addition to the walking, running, jumping, and basic dance movements of public square dancing, participants experience the cheerful music rhythm and practice single-foot support. Moreover, participants must actively adjust their body posture to maintain balance, and eventually, they effectively increase muscle strength, body flexibility, and coordination and improve their dynamic balance. In addition, public square dancing participants need to rotate their bodies constantly during activities, thereby improving their visual field. This aspect strengthens the body’s ability to deal with vestibular sensation, vision, and proprioception to a certain extent and promotes the vestibular function’s dynamic recovery ability. According to the above speculation, it is possible that public square dancing may improve the clinical symptoms of dizziness, instability, anxiety, and depression in middle-aged and older women with PPPD. However, no study has comparatively evaluated the effects of public square dancing on patients with PPPD. Research on the effects of public square dancing may offer positive guidance to people with PPPD in selecting an appropriate exercise program.
This study aimed to assess the effects of public square dance exercises combined with SSRIs or SNRIs on middle-aged to older women with PPPD. We assessed and compared the effect of pre-treatment and post-treatment scores on various scales to evaluate the impact of vestibular disorders on patients’ daily lives. These scales include the Dizziness Handicap Inventory (DHI), a standard questionnaire that quantitatively measures the degree of handicap experienced by patients with vestibular disorders [13], the Hospital Anxiety and Depression Scale (HADS), which measures the severity of depressive or anxiety symptoms, the Activities-specific Balance Confidence scale (ABC), which assesses the confidence of performing 16 daily activities without falling, and the Vestibular Disorders Activities of Daily Living scale (VADL). We hypothesize that public square dancing combined with serotonin reuptake inhibitors can improve behavioral cognition, promote vestibular function rehabilitation, relieve anxiety and depression, and alleviate the symptoms of PPPD in middle-aged and older women.
Materials and methods
Study design and participants
This randomized controlled trial was conducted at the First Hospital of Changsha, Hunan Province, China. First, we enrolled 130 patients and divided them into an experimental group (EG) and a control group (CG). Patients in both groups had previously undergone treatment with SSRIs or SNRIs such as sertraline, escitalopram, etc., but had poor responses to these medications.
In this study, the EG group received square dancing training in addition to SSRIs or SNRIs, while the CG group only received SSRIs or SNRIs. The participants in the CG did not engage in any organized sports activities and had freedom in their daily lives. However, six patients were excluded from the study for the following reasons: one patient in EG was incapacitated by an accidental fracture, and five patients in CG did not adhere to their prescribed medication regimen. The predisposing diseases of PPPD in both groups are shown in Table 1.
Predisposing diseases of PPPD in two groups of patients
Predisposing diseases of PPPD in two groups of patients
Abbreviations: CG, control group; EG, experimental group.
Middle-aged and older women with PPPD between 45 and 75 years were recruited from the neurology outpatient clinic and hospital ward in the First Hospital of Changsha between June 2020 and May 2022. PPPD was diagnosed by a licensed neurologist (SN) according to the diagnostic criteria for PPPD established by the Classification Committee of the Bárány Society [31]. Patients were recommended to start and continue maintenance treatment with SSRIs or SNRIs for at least 3 weeks before and during the study period to minimize the possible confounding effects of side effects. The exclusion criteria were neurological disorders other than PPPD, psychiatric disorders (e.g., generalized anxiety disorder or major depressive disorder), history of head trauma with loss of consciousness, and pregnancy. The Ethics Committee of the First Hospital of Changsha, Hunan, China, approved the study protocol.
The EG was simultaneously supplemented with a public square dancing treatment based on medication. It is a popular form of aerobic exercise for middle-aged and older women. Public square dancing features a simple and easy-to-learn structure, making it accessible for older individuals as a form of exercise. We selected dance music with simple melodies and low-movement activities for our study. The main movements involved hand clapping, high-fiving, chest expansion, arm extension, and leg kicking.
According to previous literature [4], the public square dance workouts were conducted outdoors three times a week, with each session lasting 30 min. These sessions were scheduled for Mondays, Wednesdays, and Fridays, starting at 7 p.m. In cases of inclement weather, the sessions were moved indoors. The public square dance exercise was led by two knowledgeable individuals who volunteered to guide the participants in the dance movements. Before the training, there were 5-min warm-up activities, including finger joint activities. The main dance lasted 30 min, followed by 5 min of relaxation exercises involving deep breathing and stretching. During the public square dance exercise, participants agreed to wear a sports watch to monitor their heart rate. Exercise intensity was assessed by targeting the heart rate at 100–140 beats/min. The CG group did not receive any placebo to account for non-specific effects of drug administration, nor did they undergo any other physical intervention to control for the non-specific effects of regular physical activity.
