
Abstract
BACKGROUND:
Research has shown that some people with neuromuscular diseases may have a lower level of education due to lower socioeconomic status and possibly compromised health literacy. In view of these data, it appears important to document their decision-making needs to ensure better support when faced with the decision to participate or not in research projects.
OBJECTIVES:
1) To document the decision-making needs of individuals with neuromuscular diseases to participate in research; 2) To explore their preferences regarding the format of knowledge translation tools related to research participation.
METHODS:
This qualitative study is based on the Ottawa Decision Support Framework. A two-step descriptive study was conducted to capture the decision-making needs of people with neuromuscular diseases related to research participation: 1) Individual semi-directed interviews (with people with neuromuscular diseases) and focus groups (with healthcare professionals); 2) Synthesis of the literature.
RESULTS:
The semi-directed interviews (n = 11), the two focus groups (n = 11) and the literature synthesis (n = 50 articles) identified information needs such as learning about ongoing research projects, scientific advances and research results, the potential benefits and risks associated with different types of research projects, and identified values surrounding research participation: helping other generations, trust, obtaining better clinical follow-up, and socialization.
CONCLUSION:
This paper provides useful recommendations to support researchers and clinicians in developing material to inform individuals with neuromuscular diseases about research participation.
Keywords
Background
Since the early 2000’s, research interest into populations with neuromuscular diseases has increased [1]. Among all the existing rare diseases, neuromuscular diseases are among the most frequent. In Canada, people with neuromuscular diseases are often referred to a neuromuscular or movement disorders university-affiliated clinic. The Saguenay-Lac-Saint-Jean university-affiliated neuromuscular clinic is one of the largest clinics in Canada who follows this population. This region has the highest prevalence of myotonic dystrophy type 1 (DM1) and autosomal recessive spastic ataxia of Charlevoix-Saguenay (ARSAC) worldwide and one of the largest cohorts of oculopharyngeal muscular dystrophy (OPMD) affected individuals. In relation to the latter, a university-affiliated research team has grown over the years and set up their research facilities within the Groupe de recherche interdisciplinaire sur les maladies neuromusculaires. As a result, an interdisciplinary research program has been ongoing since 2006 with multifaceted research activities (e.g., natural history studies, international registries, biomarkers identification, clinical trials, development and implementation of clinical practice guidelines and interventions, documentation of outcome measures metrological properties) [2]. Research has shown that some people with neuromuscular diseases may have a lower level of education due to lower socioeconomic status [3] and possibly compromised health literacy [4]. In view of these data, it appears important to document the decision-making needs of people with neuromuscular diseases to ensure better support for their decision to participate in research projects.
The objectives of this research are: 1) to document the decision-making needs of adult individuals with neuromuscular diseases in regard to participation in research activities; 2) explore preferences in format of knowledge translation tools related to their participation in research activities.
Methods
This study was based on the Ottawa Decision Support Framework [5]. The descriptive qualitative design with individual semi-directed interviews (with individuals with neuromuscular diseases) and focus groups (with healthcare professionnals) was chosen for its flexibility in the topics discussed by participants [6, 8]. For the individual interviews, the three nurse case managers at the Groupe de recherche interdisciplinaire sur les maladies neuromusculaires identified potential participants from their caseload. Participants with neuromuscular diseases were selected according to pre-established criteria to obtain a representative sample of affected individuals related to personal characteristics [9] (e.g., diagnosis of neuromuscular disease, age, sex, education) and representativeness of level of exposure to research activities (e.g., questionnaire or biopsy). Individuals who had severe impairments related to cognition or verbal communication, or an inability to consent were excluded. An initial contact was made by their nurse case manager to obtain participant consent to be contacted by the research team.
The formal recruitment was done by a trained research professional. Participants completed a sociodemographic questionnaire. For the focus groups, participants had to have more than two years work experience with neuromuscular disease. In addition, at least three types of healthcare professions had to be represented (e.g., nurse, physiotherapist, neurologist). Interviews and focus groups were approximately one-hour long. Both interview guides had the same content but language was adapted to each group’s level of literacy.
