
Abstract
BACKGROUND:
The technique of measuring ocular vestibular evoked myogenic potentials (oVEMP) in response to Mini-shaker vibration is relatively new, there is a limited normative data to define the presence or absence of a response in the literature.
OBJECTIVE:
To determine the test-retest reliability of cervical and ocular VEMPs (cVEMP and oVEMP, respectively) to air-conducted sound (ACS) and bone-conducted vibration (BCV) stimulation and to determine normative ranges for the responses.
METHODS:
Twenty normal-hearing individuals (40 ears) and 20 hearing impaired volunteers with normal balance function (40 ears) were examined in this study. ACS cVEMP and BCV oVEMP (using a Mini-shaker) were recorded from both groups to assess the test-retest reliability and to collect normative VEMP data for P1/N1 latencies and amplitudes from 20 normal hearing individuals. To test reliability, VEMP recordings were repeated within the same session.
RESULTS:
The test-retest reliability for all the cVEMP parameters showed excellent reliability whereas oVEMP parameters showed between fair and excellent reliability depending on the parameter tested. Normative data for VEMP P1/N1 latencies and amplitudes were established.
CONCLUSIONS:
Normative data and test-retest reliability for BCV oVEMP using the Mini-shaker at 100 Hz were established in our study for the first time in the literature. Responses appear reliable.
Introduction
Vestibular evoked myogenic potentials (VEMPs) are widely used in clinical practice as an objective vestibular technique for measuring otolith organ (saccular and utricular) function. VEMPs are short-latency myogenic potentials that can be elicited using several ways including high-level air-conducted sound (ACS) (clicks or tone-bursts), bone-conducted vibration (BCV), mechanically tapping on the forehead, or electrical stimulation [24, 35]. VEMPs have been recorded from different muscles. VEMPs that are recorded from the contracted neck muscles e.g. the sternocleidomastoid (SCM) muscle are referred to as cervical VEMPs (cVEMPs), while those recorded from the eye muscles (extraocular muscle) are termed ocular VEMPs (oVEMPs) [21, 35].
Stimulation of the saccular afferents with a high-level of either ACS or BCV causes inhibition of electromyography (EMG) activity of the contracted SCM muscle as a manifestation of the vestibulo-collic reflex (VCR) [24]. Activation of utricular afferents by either ACS or BCV results in extraocular muscle activity as a manifestation of the vestibulo-ocular reflex (VOR) [24]. There is still some debate in the literature as to whether it is the type of measurement (e.g. cVEMP or oVEMP) or the stimulation method (sound or vibration) that determines which end organ is tested with VEMP (see [31], for a review). Curthoys [6] proposed that oVEMPs reflect contralateral utricular function and cVEMPs reflect ipsilateral saccular function. Hence, oVEMP and cVEMP are independent measures that can be used to discriminate responses of the saccular and utricular macula due to differential neural projections to various muscle groups. However, Todd et al. [29] suggests that it is the type of stimulation used that determines which end organ is selected, with 100 Hz low-frequency vibration selectively stimulating the utricle when the stimulus applied to the mastoid, so that the acceleration occurred mainly in the interaural axis and 500 Hz sound selectively stimulating the saccule. There does however appear to be agreement in the literature that sound elicited cVEMPs using 500 Hz tone-burst predominantly reflect saccular function [1, 28]. It has been proposed that oVEMPs elicited using 100 Hz low-frequency vibration mainly reflect utricular function [25]. On the other hand, Curthoys [6] have shown that low frequency vibration (including at 100 Hz), will also stimulate some semicircular canal afferents, and thus animal studies show less frequency specificity at 100 Hz.
Sufficient vibratory output to evoke oVEMP at 100 Hz can be achieved using a Mini-shaker, such as the Bruel and Kjer 4810, which, compared to the classical bone conductor, yields a more reliable and consistent response and a higher response prevalence [8, 11]. However, the Mini-shaker weighs around 1.1 Kg and for clinical use is likely to be held manually on the patient’s mastoid process. Due to size of the Mini-shaker, it is important to explore whether the positioning of the Mini-shaker on the patient’s mastoid affects the reliability of oVEMP responses. In the research literature to date, only one study [8] has measured the test-retest reliability of BCV oVEMP and cVEMP in terms of the peak-to-peak amplitude parameter for three different stimulation devices (B-71, impulse hammer, and Mini-shaker) in three age groups. However, they only used 500 Hz tone-burst stimulus to elicit BCV VEMP. Several studies have reported a trend of inverse correlation between VEMP amplitude and age [8, 34]. Greenwalt et al. [8] found that the BCV oVEMP and ACS cVEMP amplitudes were negatively correlated with age. However, age was positively correlated with ACS oVEMP and BCV cVEMP amplitudes. This could be related to the type of stimulation used to elicit cVEMP and oVEMP. As suggested by Todd et al. [29], 100 Hz low-frequency vibration may be selectively stimulating the utricle and 500 Hz sound the saccule [32].
Since the technique of measuring oVEMP in response to Mini-shaker vibration is relatively new [16, 29], there is limited normative data to define the presence or absence of a response in the literature. The aims of the present study were to measure the reliability of 100 Hz Mini-shaker responses and 500 Hz AC responses and to determine the normative ranges of the 100 Hz response.
Previous studies have revealed that hearing impaired patients with normal vestibular function have VEMPs, whereas patients with normal hearing and vestibular loss do not have VEMPs confirming the vestibular origin of VEMPs [5, 11]. In the current study we included a hearing-impaired group to demonstrate that neither AC, nor minishaker VEMPs are affected by hearing impairment.
Methods
The design of this study was cross sectional. A convenience sample of normal control subjects and hearing-impaired patients were recruited in this study. oVEMP responses to vibration using the mini-shaker and cVEMP responses to ACS were collected from all subjects, twice in the same session to assess intra-subject reliability.