Outcome measures
The DHI is a 25-item questionnaire that measures the patient’s self-perceived handicap and its impact on their quality of life concerning dizziness. It assessed three domains: physical, functional, and emotional. The questionnaire provides a total score of 100, with higher scores indicating a greater impact of the patient’s symptoms on their quality of life. This questionnaire was chosen because it has been validated [13], has high test-retest reliability, and is widely used in clinics and research to measure the improvement in symptoms associated with public square dancing. The minimally clinically important change is 18 points between pre- and post-treatment (95% confidence interval [CI]) to indicate a significant change in self-perceived handicap [13].
The HADS [40] is a self-report questionnaire comprising 14 questions, each rated on a 4-point scale. The anxiety and depression scales include seven items. This psychometric instrument was chosen because all items exclude physical symptoms and refer to only emotional statese.
The ABC Scale [24] comprehensively assesses the patient’s confidence in not falling while performing 16 daily activities. A score of 0 indicates that the patient consistently falls while performing the exercise and fears losing his balance, whereas a score of 100 indicates that he is 100% confident that he will not fall.
The VADL was developed by Cohen et al. [5]. The scale has three subscales: functional, ambulation, and instrumental. The scale has 28 items, each scored from 1 to 10, giving 280 points. Means were calculated for the sub-scores and total scores. It is a reliable scale for evaluating adult patients with vertigo and dizziness [5, 6].
Statistical analysis
Statistical analyses were performed using SPSS 23.0. Kolmogorov–Smirnov test or Shapiro–Wilk test were used to test the normal distribution of the continuous variables, with p > 0.05 considered to obey the normal distribution and normally distributed with mean±standard deviation (x±s), according to comparison between groups using an independent sample t-test. If the distribution was non-normal, the median and interquartile range were used to describe the distribution, and the Mann–Whitney non-parametric rank sum test was used to compare groups. Independent t-tests compared the EG and CGs’ baseline demographics and outcome variables. A repeated measure ANOVA was used to compare scale scores at different time points. Statistical significance was set at p < 0.05. Data analyses were performed according to the principle of completing all experiments, and missing data were not included in the results.
Results
Baseline participant characteristics
All experimental tests were completed by 124 participants, with 64 in the EG and 60 in the CG. Table 2 presents the participants’ basic characteristics. There were no significant differences between the CG and CG regarding baseline characteristics such as age, subjects on central nervous system medication, disease duration, DHI, HADS, ABC, and VADL scores (p > 0.05).
Baseline characteristics of participants
Baseline characteristics of participants
Continuous variables are presented as the mean±standard deviation. Abbreviations: DHI, Dizziness Handicap Inventory; HADS-A, Hospital Anxiety and Depression Scale for Anxiety; HADS-D, Hospital Anxiety and Depression Scale for Depression; ABC, Activities-Specific Balance Confidence Scale; VADL, Vestibular Disorders Activities of Daily Living Scale; CNS,; CG, control group; EG, experimental group.
A series of subjective self-report measures were taken at baseline, 3 months, and 6 months to document the efficacy of public square dancing in the EG. Table 3 compares the results of the CG and EG over time.
Comparison of outcomes at baseline, three months and six months between the two groups of patients
Comparison of outcomes at baseline, three months and six months between the two groups of patients
*P < 0.05, **P < 0.001. Abbreviations: DHI, Dizziness Handicap Inventory; HADS-A, Hospital Anxiety and Depression Scale for Anxiety; HADS-D, Hospital Anxiety and Depression Scale for Depression; ABC, Activities-Specific Balance Confidence Scale; VADL, Vestibular Disorders Activities of Daily Living Scale; CG, control group; EG, experimental group.
The two groups’ DHI, HADS-A, HADS-D, ABC, and VADL scores were compared at different time points using the Mauchly spherical test (p < 0.01). The data did not conform to spherical data, indicating a correlation between the results of multiple measurements. Therefore, a repeated measures ANOVA was performed. The results demonstrated that the total scores of DHI, HADS-A, HADS-D, and VADL in the CG and EG decreased over time, while the score of ABC increased, and the differences were very significant (p < 0.001). The interaction effect of group and time was very significant for DHI, HADS-A, HADS-D, and ABC (p < 0.001). It was significant for VADL (p < 0.05), with significant differences among different interventions (p < 0.001).
An independent sample t-test was used to compare the scores of each scale between the CG and EG. The results showed that the DHI scores (EG: 33.7±9.7; CG: 42.4±14.8; p < 0.001), HADS-A scores (EG: 7.39±2.13; CG: 8.25±2.07; p = 0.02), HADS-D scores (EG: 7.56±3.08; CG: 9.12±2.64; p = 0.003), ABC scores (EG: 102.7±22.1; CG: 85.3±18.1; p < 0.001) and VADL scores (EG: 65.3±16.9; CG: 76.8±20.9; p = 0.001) were significantly different between the EG and CG at 3 months. In addition, like at month 3, at month 6, the DHI scores (EG: 22.0±7.7; CG: 32.6±11.1; p < 0.001), HADS-A scores (EG: 5.19±1.94; CG: 6.97±2.67; p < 0.001), HADS-D scores (EG: 5.19±2.43; CG: 7.98±2.45; p < 0.001), ABC scores (EG: 116.3±24.6; CG: 98.1±23.1; p < 0.001) and VADL scores (EG: 50.2±12.4; CG: 60.7±23.7; p = 0.002) remained significantly different between the two groups.