A descriptive study was conducted to define decision-making needs (information needs and values) [6]. This design helps to guide the actions that need to be taken when little information exists in a specific context [7]. The study was conducted with patient partners as co-investigators on the research team. Patient partners were trained by our research team and with the Quebec SPOR-Unit, prior to the project to become familiar with the research process, data collection and interview method. They participated in the creation of the project, in the co-animation of the interviews and in the analysis of the results. The study was carried out in two steps: 1) semi-directed individual interviews (people with neuromuscular disease) and focus groups (healthcare professionals and 2) synthesis of the literature regarding the information needs and values of people with neuromuscular disease related to their participation in research activities.
For step 1, the research team, including patient partners, determined the themes of the interview guide to cover the three main categories of the Ottawa Decision Support Framework: 1) Decisional Needs; 2) Decisional Outcomes; 3) Decision Support [5]. In this study, decisional needs included: decision type/timing, decisional conflict, clinical needs, values, lack of knowledge, support and resources. Decisional outcomes included: quality of the decision based on knowledge of the different options and the values linked to these options. Decision support included knowledge translation tools and significant persons (family, caregivers, healthcare professionals team). All interviews were recorded and transcribed verbatim in order to perform a qualitative inductive interpretive analysis [9]. The themes included: 1) Knowledge about the clinical, teaching, and research missions of the Groupe de recherche interdisciplinaire sur les maladies neuromusculaires; 2) Knowledge about the types of research projects and clinical services offered by the clinic; 3) Context of their attendance (e.g., research and care experiences); 4) Knowledge of the issues related to research participation. To help the discussion around knowledge translation tools, we provided the context for the creation of information and decision-making tools before asking questions on the content, format, and use of these tools including: 5) Information decision-making needs; 6) Research value decision-making needs; 7) Tool format. To lessen the interviewer’s influence on the participants’ point of view, the interviewer used the reformulation technique throughout the interviews. The same process was used for the two focus groups.
After data collection, the themes were entered into the NVivo 11 Software [10]. An extraction grid was constructed based on the themes to proceed to the synthesis of the literature. An in-depth reading of the content of the individual interviews and focus groups was done by three members of the research team. Then, emerging themes were classified according to the three predetermined categories of the Ottawa Decision Support Framework (Decisional Needs, Decisional Outcomes, Decision Support). Subthemes for each category were determined inductively afterwards. The themes were then reviewed by the entire research team and proposals were made regarding the emergence of new themes in relation to the Ottawa Decision Support Framework.
For step 2, the general question that guided the literature synthesis was: What are the decision-making needs of individuals with neuromuscular disease regarding information needs and values related to their participating in research activities? Results from step 1 supported the selection of the main concepts for the literature synthesis. An extraction grid was constructed by a research professional validated by the research team before data extraction. The search strategy was divided into three main concepts: 1) Person with a rare genetic disease or neuromuscular disease; 2) Participation in research; 3A) Values associated with participation in research; 3B) Information needs related to participation in research. The principal keywords were rare disease, neuromuscular diseases, patient participation, patient involvement, patient empowerment, patient preference, patient experience, patient values, information, registry, clinical trial, and biobank. This literature synthesis was conducted by one reviewer using the Cochrane method for rapid review and included: a) A comprehensive literature search in databases; b) Pre-defined inclusion and exclusion criteria (i.e., study eligibility criteria); c) Discussion about the limitations of included studies [11]. A comprehensive literature search in four databases was performed (Pubmed, CINAHL, PSYCHInfo, and EMBASE) and bibliographic references were also consulted from selected articles. To be included articles had to be written in French or English within the last 10 years. One member of the research team (the research professional that conducted the qualitative analysis) carried out a first reading of the abstracts followed by a full reading of the articles if they were included. A second person confirmed article selection (principal investigator).