This study was approved by the University of Jordan ethics committee (5–2021) before the research commenced. Participants gave informed consent prior to conducting the procedures of this study.
Participants
Normative group
Twenty control participants (11 males and 9 females) aged between 27 and 55 years, with a mean age of 33 years were recruited in the study. A screening questionnaire was used to rule out any balance problems, neck/back stiffness or pain, and major visual problems that could not be corrected with eyeglasses or contact lenses. All normal participants had pure-tone thresholds of 20 dB hearing level (HL) or better (normal hearing). oVEMP responses to vibration using the Mini-shaker and cVEMP responses to ACS were recorded from all participants (40 ears).
Hearing impaired participants and vestibular loss control
Twenty participants with severe to profound sensory-neural hearing loss (SNHL) (10 males and 10 females) aged between 30 and 60 years, with a mean age of 48 years were recruited in this study. Participants who had back/neck pain, visual problems, outer and middle ear pathology (e.g. excessive wax, infection, ear discharge or bleeding), balance problems, and allergy to alcohol swab were excluded from this study. A modified version of the Vestibular Rehabilitation Benefit Questionnaire (VRBQ) (http://www.isvr.soton.ac.uk/audiology/vrbq.htm) was used to rule out balance problems. The majority of the participants (15) included in the study had acquired SNHL from unknown causes. Two participants had congenital hearing-impairment due to maternal rubella and three participants had bacterial meningitis. oVEMP responses to vibration using the Mini-shaker and cVEMP responses to ACS were recorded from all participants (40 ears).
Control recordings were also made from one subject with bilateral hypofunction.
Apparatus and stimulus
VEMP testing
cVEMP was measured using Cambridge Electronic Device’s CED 1401 data acquisition system and CED “signal” software (http://ced.co.uk/). A sampling rate (input and output) of 10000 Hz was used. The output from the Digital to Analogue Converters (DAC) port was routed through a headphone amplifier (OBH-21) to control the intensity of the stimulus. Amplification of the signals was performed using an isolated amplifier (CED 1902) with a 1–3000 Hz bandpass filter with 1000 times gain. Vibration oVEMP was measured using the Bio-Logic Auditory Evoked Potentials system (AEP version 6.2.0) through a Mini-shaker which is part of a ‘vibrotactile perception meter’ (VPM) system for measuring vibrotactile thresholds. The VPM consists of an amplifier which can input an external signal and use it to drive a small shaker. The shaker includes a force meter, so the force applied to the head is seen on the VPM amplifier. The shaker also has an accelerometer built into the tip that is applied to the head, so the acceleration of the target area is known. The acceleration signal can be output from the system for measurement/calibration of the applied force.
For AC cVEMP, 500 Hz 4 cycle tone-burst stimuli with 1-cycle (2 ms) rise/fall, and 2-cycle plateau were presented using insert earphones (Etymotic ER-3A) at sound intensity level of 90 dB normal HL (nHL) (127 dB SPL). The zero nHL reference used was previously established in normal hearing participants (Obeidat and Bell, 2018) and represents the mean threshold of normal hearing stimuli to the tone-burst stimuli. Each recording consisted of 150 repeats of an 8 ms short tone-burst. A repetition rate of 10 Hz was fixed for all measurements, so the total duration for each recording was 15 s. The rate of 10 Hz was found to be the optimal trade-off between recording time and response detection for the majority of participants in our previous study [18]. Four recordings (2 recordings for each ear) were repeated to give a total exposure time of 60 s.
Vibration oVEMPs were measured using 40 ms tone bursts at 100 Hz (delivered via mini-shaker) with a root mean square (rms) level of 1 ms–2 applied to the mastoid bone directly behind the auricle. Rise/fall times were 10 ms (1 cycle) with a 20 ms (2 cycle) plateau. For each condition, 150 epochs at 2.5 Hz stimulation rate were generated (60 s exposure). Four recordings were repeated to give a total exposure time of 240 s. The tone-pip output from the Bio-Logic AEP system (version 6.2.0) was routed into the VPM, which amplifies the tone-pip signal to drive the mini-shaker at the mastoid. The mini-shaker was applied to the head with a force of 10 Newtons (N), as indicated on a calibrated force meter. It should be noted that different head masses/impedance can result in different resulting acceleration at the mastoid for the same drive signal. We intended to apply the same acceleration to all participants as measured at the measurement tip of the mini-shaker. To achieve this, the acceleration signal from the mini-shaker was measured on an oscilloscope and the drive signal was adjusted in-order to target an acceleration of 10 ms–2 rms at the mastoid.
We did not calibrate the dB FL of the stimuli at the time of the study, but a recent calibration with the same equipment found a 1 ms–2 acceleration at 125 Hz produces 111 dB FL, so the 100 Hz stimulation used in the current study should be close to this value.
Procedures
cVEMP recording
VEMPs from the SCM muscle were recorded ipsilaterally while participants were seated upright on a chair with their chin turned over the contralateral shoulder to tense the SCM muscle. The EMG activity of the SCM muscle was recorded using surface electrodes placed on the muscle: active on the belly of the ipsilateral SCM muscle, and reference on the upper sternum of the test side. A ground electrode was placed on lower forehead. The impedance of the electrodes was kept below 10 kΩ. The EMG activity of the SCM muscle was visually monitored in real-time by the investigator and subject, using a digital oscilloscope (TDS 210), and the subject was asked to maintain the level between 80 and 100 mV throughout the recording.
oVEMP recording
VEMPs from the ocular muscles were measured for each ear contralateral to the stimulated ear in response to vibration. The responses were recorded from both ears by placing five electrodes on the face. The two active pairs of electrodes were placed on the orbital margin below the center of the eye and referred to 2 reference pairs of electrodes approximately 15–30 mm below, on the cheek, and the ground electrode low on the forehead. The impedance of the electrodes was maintained below 10 kΩ. Participants sat on a chair and were asked to look up at a target located 2 meters away, with an elevation of 25 degrees, whilst vibrations were applied to subject’s tested ear via the mini-shaker at the mastoid process (behind the pinna of the ear). The participants were tested with the same angle of elevation and with rest breaks to allow the participants to blink.