Statistical analysis showed that time and group significantly affected the composite score. Figures 1–5 show the composite score for each group over time, where a score improvement is observed and the degree of change is significantly different between the groups. There was no difference in the starting point of the composite score between the CG and the EG. However, a significant group effect was observed for each specific observation’s scores at different points in time. Furthermore, a significant overall time effect was observed, indicating a trend of improvement for both groups. The degree of improvement in EG was more noticeable than that in CG.
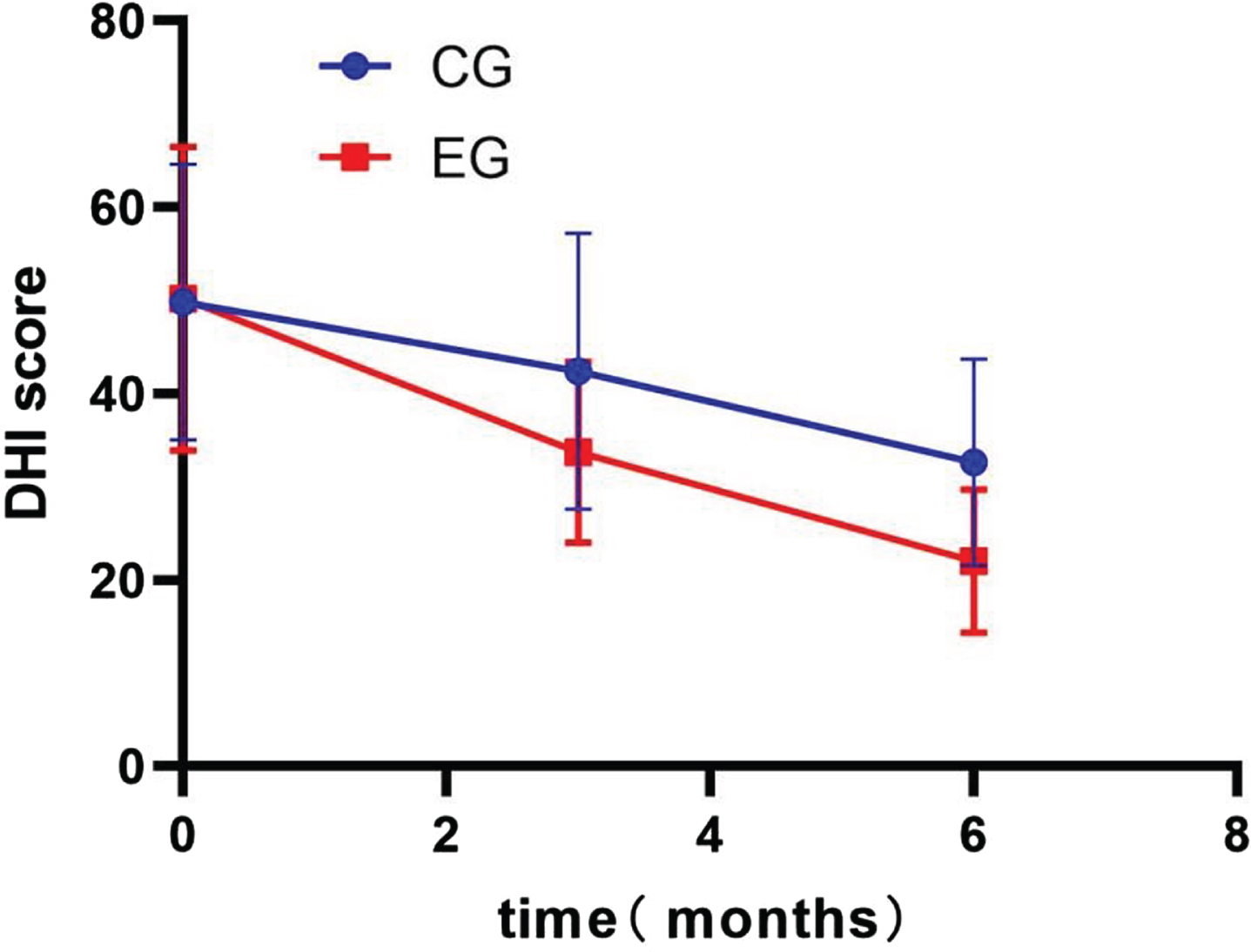
Changes in the Dizziness Handicap Inventory (DHI) total score. CG, control group; EG, experimental group.