The project was approved by the Comité d’éthique de la recherche du Centre intégré universitaire de santé et des services sociaux du Saguenay–Lac-Saint-Jean. The experiments were undertaken with the understanding and written consent of each subject, and the study conforms with The Code of Ethics of the World Medical Association (Declaration of Helsinki), printed in the British Medical Journal (18 July 1964).
Results
This study was conducted among eleven individuals with neuromuscular diseases, four healthcare and social services professionals, and seven research-related professionals. For participants with neuromuscular disease, four individuals had DM1, three had OPMD and four had ARSACS. Six were men and five were women. Six had completed high school. Six had already participated in research activities. Health and social service professionals had significant work experience (more than three years) with people with neuromuscular disease and represented at least three different types of professions (doctor, nurse case manager, social worker). As for research-related professionals, they had at least two years of work experience at the Groupe de recherche interdisciplinaire sur les maladies neuromusculaires, significant work experience with individuals with neuromuscular disease, and included researchers, research professionals, master or doctoral students involved in research (see Table 1).
Participant’s characteristics
Participant’s characteristics
The results are presented according to the three main concepts of the Ottawa Decision Support Framework: 1) Decisional Needs; 2) Decisional Outcomes; 3) Decision Support [5].
Decisional needs
Decisional needs, refer to different levels of information that affected individuals with the same diagnosis have about their own disease. Experience with research activities at the Groupe de recherche interdisciplinaire sur les maladies neuromusculaires is different according to the neuromuscular disease (DM1, OPMD, ARSACS). Since the early 2000 s, individuals with DM1 have been asked to participate in research activities. Many shared that the more they participated, the more comfortable they felt participating again because they have more information about ongoing research on their disease. However, a structured research program on OPMD and ARSACS has only recently been put in place. One individual said:“There are diseases where there is no research culture (...). ARSACS or OPMD, there is no research. This is new. They don’t know what to expect. It is a culture that is not rooted, compared to other diseases, such as myotonic dystrophy (...). They have been doing intensive research with them since 2002.” (Group2Research)
Decisional outcomes
Decisional outcomes refer to the values associated with research participation for all affected individuals. All participants strongly emphasized the desire to help others with the disease. For example, many of them talked about helping future generations and being part of the solution (feeling of pride), and not part of the problem because of the genes they passed on to their children (feeling of guilt). Many wanted to give everything to research (e.g., compensation, donation, access to their medical files, test results). Some expressed an interest in participating in projects that address all neuromuscular disease, while others wished to participate only in projects that address their own disease.
“To advance research. Yes, they found the gene, but it has to continue. Maybe it’s too late for us, but, for the new ones, it will be convenient to know that they can find a pill or medication.” (P-ARSACS)
In terms of decision-making needs related to information needs, some themes need further exploration, including knowledge of scientific advances related to their disease and the need to receive detailed information about their participation in a research project when the level of risk is higher (for example, muscle biopsy).
Information needs differed, namely the need to know their own individual results from their participation in research activities (progression, or in comparison to normative data), the amount of information and level of detail.
“In my case, I don’t know where the research is at, either. These are research programs. Researchers have results; they sometimes try to tell us how their results work, but it’s not clear.” (P-DM1)
Decision support
Regarding values associated with the decision to participate in research or not, similarities were found, including the importance of having a trust-based relationship with the Groupe de recherche interdisciplinaire sur les maladies neuromusculaires healthcare professionals. This trusting relationship helps them feel free to ask questions. They also feel more comfortable knocking on the professional’s door when they are welcoming and interested in their wellbeing. The trust between individuals with neuromuscular disease and research professionals, combined with strong collaboration between neuromuscular clinical healthcare professionals, encourages recruitment for research.
