
Abstract
BACKGROUND:
There is a paucity of knowledge regarding neuroendocrine neoplasms (NEN) in patients with HIV infection.
OBJECTIVE:
To explore the incidence, characteristics and treatment outcomes of NEN in HIV-positive individuals.
METHODS:
This is a single-center, descriptive cohort study. Patients with HIV and biopsy-confirmed NEN were identified from our data registry. Data were collected retrospectively from medical records. Progression-free and overall survival (OS) were estimated using the Kaplan-Meier method.
RESULTS:
Nineteen HIV-positive patients with neuroendocrine tumors (NET) (n = 14), neuroendocrine carcinomas (NEC) (n = 2) or Merkel cell carcinoma (MCC) (n = 3) were included (median age at NEN diagnosis, 53 years). In 15 (79%) patients, HIV diagnosis preceded NEN diagnosis by a median of 11 years and 14 were receiving antiretroviral therapy (ART). Of those with data available, 75% had a viral load < 50 copies/ml and mean CD4 771 cells/mm3. The median OS in the NEC/MCC cohort was 8 months (range 5–29). The median OS in the NET cohort was not reached but based on the 25th centile, 75% of patients are expected to survive for at least 57 months. Treatment outcomes will be described.
CONCLUSIONS:
Within the limits of a small descriptive cohort study, we found no evidence in the era of ART that patients with HIV and NEN are diagnosed at a younger age, nor have a poorer prognosis compared with the wider NEN population. Thus, they should receive maximal NEN therapies to support best outcomes.
Keywords
Introduction
Neuroendocrine neoplasms (NEN) are rare tumors with an incidence of 2.5–5 cases per 100,000 persons per year [1, 2]. However, the incidence of NEN is increasing, and given their long survival durations, the prevalence of NEN has now eclipsed gastric, pancreatic, esophageal and hepatobiliary adenocarcinomas [1, 3]. Given the wide distribution of neuroendocrine cells, tumors may originate in almost any organ but are commonest in the gastroenteropancreatic (GEP) system (57%) and lung (27%) [3].
The histological classification of NEN is dependent on their site of origin. For the commonest subtype, GEP NEN, the WHO 2010 classification [4] divides them into 3 grades as determined by a proliferation-based grading index of Ki67 and/or mitotic count/10 high-power fields. Grade 1 (G1) tumors are well-differentiated, with < 2 mitosis per 10 high power fields and Ki67 < 3%. Grade 2 (G2) are well-differentiated with 2–20 mitosis per 10 high power fields and/or a Ki67 of 3–20%. Grade 3 (G3) contains both well-differentiated neuroendocrine tumors (NETs) and poorly differentiated neuroendocrine carcinomas (NECs) with > 20 mitoses per 10 high power fields and/or Ki67 > 20%. The 2019 WHO classification [5] has recently been adopted for G3 gastroenteropancreatic NEN which differentiates between G3 well-differentiated NET and G3 poorly differentiated NEC based on distinct differences in prognosis.
Given the biological heterogeneity of NEN, management is complex and a multidisciplinary approach in a center with NEN expertise is critical. For well-differentiated NET, the mainstay of treatment where possible is surgery with curative intent, including metastasectomy for oligometastatic disease. Hepatic-directed therapies, such as transarterial embolization, are also frequently used depending on site, size and number of metastases. Systemic treatment options most commonly include somatostatin analogues in the first-line setting for both anti-tumor effect and control of hormonal syndromes [6, 7]. Other systemic therapies for diffuse disease include molecular targeted therapy such as sunitinib [8] and everolimus [9, 10], peptide receptor radionuclide therapy (PRRT) [11] as well as cytotoxic chemotherapy for more aggressive tumors [12]. Treatment choice is influenced by a number of factors including primary site of origin, the functional status of the tumor, distribution and volume of disease, tumor morphology and histological grade, and patient factors such as performance status and renal function.
HIV infection and cancer
A strong association has been described between HIV infection and a number of virally-mediated malignancies designated AIDS-defining cancers, namely, Kaposi’s sarcoma, non-Hodgkin’s lymphoma and cervical cancer. The widespread adoption of antiretroviral therapy (ART) has dramatically altered the incidence and prognosis of AIDS-defining cancers although, due to increased life expectancy, a significant increase in non-AIDS defining cancers, such as lung cancer and head and neck cancer, has been reported which now cause greater morbidity and mortality [13–15].