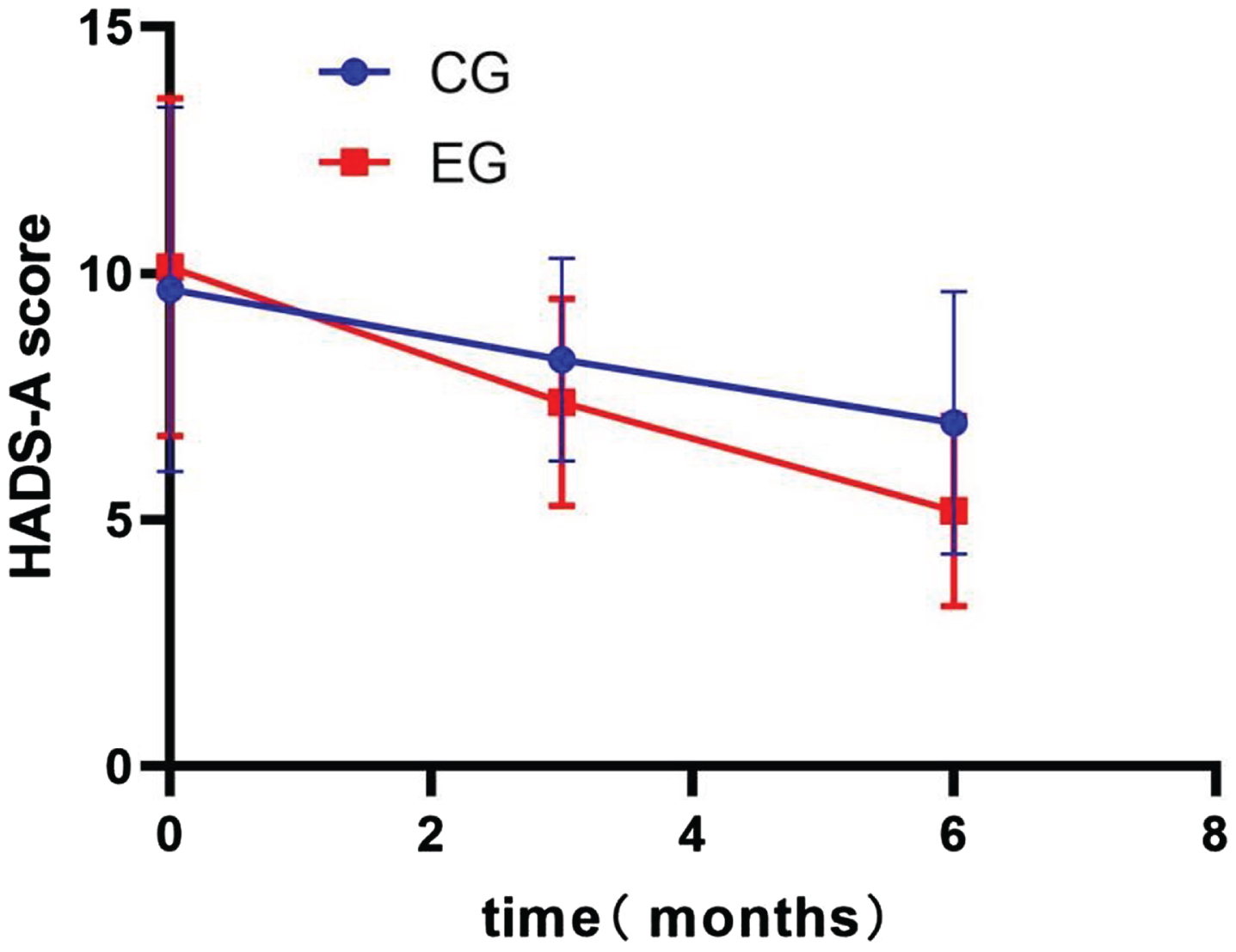
Changes in the Hospital Anxiety and Depression Scale for Anxiety (HADS-A) total score. CG, control group; EG, experimental group.