Response analysis
cVEMP
The presence of the responses was objectively detected using a one-sample Hotelling’s T2 test (HT2; Hotelling, 1931) on the array of cVEMP data with a detection p-value of 0.05 (false positive rate of 5%). For more detailed of the method see Chesnaye et al. [3] and Obeidat and Bell [17].
oVEMP
oVEMP responses were measured on clinical equipment that did not have HT2 detection available. Instead oVEMP responses were deemed to be present if the oVEMP waveforms were reproducible, biphasic with a negative (N1) peak followed by a positive peak (P1), peak-to-peak amplitude and peak latencies should be within the 95% range that was determined from a recent study [16] using oVEMP evoked by 40 ms tone bursts at 100 Hz in 10 adults with no history of hearing and balance problems.
Exploring Artefact in oVEMP responses
A possible concern was whether there was a stimulus artefact on the BCV oVEMP responses. With vibration induced o-VEMP, the response occurs at the stimulation frequency and may be a high frequency manifestation of the linear VOR [30]. The long low frequency stimulus can also overlap the response of interest, so it is important to confirm that the response seen is not stimulus artefact. One approach to confirm that the response is physiological is to demonstrate that the response amplitude depends on eye position, which has been demonstrated for oVEMP [25], but would not be the case for a stimulus artefact. Five participants with normal hearing and balance function were tested with vibration oVEMP by using two different gaze positions (up and straight) in order to determine whether latency and amplitude of BCV oVEMP are affected by gaze position.
Statistical analysis
Descriptive statistics were computed for demographics and study data. The mean±1.96×SD of amplitude (uV), and latencies P1-N1(ms) of c–and oVEMPs at 90 dB nHL for the 2 testing measurements were used to set the limits for normality.
Intra-subject reliability was estimated using the intra-class correlation coefficient (ICC) (2-way random, absolute agreement) with the 95% CI. An ICC of less than 0.40 indicates “poor” reliability, 0.40 to 0.74 indicates “fair to good” reliability, and an ICC that is more than 0.75 indicates “excellent” reliability [26].
The correlation between age, amplitude, and latencies (P1 and N1) of the oVEMP and cVEMP for normal participants and hearing-impaired participants was calculated using Spearman correlation coefficient from measurement 1. A Spearman correlation coefficient ≥0.60 indicates “strong” correlation, while 0.31 and 0.59 indicates “moderate” correlation and <0.30 indicates “poor” correlation [4]. The differences in VEMP amplitudes and latencies between normal control participants and hearing-impaired participants for the two measurements were calculated using the Mann-Whitney U test.
Results
The effect of gaze position on oVEMP peak to peak amplitude
Peak to peak amplitude was bigger in gaze-up (6.71 uV) than in gaze-straight (1.77 uV). The pattern is consistent with the expected pattern for a physiological o-VEMP response, with a larger response arising from the extraocular muscle (inferior oblique muscles) with eyes elevated and a smaller response seen in neutral gaze position representing the summation of responses for all tonically active muscles [25]. As response amplitude is clearly dependent on eye position, we were confident that BCV oVEMP responses are physiological in origin rather than resulting from artifact.
ACS cVEMP and BCV oVEMP responses for a healthy subject and a subject with bilateral vestibular loss
In addition to the main test group, we also tested responses from a subject with bilateral vestibular loss as a control condition. The absence of BCV oVEMP response in a subject with bilateral vestibular hypofunction was further evidence that BCV oVEMP responses are not stimulus artefact. Figure 1 below shows ACS cVEMP and BCV oVEMP responses obtained from a healthy subject (left panel), and a subject with bilateral vestibular loss (right panel) using the Bio-Logic Auditory Evoked Potentials system (version 6.2.0). The healthy subject displays normal P1-N1 from both SCM muscles and N1-P1 responses beneath both eyes. The subject with bilateral vestibular loss has no P1-N1 from both SCM muscles and N1-P1 responses beneath both eyes, which is consistent with bilateral loss of otolithic function.