HIV infection and neuroendocrine neoplasms
There is a well-defined association between HIV infection and Merkel cell carcinoma (MCC) [16]. MCC is a rare skin cancer which arises in cutaneous neural crest cells and occurs more frequently after organ transplantation or B-cell malignancy [17]. It is frequently associated with Merkel cell polyomavirus infection, a common viral infection without long-term sequelae in the general population, but associated with increased pathogenic potential in the immunocompromised [18, 19]. In a cohort of 309,365 individuals with acquired immunodeficiency syndrome (AIDS) linked to cancer registries, six cases were identified, corresponding to a relative risk of 13.4 (95% CI 4.9–29.1) compared to the general population [20].
With respect to immunodeficiency and NETs, an association between X-linked hyper-IgM syndrome (XHIGM) and NET has been described but is not seen in other types of primary immune deficiency, despite an association observed with other gastrointestinal neoplasms. Nicolaides et al. [21] described 10 patients with XHIGM and NETs, suggesting an occurrence rate of 0.02–0.06% i.e. a very rare phenomenon compared to other genetic conditions such as multiple endocrine neoplasia type 1, where the risk of developing GEP NEN is 30–70% [22].
There is little in the literature describing NEN in patients with HIV infection. Nicolaides et al. [21] described 12 HIV infected individuals who developed NET (n = 5), NEC (n = 6) and MCC (n = 1). Compared to the general NEN population, they were younger at the time of NEN diagnosis, between the 2nd and 4th decade of life; however, only half of patients were receiving ART. Three cases of rectal small cell carcinoma, a carcinoid tumor of the appendix and a NEC of the tail of the pancreas, were described. A further case series included four patients with GEP NEN ranging from well-differentiated NET to two aggressive metastatic NECs, and one patient had an intra-parotid lymph node MCC [23].
We describe the largest and most comprehensive cohort thus far reported in the literature of 19 HIV positive patients treated at a single institution and certified European NET Centre of Excellence; the clinical manifestations, treatment challenges and outcomes will be described.
Methods
This descriptive cohort study included all HIV positive patients with biopsy-confirmed NET, NEC or MCC identified from the Royal Free Hospital NET registry and hospital records spanning the years January 1999–June 2020. Data were collected retrospectively from medical records and comprised patient demographics, date of diagnosis of HIV and date of diagnosis of NEN, HIV status (CD4 count and HIV viral load at time of NEN diagnosis, CD4 nadir), grade and stage of NEN, co-morbidities, radiological findings, cancer treatment received, modification of ART in preparation for cancer treatment and patient outcomes. Medical records were evaluated until date of death.
Given the anticipated small sample size and consequently limited statistical power, the intent of our analysis was descriptive and hypothesis generating. Continuous variables were expressed as median (range) or mean (standard deviation) and categorical variables as frequencies (percentages). Progression-free survival (PFS) and overall survival (OS) were estimated using the Kaplan-Meier method and comparison of curves was performed using the log-rank test. PFS was calculated from date of commencement of NEN therapy to date of first radiological progression or NEN-related death. Subjects without disease progression or death were censored at the date of last imaging assessment. OS was calculated from date of NEN histological diagnosis to date of NEN-related death. Subjects who remained alive were censored at last date of contact. Patients were followed for disease progression and survival every 3–6 months. Tumour assessment was performed with contrast-enhanced CT or MRI at baseline and then every 3–6 months. One patient was diagnosed with a G1 NET, one month before succumbing to metastatic esophageal cancer and was censored at date of death. One patient moved abroad after commencing third line systemic therapy; however the date of death was recorded. Statistical analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA) and Microsoft Excel, version 16.43. For all analyses, a two-sided p value < 0.05 was considered to be statistically significant.
Results
Patient population
Nineteen HIV positive patients with biopsy-confirmed NET (n = 14), NEC (n = 2) or MCC (n = 3) were included (Table 1). Sixteen (84%) patients were male with a median age at NEN diagnosis of 53 years (range 24–68).
Patient characteristics at time of NEN diagnosis (n = 19)
Patient characteristics at time of NEN diagnosis (n = 19)
NR not reported, NA not available, WD well-differentiated, PD poorly differentiated, DIPNECH diffuse idiopathic pulmonary neuroendocrine cell hyperplasia, CMV cytomegalovirus, PCP pneumocystis jirovecii pneumonia, T2DM type 2 diabetes mellitus, IHD ischemic heart disease, HTN hypertension, HBV hepatitis B, HCV hepatitis C, CIN1 cervical intraepithelial neoplasia grade 1, HPV human papilloma virus, SCC squamous cell carcinoma, NASH non-alcoholic steatohepatitis, COPD chronic obstructive pulmonary disease, ITP idiopathic thrombocytopenic purpura, PE pulmonary embolus, OSA obstructive sleep apnea. *Biopsy on peritoneal disease at diagnosis was consistent with G1 disease; biopsy of liver metastasis 2 years later showed high G2 disease.