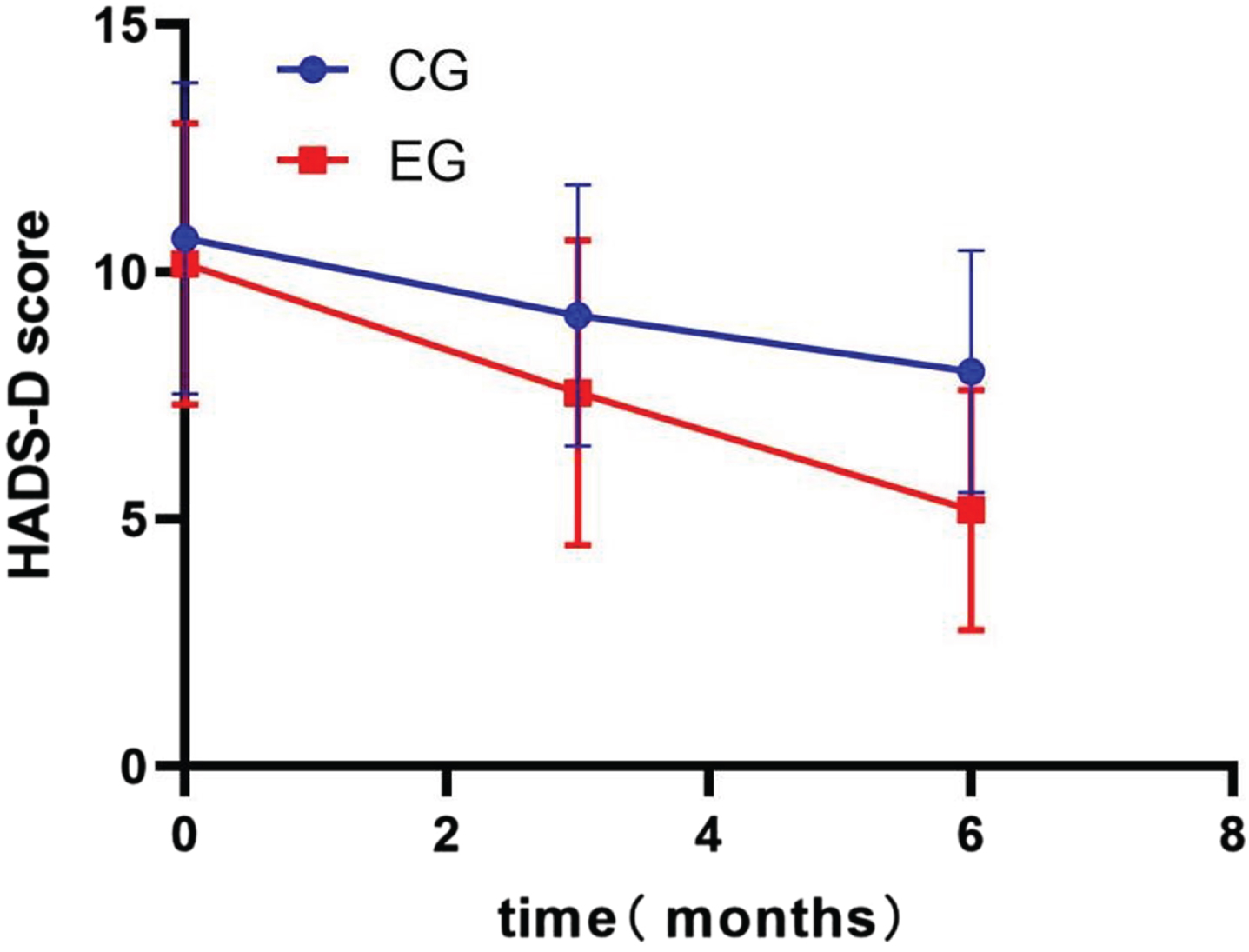
Changes in the Hospital Anxiety and Depression Scale for Depression (HADS-D) total score. CG, control group; EG, experimental group.
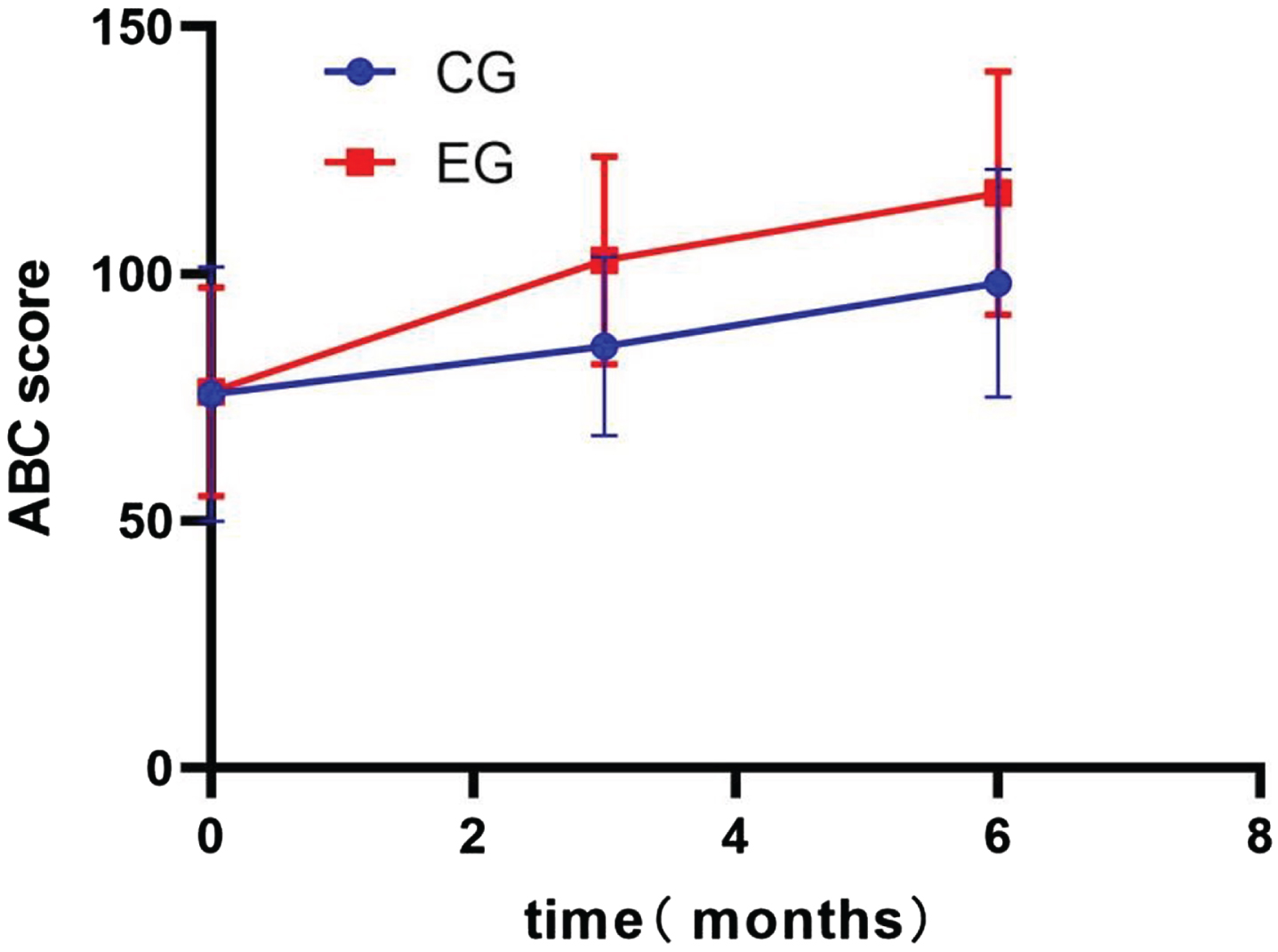
Changes in the Activities-Specific Balance Confidence Scale (ABC) total score. CG, control group; EG, experimental group.
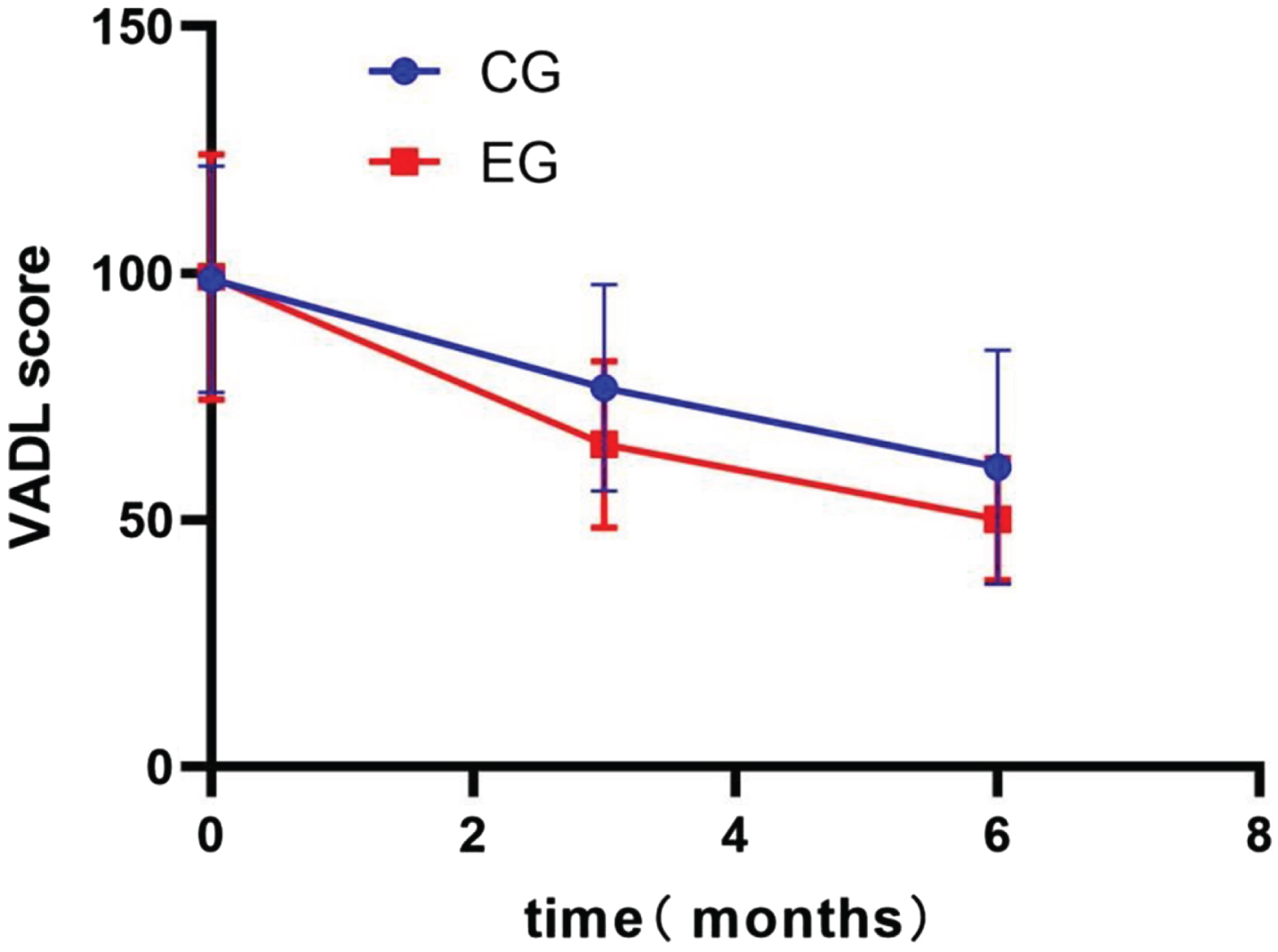
Changes in the Vestibular Disorders Activities of Daily Living Scale (VADL) total score. CG, control group; EG, experimental group.
As a newly defined syndrome, PPPD encompasses the main characteristics of the lesions, including phobic postural vertigo (PPV), chronic subjective dizziness (CSD), and related disorders [31], which are more comprehensive and specific than previous definitions. Although the exact pathophysiological mechanism of PPPD has not been clarified in academic circles, three key mechanisms for the occurrence and development of PPPD are excessively rigid posture when walking or standing, excessive dependence on visual information rather than vestibular input information when processing spatial orientation information, and failure of the higher cortex in regulating the first two processes [12, 28]. The cognitive-behavioral response to this state is often followed by psychological and functional disorders such as fear of falling, anxiety or depression, and postural gait abnormalities [16, 26]. Based on the above mechanisms, the current commonly used therapeutic strategies for PPPD involve treating comorbid vestibular disorders, adjusting sensory posture, and increasing tolerance to sensory stimuli through desensitization.