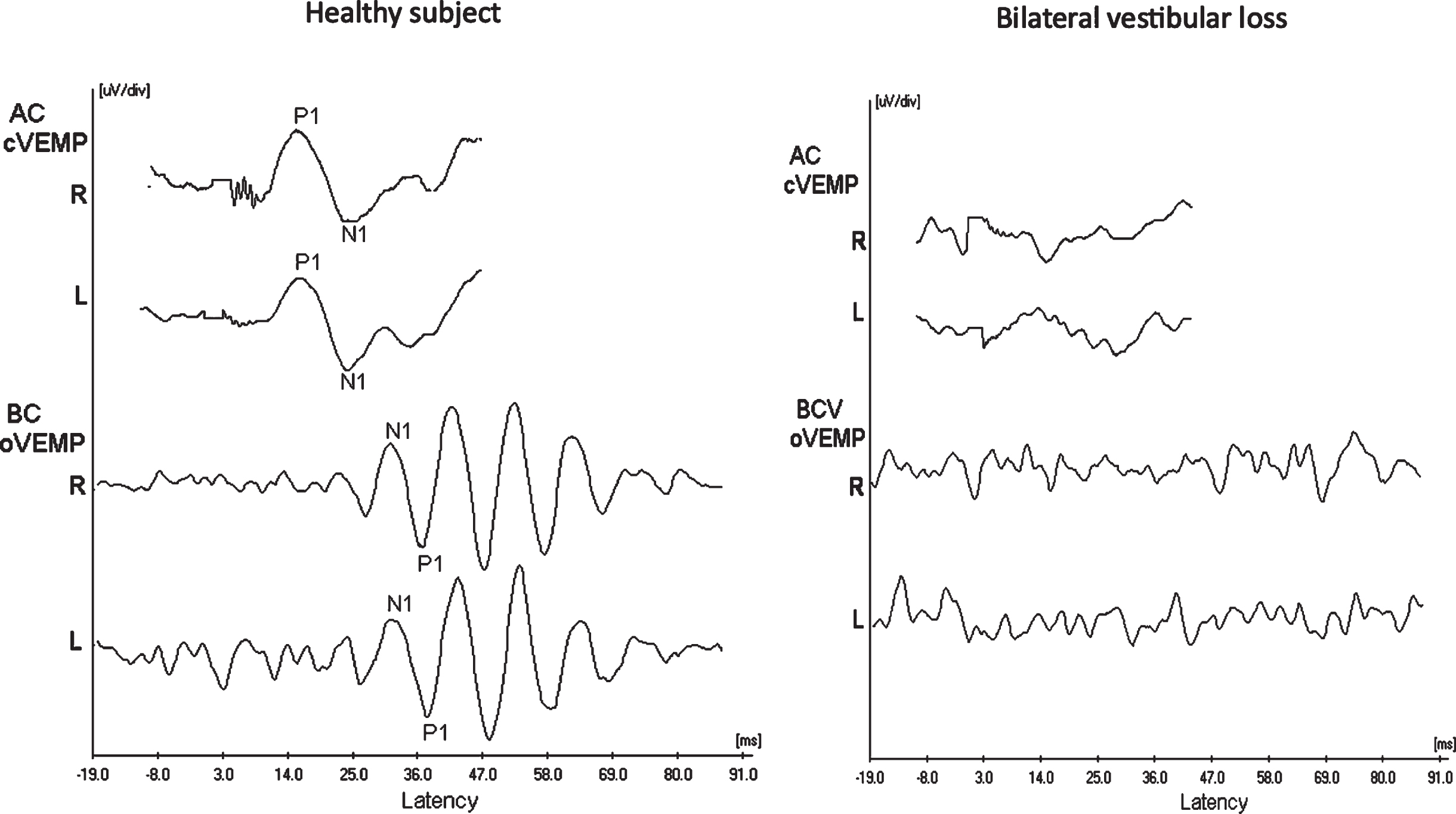
ACS cVEMP and BCV oVEMP responses obtained from a healthy subject (left panel), and a subject with bilateral vestibular loss (right panel).
The normative range for oVEMP parameters to vibration with a Mini-shaker was explored in 20 normal hearing participants (recorded from the first measurement of the two repeats). The mean of oVEMP peak to peak amplitude was 3.7±1.1 uV with 95% range [1.4 to 5.9 uV]. The mean of wave latencies (P1&N1) for oVEMP were 24.7±2.5 ms with 95% range [19.7 to 29.7 ms] and 18.14±2.4 ms with 95% range [13.4 to 22.8 ms], respectively. The oVEMP response rate was 100% in the control group and 91% in the clinical group. The two participants with absent oVEMP in the hearing-impaired group both reported double vision.
Normative data for ACS cVEMP at 500 Hz
The normative range for cVEMP parameters to ACS at intensity of 90 dB nHL was explored in normal hearing participants (recorded from the first measurement of the two repeats). The mean of cVEMP peak to peak amplitude was 104.6±68.8 uV with 95% range [32 to 241.2 uV]. The mean of wave latencies (P1&N1) for cVEMP were 16.5±1.6 ms with 95% range [13.2 to 19.7 ms] and 23.9 + 2.2 ms with 95% range [19.6 to 28.4 ms], respectively. The cVEMP response rate was 95% in the control group and 91% in the clinical group. One healthy subject and two participants with congenital bilateral profound SNHL had absent cVEMP responses in both ears, likely due to difficulties in identifying the SCM muscle as a result of thick neck tissue.
Intra-subject reliability
Table 1 presents the ICC values for oVEMP measurements (between measurement 1 and 2). It can be observed that the ICC values of the oVEMP parameters showed excellent reliability (ICC >0.75), whereas the latency of P1 indicated fair to good reliability (ICC range 0.34–0.81) in both normal hearing- and hearing-impaired participants. Table 2 presents the ICC values for cVEMP measurements. In Table 2, it can be seen that all cVEMP parameters showed excellent reliability (ICC >0.75) in both groups.
Intra-subject reliability (including Interclass correlation) of BCV oVEMP using the mini shaker for normal hearing- and hearing-impaired subjects
Intra-subject reliability (including Interclass correlation) of BCV oVEMP using the mini shaker for normal hearing- and hearing-impaired subjects
Intra-subject reliability (including Interclass correlation) of cVEMP using 500 Hz air conduction for normal hearing- and hearing-impaired subjects.
Figures 2 and 3 show scatterplots of o–and cVEMP amplitudes for normal adults and hearing-impaired subjects in measurement 1 against measurement 2, respectively.There was no statistically significant difference between the two measurements regarding c–and oVEMP amplitudes and latencies in the two study groups (p > 0.05).