“The feeling of relation and belonging is very strong (...). They feel that we need them. They feel appreciated. We have always taken care of our patients (...). We call them. They call us (...). We have developed a relationship of trust. That’s why you don’t have any difficulty recruiting. There is continuity.” (Group 1 Clinicians)
For information comprehension and retention, participants with DM1 expressed the need to have the same information repeated across many knowledge translation tools and more graphical representation of the concepts associated with the different research activities. Indeed, specific projects are often not clear to them, and they appreciate practical examples to which they can relate to, to get the essence of their participation and goals of the research activities proposed to them. Often, research projects on physical exercise or nutrition are more tangible for them. Individuals with OPMD expressed the need for more specific details in the information provided to them. Various media were discussed for the creation of knowledge translation tools to help the decision-making process. No consensus was reached on any, and media preferences included iPads, videos, websites including social networks like Facebook, posters or leaflets.
“There would be an advertisement that would be interesting to do (or) a DVD that would (play in) the waiting room. ‘You have myotonic dystrophy. Do you know that there is such a thing? (We are having) a study.’ The papers, I don’t look at it. But I keep them all in an envelope. If I have a problem, I’ll be able to look at them. But I don’t read them; I trust you.” (P-DM1)
Step 2: Synthesis of the literature
As the studies reviewed addressed different research activities, presentation of the results was divided into the four most common research activities in the area of neuromuscular disease: 1) registries (n = 8); 2) clinical trials (n = 17); 3) biobanks (n = 13) and 4) academic research projects (n = 12) (see Fig. 1 and Table 2).
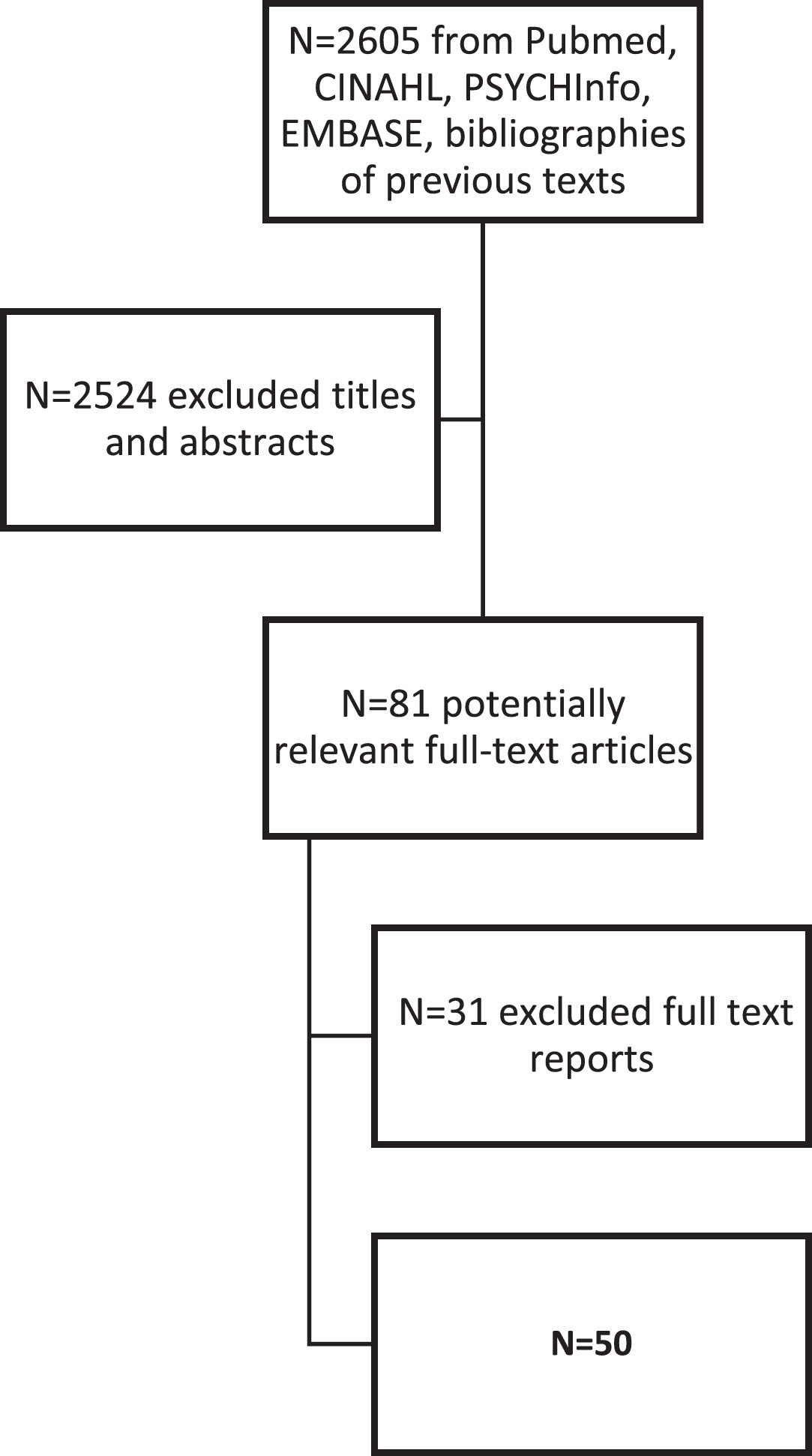
Results of literature review.
Results details of synthesis of the literature (n = 50)