This randomized controlled study verified the application value of public square dancing in middle-aged and older women with PPPD, which can relieve patient symptoms and promote their recovery. We observed significant decreases in DHI, HADS, and VADL scores among patients with PPPD who participated in public square dancing compared to the CG who did not engage in this activity. Additionally, there was a significant increase in ABC scores, indicating a reduction in vertigo disability, mood improvement, and overall quality of life. These improvements were sustained even after 6 months. This is the first study in China to examine the effect of public square dancing on individuals with PPPD. We chose public square dancing because it is easy to learn, does not require specialized equipment or venues, and is easily accessible, which is particularly beneficial for older participants with PPPD. The favorable attendance rate and absence of adverse events further support the feasibility of this intervention trial.
This study demonstrated that after 3 months of public square dance training, there was a significant decrease in negative emotional indicators such as anxiety and depression. Furthermore, as the training duration extended to 6 months, the improvement effect became even more pronounced. The reason may be attributed to the fact that public square dance exercise falls under the category of aerobic exercise. Many previous studies have confirmed that aerobic exercise improves mood by increasing positive emotions and reducing negative emotions such as anxiety and depression [1, 35], which is confirmed in this study. The mechanism may be based on the fact that square dancing involves focusing on dance movements and steps while also allowing dancing participants to feel the melody and beat of the music, resulting in a pleasurable emotional experience. In addition, aerobic exercise causes the body to produce more beta-endorphins, which not only improve mood but can improve memory. Furthermore, compared to the CG, individuals who partake in public square dancing were able to share life experiences, alleviate feelings of helplessness and anxiety, reduce their ideological pressure, relax their mood, and obtain valuable experience of daily health care, thereby eliminating loneliness and improving their mood [17].
Regarding DHI and VADL scores, our study revealed a significant main effect over time. The gradual decrease in dizziness symptoms over time in both groups could be because of the effects of SSRIs, as the efficacy of serotonergic medication in PPPD has been proven in previous studies [32, 39]. HADS-D scores were used to measure the severity of depressive symptoms, and HADS-A scores were used to measure the severity of anxiety symptoms. In patients in the EG, the above scores decreased to the normal range and remained at the level of maintaining mildness in patients in the CG.