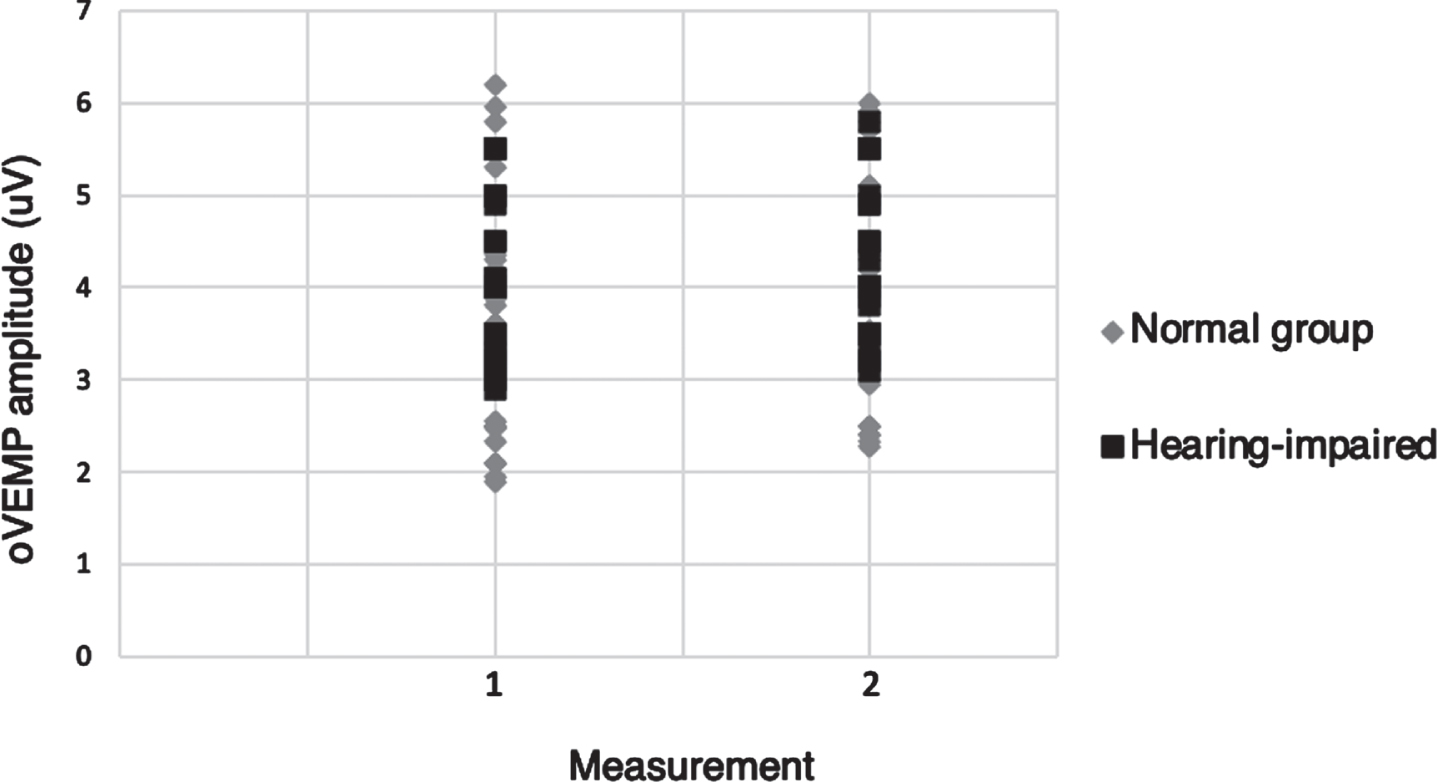
A scatterplot of oVEMP amplitude values for normal adults and hearing-impaired subjects in measurement 1 against measurement 2. There was no significant difference in oVEMP amplitudes between measurement 1 and 2 (p > 0.05) in both groups.
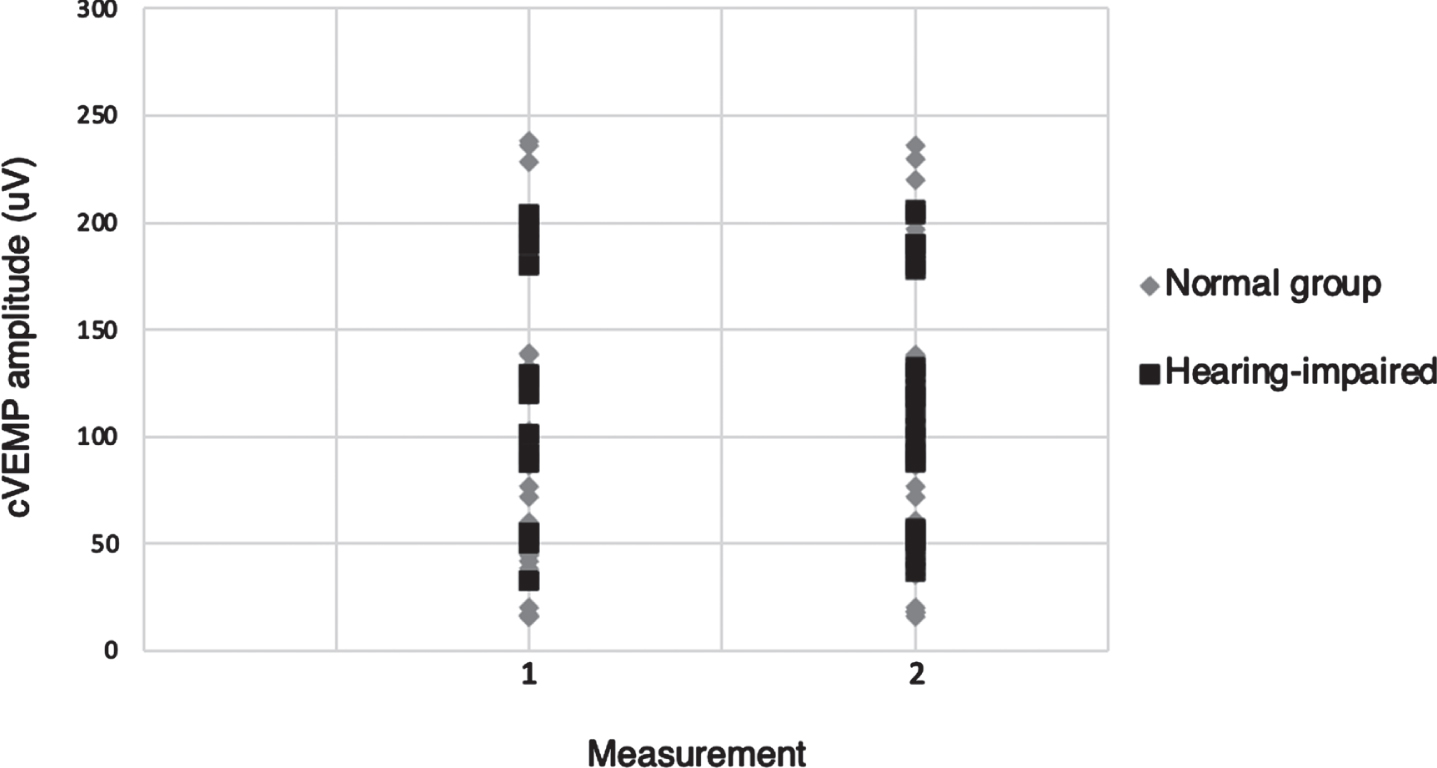
A scatterplot of cVEMP amplitude values for normal adults and hearing-impaired subjects in measurement 1 against measurement 2. There was no significant difference in cVEMP amplitudes between measurement 1 and 2 (p > 0.05) in both groups.
Table 3 presents the mean difference of VEMP results between normal and hearing-impaired participants. A Mann-Whitney U test was performed to compare ACS cVEMP and BCV oVEMP amplitudes and latencies between the two study groups. There was no statistically significant difference regarding C–and oVEMP amplitudes or latencies between the two study groups (p > 0.05).