The selected articles focused mainly on the importance of the active involvement of individuals with rare diseases in research (e.g., being more than a patient, becoming a partner by making their voices heard in decision-making) [12–14]. The main reasons for agreeing to participate in a registry study are to help family members, to help other individuals with rare diseases to improve their own health condition, or to improve care and services [12, 15]. Trust in the registries and healthcare professionals involved must be developed with individuals with rare diseases and their families, by actively engaging them in research and information sharing (e.g., ongoing studies and opportunities to participate, showing gratitude for their input) [14, 17]. Their data in the registries should be kept confidential [16, 18]. These data should only be available to certain entities such as their healthcare team and researchers but not private insurance companies [16] (see Table 2).
Clinical trials
The topics covered in the selected articles on clinical trials focused mainly on individual benefits for trial participants [19–32]. For these people, their participation in research on their disease is the only option to improve their condition, sometimes even their last possible choice [19–21, 31]. Participating in a clinical trial allowed them to obtain additional healthcare services (especially for those without access to insurance) [19–28, 32]. It also seemed very important to them that their participation in studies would benefit their loved ones (e.g., future generations in their families) [19–21, 32]. Alternatively, the higher the risk of clinical trials (e.g., side effects), the more reluctant they were to participate [19, 32]. They did not wish to be part of a control group [21, 32]. According to them, therapeutic trials sometimes involved invasive procedures (e.g., biopsy) [19] which can cause pain [23] or can deteriorate their health for multiple reasons (e.g., discontinuation of current medication, drug interactions, decreased quality of care, increased testing) [21, 32–34]. This is the reason why their relationship with professionals and their trust in them, are very important [21, 35]. To facilitate comprehension, they suggest structuring the information provided to them (e.g., graphics and images, underscoring, highlighting, bolding, and underlining text, using various colours, sections, and text sizes, as well as Braille, headers, first-impression appeal, meeting agendas, checklists) [27]. Finally, the preferred methods for providing information were through face-to-face meetings (allowing time for discussion and questions) [23, 34], websites and social media [28, 34], pamphlets and letters [25, 34], groups [34], conferences [29], videos [28], and phone calls [34] (see Table 2).