Previous research has revealed that most individuals suffering from PPPD are often triggered by vestibular disorders, most commonly vestibular migraine, or other medical conditions. Additionally, some are associated with acute psychological trauma that gradually transforms into a functional disease with recurrent symptoms [33, 36]. Our investigation once again confirms this fact. Although most patients with PPPD have normal vestibular function, a significant proportion exhibit vestibular abnormalities. These abnormalities include isolated unilateral otolith dysfunction based on assessments such as static bias, cervical vestibular evoked myogenic potential (cVEMP), and ocular vestibular evoked myogenic potential (oVEMP) assessments [36]. Although vestibular dysfunction is present in a subset of patients with PPPD and restoring normal head and body movement strategies appears crucial for recovery, there is no evidence to suggest that this vestibular compensation pattern is the underlying mechanism for PPPD improvement. In public square dancing, participants engage in repetitive and simplistic movements while maintaining an emotionally relaxed state, which prior research has shown to desensitize the balance control system in a “high alert” state among individuals with PPPD [20, 37]. Moreover, studies have shown that exposure and appropriate physical behavior can help patients with PPPD develop reasonable awareness and promote self-controlled desensitization, thereby alleviating their symptoms [8]. This aspect is also present among public square dance participants. In addition, some studies have found that repetitive head and neck movements can effectively reduce sensitivity to one’s movements and compensate for dynamic vision by utilizing other sensory systems [15, 29]. These adaptive mechanisms can help patients with PPPD better adapt to their surroundings and alleviate symptoms. Considering these factors, we propose that the movements featured in public square dancing may alleviate symptoms by reducing visual motor perception in patients with PPPD. This effect may contribute to helping patients better adapt to their environment and reducing their discomfort. Through this study, we observed that after participating in public square dance exercise for 3–6 months, the patients with PPPD displayed a significant reduction in their DHI and VADL scores, strongly indicating that public square dancing has a positive impact on alleviating dizziness and balance-related symptoms in these patients.
Public square dancing is a promising nonpharmacological intervention strategy for middle-aged and older adults with PPPD. A 6-month daily exercise intervention can improve overall dizziness, depressive or anxiety symptoms, balance, and quality of life in middle-aged and older women with PPPD. Public square dancing, an affordable form of exercise, is suitable for communities and other areas where middle-aged and older women are concentrated. Exercise in such an environment improves mood and is equally beneficial for improving cognition. We recommend practicing once daily for about 30 min, three times a week, preferably for 6 months. However, because of the dizziness and instability symptoms of patients with PPPD, primary hospitals or communities should evaluate patients’ physical conditions when organizing public square dance exercises, provide the necessary guidance, supervise these exercises, and prevent patients from falling and other adverse events.
This study demonstrated the feasibility of public square dancing, whose importance is being acknowledged. One potential weakness of this study is that the CG received no intervention other than medication.Nevertheless, we maintained that the observed improvement in the EG cannot be solely attributed to the medication alone. Notably, in the CG, participants received no additional human intervention other than the medication. Their symptoms did improve, but the degree of improvement was not as significant as that observed in the EG. Moreover, this study is also subject to other limitations. First, the participants were recruited from a single center, and future multicenter studies are needed to confirm our findings. Second, the assessment instrument used only scale measures. Future studies, including the vestibular function examination and functional magnetic resonance imaging, might provide more information about the effect of public square dancing in patients with PPPD. Third, this study only discuss PPPD in middle-aged and older women, and its applicability in men remain to be further explored.
Conclusion
This study investigated the effects of public square dancing combined with serotonin reuptake inhibitors in middle-aged and women with PPPD. This study supports the positive effects of public square dancing in improving dizziness, depression or anxiety, balance, and quality of life in middle-aged and women with PPPD.
Data availability statement
The original data supporting the conclusions of this study will be provided by the authors without reservations.
Ethics statement
The studies involving human participants were reviewed and approved by the Scientific and Ethics Committee of the First Hospital of Changsha. The patients provided written informed consent to participate in the study.
Author contributions
Xiaojun Yu and Bo Tang conceived of and designed the study. Xiaojun Yu obtained the funding. Wei Jiang, Chuang Zhang, and Hong Tan supervised this study. Bo Tang, Yuqing He, Minghua Luo, and Chuang Zhang collected the data. Xiaojun Yu independently performed randomization. Bo Tang and Xiaojun Yu performed data analysis and wrote the first draft of the manuscript. All authors contributed to manuscript revisions and read and approved the final version of the manuscript for submission.
Funding
This study was funded by the Hunan Provincial Science and Technology Department Natural Science Foundation Science and Health Joint Project (No.2021JJ70126).
Footnotes
Acknowledgments
We sincerely thank all the volunteers who participated in this study. We also thank the reviewers for their comments and suggestions.