The mean difference of VEMPs results between normal hearing (NH) and hearing-impaired subjects (HI)
The mean difference of VEMPs results between normal hearing (NH) and hearing-impaired subjects (HI)
For the normal hearing group, there was no significant effect of age on amplitude or latency for c–and oVEMP data (p > 0.05). However, there was a significant inverse correlation for the hearing-impaired participants between age and amplitude of c–and oVEMP data (i.e. amplitude reduces with age). The correlation between age and oVEMP amplitude was –0.575 (p < 0.001) while the correlation between age and cVEMP amplitude was –0.626 (p < 0.001) in hearing impaired participants. Figures 4 and 5 show scatterplots of age and amplitude of c–and oVEMP data in hearing impaired subjects.
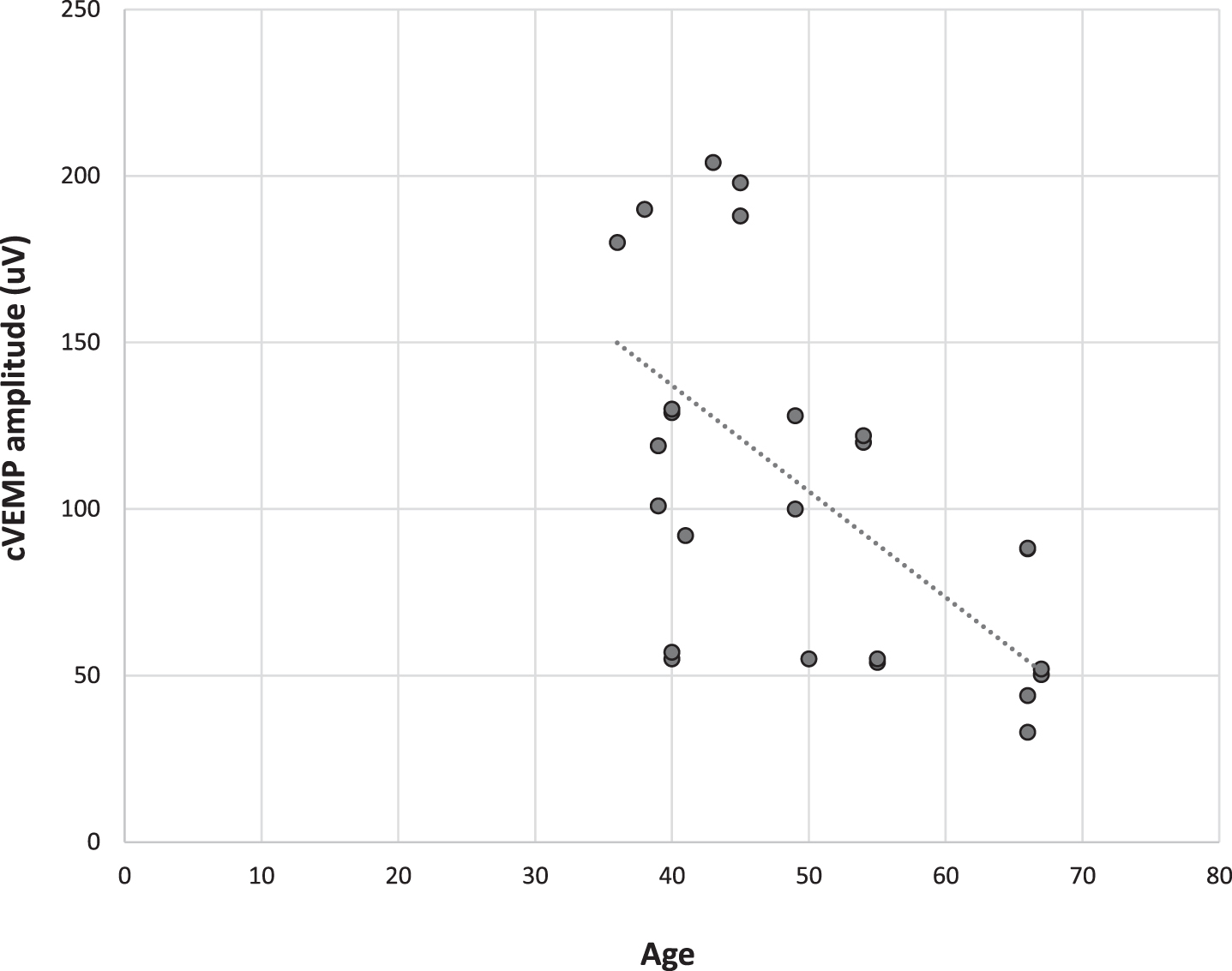
Scatterplot of age and cVEMP amplitude in hearing impaired subjects.