Biobanks
Reasons for participating in research centered mainly on helping others, including future generations [36–43], advancing research knowledge to improve services [36, 41–44] and helping oneself [36, 40–42]. Individuals with rare diseases interviewed in these studies also emphasized the importance of establishing a trusting relationship with those involved in the creation and application of biobanks with knowledge of their credibility and sources [38–40, 45]. According to them, biobanks can contribute to the common good by reducing health costs [37–40, 45]. However, they pointed out that their data must remain confidential [42, 46]. Others highlighted the desire to obtain information on the risks associated with their participation in a biobank when collecting biological materials (e.g., injuries, pain) [38, 47], the benefits [36, 46], and the results of their participation [42, 47]. Some wanted to know if there are rules for sharing and accessing biological materials and other data [38, 48], including what are the penalties if researchers do not respect confidentiality [38, 46]. They would prefer being able to decide who can and cannot access their data [38, 46]. In terms of how to provide information, the studies emphasized that their participants preferred that the content be made accessible to the general public according to their literacy and educational level [37, 46]. Repeating information and maintaining constant communication with research professionals are some of the proposed strategies [40, 46]. Many emphasized the importance of having access to a person who is comfortable with providing information [44] and who is also able to answer their questions [37, 48] (see Table 2).
Academic research projects
The themes covered in the collected texts on academic research (e.g., qualitative with interviews, longitudinal) regarding research values important to individuals with rare diseases focused mainly on the trustworthiness of the information sources [49–54]. The willingness of researchers to give back to individuals with rare diseases [50], to express their gratitude to them [54, 55], to not being cold and distant [55], to promote solidarity (e.g., sharing information) in order to avoid competitiveness (e.g., retention of research results) [50], in developing a research culture accessible for all [55], in participants not feeling used for career advancement purposes by researchers [55] and confidentiality [50, 56], are winning strategies, in their opinion, to help build trust among individuals with rare diseases. Participating in research is a way for individuals with rare diseases to obtain better treatment (e.g., more treatments, detection before deterioration, prevention, improvement of quality of life) and to develop new knowledge [51–53]. Regarding the information that individuals with rare diseases want to receive, the main topic discussed was benefits (e.g., reducing feelings of guilt, helping, socializing) [49–51, 57–58]. They want to receive the results of the study [50, 59]. They also want to receive information on risks before accepting to participate (e.g., anxiety about the results that may affect them regarding their disabilities) [49, 51], eligibility criteria [49, 54], goals and steps [51] and no impact quitting options [51]. Regarding how information is provided, studies emphasized that individuals with rare diseases preferred to receive information face-to-face [50, 59]. When discussing other means of disseminating information, several mentioned technology-based media (e.g., email, Skype, websites) [52–54, 59], while some mentioned more traditional media (e.g., flyers, poster) [51, 59] (see Table 2).
Discussion
This study explored the decision-making needs (information and values) of individuals with neuromuscular disease when deciding to participate in research activities. Data revealed the following observations: first, they need to know more about research opportunities. Also, helping other generations with neuromuscular disease is an important part of the decision to participate in research. Finally, the creation of knowledge transfer tools to support the decision-making process on patient’s engagement in a research project is also an important part of the decision to participate in research.
Regarding decision-making needs, several individuals with neuromuscular diseases highlighted the need to know more about opportunities to participate in ongoing projects and about scientific advances in the area of their disease. Individuals expressed a desire to know more about the importance of research participation to advance knowledge (e.g., scientific, clinical), and the potential benefits for themselves and other individuals with the same disease. As presented in the results, the development of research on DM1 is more advanced than on OPMD and ARSACS. Some patients have already participated in research projects. This is why it seems important to develop knowledge transfer tools, specific for each disease in relation to scientific advances. As Farha et al. (2020) emphasize, knowledge can influence the willingness of patients to participate in research. Lavoie et al. (2020) add that DM1 patients can choose the knowledge transfer tool that matches their literacy level. It therefore seems important to focus on the vulgarization of all research documents in order to promote recruitment.
Regarding decisional outcomes, all patients highlighted the importance of helping other generations. Contributing to scientific progress and improved practices were themes promoted. Being part of the solution, not the problem, is an important element for individuals because many of them live with the guilt of being a carrier of an inherited disease. Helping others was a theme observed in recent literature [61, 62]. This aspect is important to highlight, because it can strongly influence a person’s decision to participate in a research project. Given that there is no cure for DM1, OPMD or ARSACS and very few ongoing clinical trials, a person’s participation in research may have more of an impact for the next generations than for themselves.
When creating knowledge transfer tools, it is important to take into account the specific needs of individuals with neuromuscular disease to support information retention using several methods, including repetition. They also suggested using several reminders (e.g., diary, calendar, phone call by a professional they know and trust). Recent studies highlighted the importance of involving healthcare professionals who are close to patients in knowledge transfer to build trust [61–63]. A trusting relationshipis very important and the strength of the Saguenay-Lac-Saint-Jean university-affiliated neuromuscular clinic is that the team (e.g., nurses, doctors, physiotherapists, social workers) ensures patient monitoring from birth to death. This contributes to the maturity of the relationship which promotes recruitment and participation in research projects (64). For example, some authors recommend highlighting items on documents that seem important to patients (65). To encourage dissemination, they proposed to involve individuals with neuromuscular disease in the creation of knowledge translation tools. Moreover, as Lavoie et al. (2020) underline, they observed that diversity of format makes it possible to respond to patient preference style of experiential learning. For the transmission of information in digital form, the study by Coathup et al. (2016) underlines that DM1 patients complain about not receiving enough medical information and they would be ready to receive more through digital tools. Especially videos on IPAD for patients with compromised health literacy to avoid abstraction [5].
Conclusions
One of this study’s major strengths is the involvement of patient partners in documenting reviews, co-leading interviews and in data analysis to better target priority areas to be addressed. In addition, focus groups with professionals from the research community and the healthcare services allowed to expand the interdisciplinary expertise involved in the project. A limitation of the study is related to the sampling procedure that could lead to an ascertainment bias: 1) limited number of affected people recruited; 2) few rare disorders covered; 3) all followed at a specialty center. The literature review resulted in a significant amount of information collected regarding the needs of individuals with neuromuscular diseases related to various research activities (e.g., registries, clinical trials, biobanks). The literature review found that few articles take into account the concept of shared decision-making in research for individuals with neuromuscular diseases. Future studies could examine the impact of shared decision-making on research participation for individuals with neuromuscular diseases and their families. This paper provides useful recommendations to support researchers and clinicians in the development of material to inform individuals with neuromuscular diseases about research participation. Future studies could document the effectiveness of these recommendations to improve patients’ understanding of research activities and support their decision-making process.
Footnotes
Acknowledgments
We would like to thank our collaborators: three patient partners (Marc Tremblay, Michel Boivin, André Girard), two nurse clinicians (Aline Larouche and Nancy Bouchard), two students (Samar Muslemani and Émilie Godin), the coordinator of the Physical Disability Program (Véronique Tremblay), the university assistant (Isabelle Boulianne) and the research coordinator (Julie Létourneau). Your investment and your reflections brought the analysis of this study to a higher level. We also thank all the participants who shared their time and experiential knowledge. Finally, we thank the Fondation de Ma Vie for the financial support that allowed us to accomplish this study.
Authors’ contributions
Véronique Gauthier: Conception, Methodology, Analysis of data, Preparation of the manuscript, Writing, Reviewing and Editing
Marie-Eve Poitras: Conception, Methodology, Analysis of data, Writing-Reviewing
Mélissa Lavoie: Conception, Writing-Reviewing
Benjamin Gallais: Conception, Writing-Reviewing
Samar Muslemani: Conception, Writing-Reviewing
Michel Boivin: Conception, Analysis of data, Writing-Reviewing
Marc Tremblay: Conception, Analysis of data, Writing-Reviewing
Cynthia Gagnon: Conception, Methodology, Analysis of data, Supervision, Writing, Reviewing and Editing
Conflict of interest
The authors declare that they have no conflict of interest.