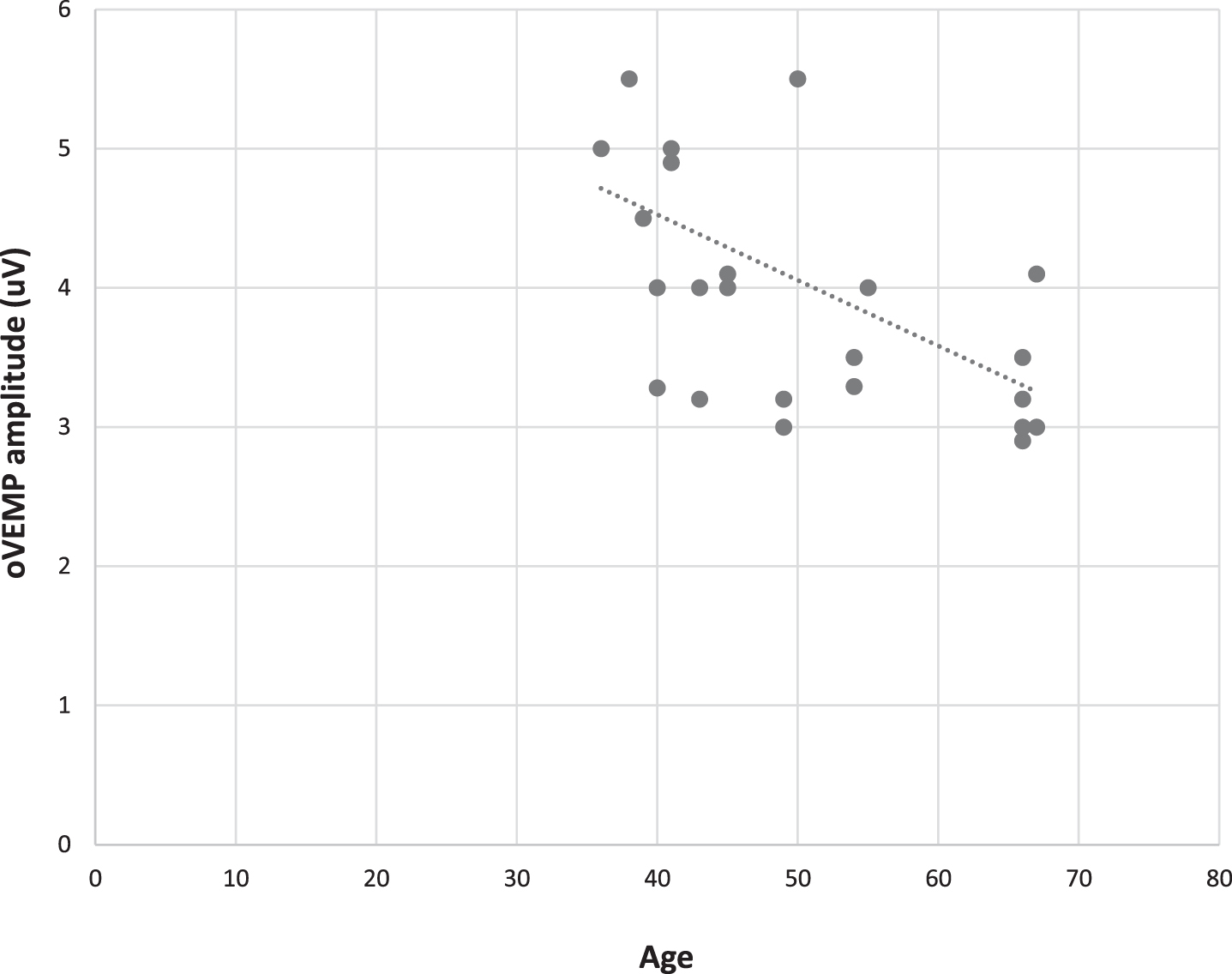
Scatterplot of age and oVEMP amplitude in hearing impaired subjects.
The aims of this study were to establish normative data of the oVEMP using vibration (Mini-shaker) and cVEMP using ACS and to estimate the agreement and the reliability of using the Mini-shaker for recording oVEMP and ACS in recording cVEMP between two repeated measurements (intra-subject reliability) for both normal hearing- and hearing-impaired participants.
VEMP Normative data
VEMP parameters that are generally used in clinical interpretation are the presence or absence of a VEMP response such as latency of P1-N1, and peak-to-peak amplitude. The results of the first measurement were not significantly different to the second measurement. As far as we are aware, no other papers have presented equivalent normative data.
Although previous studies have explored normative data using ACS (500 Hz tone-burst) evoked cVEMP in adults [2, 23], in the current work we included objective detection of cVEMP responses to eliminate the high variability that can arise using visual judgements of response presence. Significant variability between subjective estimates of VEMP threshold by experienced raters was seen in our previous study [17].
The amplitude of ACS cVEMP (104.6 uV±68.8) with target EMG level at 80–100 mV in our study was higher than other studies: Isaradisaikul et al. [9] reported peak-to-peak amplitude at 28.36±11.65 mV with target level of EMG at 50 mV. Basta et al. [2] reported peak-to-peak amplitude at 73.8±45.5 mV with target level of EMG at 50–200 mV. The p13/n23 mean latency values in our study (16.4/23.5 ms) are approximately similar to those of previous studies for adults of the same age [2, 12]. Greenwalt et al. [8] reported peak-to-peak amplitude at 315.32 mV with target level of EMG at 100–300 mV [8]. Janky and Shepard [12] reported peak-to-peak amplitude at 32.76 mV [12]. However, our normative amplitude ranges (95% ranges) are similar to those obtained by Rodriguez et al. [23] (223.17±99.18 mV with target level of 175.5 mV) in adult group, although their p13/n23 mean latencies (13.92/22.2 ms) are shorter [23].
The large discrepancy in reported cVEMP amplitude values between these studies could reflect the lack of a unified methods for monitoring SCM muscle contraction. Thus, it appears that it is important to standardize the approach for SCM muscle contraction monitoring in order to compare cVEMP normative data among studies.
Intra-subject reliability
Normal participants
Test-retest reliability of the vibration oVEMP responses were excellent for N1 latency, whereas P1 latency showed significant fair to good reliability. Moreover, significant excellent reliability was reported for peak-to-peak amplitude. Similarly, Greenwalt et al. [8] reported excellent reliability for the peak-to-peak amplitude of BCV oVEMP elicited by a Mini-shaker (ICC = 0.98) in adults [8]. However, they only used a 500 Hz tone-burst stimulus to elicit BCV oVEMP, which might not elicit utricular function. It has been proposed that the saccule is tuned to 500 Hz whereas the utricle is tuned to 100 Hz [29], in which case 500 Hz vibration responses may represent saccular function. The stimulus frequency that we used in the present study to elicit BCV oVEMP was selected based on the agreement in the literature that the 100 Hz vibration oVEMP primarily reflects utricular function. No previous studies have measured the reliability of the latency parameter for vibration oVEMP at 100 Hz using the Mini shaker.
For cVEMP to 500 Hz AC stimulation, we found excellent test-retest reliability for n23, p13 latencies and peak-to-peak amplitude. Several previous studies have similarly shown excellent reliability for p13-n23 latencies of ACS cVEMP [14], although there is some variation on this point in the literature: Kumar et al. [13] reported a fair to good reliability for p13 and excellent reliability for n23 [13]. Nguyen et al. [15]and Isaradisaikul et al. [10] reported poor reliability for p13 latency and fair to good reliability for n23 latency. Vanspauwen et al. [33] reported excellent reliability for n23 latency and fair to good reliability for p13 latency [33].
The excellent reliability for peak-to-peak amplitude of ACS cVEMP found in the current study is consistent with a number of previous studies [7, 14].
Responses from Hearing impaired participants
As VEMP is a vestibular response, we would expect similar responses in hearing impaired participants. Overall ACS cVEMP and BCV oVEMP amplitudes and latencies were not significantly different between normal, and hearing-impaired participants. For hearing impaired participants test-retest reliability of c–and oVEMP were excellent for both P1 and N2 latencies and peak-to-peak amplitudes. Surprisingly, no previous studies have measured the test-retest reliability of recording ACS cVEMP and vibration oVEMP in hearing impaired participants. More data is needed to replicate our findings. It should be noted that both the stimulus type and the filter settings used in equipment may alter latency and so should be consistent across studies to allow comparisons.
Correlation with age
In the normal hearing group, there was no significant age effect on amplitude or latency of c–and oVEMP data. A lack of age-related changes in the latencies of VEMP data in the normal hearing participants is in line with some previous results: Basta et al. [2] explored normative data for tone-burst (500 Hz) evoked cVEMP in three different age groups [2]. The p13-n23 latencies of cVEMP did not show any statistically significant differences among the three age groups. In contrast, other studies have reported age-related changes in the peak-to-peak amplitude of cVEMP data [2, 27]. We did see age-related changes in peak-to-peak amplitudes of c–and oVEMP in the hearing-impaired participants. It should be noted that the upper ages in the hearing-impaired group were higher than in the normal group and this may explain why we saw an age effect in the hearing impaired, but not the normal hearing participants.
Limitations
There were some limitations to the current study. The small sample size was not sufficient for the purpose of drawing firm conclusions about age effects on VEMP (although this was not the main aim of the study). In addition, test-retest reliability was obtained by administering VEMP testing twice in the same session without removing/replacing electrodes, so it would be helpful to explore between session variability further. As the main aim of the study was to obtain normative data, we did not test significant numbers of subjects with vestibular disorder. Further work could test the sensitivity and specificity of the proposed normative data for various vestibular disorders.
Conclusion
The present study explored the reliability of BCV oVEMP and ACS cVEMP in adults and aimed to define normative ranges for the responses. It appears that both methods are reliable in adults. Peak to peak amplitude showed excellent test-retest reliability for both ACS and BCV stimulation. ACS latency showed excellent reliability and BCV latency showed fair to good reliability. The normative values described in the current study may be helpful as a reference to identify utricular or saccular dysfunction in patients with vestibular disorders.
Financial disclosures
This study was funded by the Deanship of Scientific Research, University of Jordan.
Disclosure statement
No potential conflict of interest was reported by the authors.