Fourteen patients (74%) had a well-differentiated NET; the commonest primary tumor site was gastroenteropancreatic (3 midgut, 3 pancreas and 1 rectal), followed by five bronchial, one head and neck paraganglioma associated with a germline SDHA mutation and one unknown primary. Most well-differentiated NET (9/14, 64%) had low proliferative indices (Ki67 < 3%) and presented with localized or locoregional disease. The remaining five patients were all grade 2 (Ki67 3–20%); four of these patients presented with distant metastatic disease, one patient had a localized pancreatic primary which was successfully resected. One patient had a peritoneal biopsy at diagnosis consistent with a G1 NET of midgut origin, but a liver biopsy performed two years later in view of more aggressive disease behavior confirmed a G2 NET (Ki67 18%). Two patients with high volume liver metastases (primary midgut and primary lung, respectively) suffered from severe carcinoid syndrome.
Five patients (26%) had more aggressive G3 histology comprising two patients with poorly differentiated NEC (lung primary with Ki67 60%, and unknown primary with Ki67 30%) and three with MCC, all presenting with metastatic disease (Table 1).
Fifteen (79%) patients were diagnosed with HIV prior to their NEN diagnosis by a median of 11 years (range 8–28): two patients had a diagnosis of NEN and HIV simultaneously and two had a diagnosis of NET prior to the HIV diagnosis, but may have been living with undiagnosed HIV at the time.
At time of NEN diagnosis the majority of patients with known HIV were receiving ART (14/15; 93%); one patient was non-compliant with therapy. Viral load and CD4 count were available for 12 patients within six months of their NEN diagnosis; nine of these patients had an undetectable viral load and mean CD4 count of 771 cells/mm3 (Table 1). Three patients had advanced HIV at the time of their NEN diagnosis: one patient with a poorly differentiated metastatic NEC of unknown primary had an HIV viral load of 261,804 copies/ml and CD4 count 150 cells/mm3 and was non-compliant with ART; one patient had an incidental finding of an 8 mm low-grade bronchial NET (typical carcinoid) at the time of presenting with advanced HIV (viral load 691,831 copies/ml, CD4 count 10 cells/mm3) and multiple sequelae (late latent syphilis, esophageal candida, CMV viremia, Pneumocystis jirovecii pneumonia (PCP)) and another patient had an incidental finding of a G1 tail of pancreas NET after presenting with advanced HIV (viral load 91,453 copies/ml, CD4 count 30 cells/mm3) and cerebral tuberculosis. Three other patients had a history of an AIDS-defining illness prior to NEN diagnosis: two with Kaposi’s sarcoma and one with tuberculosis.
Non-AIDS defining cancers were seen in four patients comprising head and neck cancer, non-small cell lung cancer, prostate cancer, locally advanced anal squamous cell carcinoma, locally advanced squamous cell carcinoma of the skin and metastatic squamous cell carcinoma of the esophagus.
All patients with known HIV diagnoses were receiving ART at the time of commencement of systemic therapy for their NEN.
NEN treatment outcomes and prognosis
Bronchial NET
In the well-differentiated NET cohort (Table 2), patients with bronchial NETs (n = 5) presented with localized or locoregional disease and low-grade histopathology (typical carcinoid), and four proceeded to pulmonary lobectomy; all were alive after a median of 73 months (range 6–217) follow-up. Two patients developed distant recurrence. One patient with a solitary positive lymph node at the time of lobectomy (TNM stage [24] T2a N1 M0 R0) developed multiple sub-centimeter liver lesions eight years later, suspicious for NET metastases (arterially-enhancing on MRI and avid on 68Gallium DOTATATE PET). This patient was commenced on systemic therapy with long-acting somatostatin analogues and the liver lesions remain stable ten years to date. A second patient who had a pulmonary lobectomy but without lymph node clearance (TNM not available) developed high volume liver and bone metastases 5.3 years later complicated by carcinoid syndrome. He was treated with long-acting somatostatin analogues and peptide receptor radionuclide therapy (PRRT) with 177Lutetium DOTA-Octreotate and achieved a sustained partial objective response and amelioration of his syndrome. Both patients had an undetectable HIV viral load at time of NET recurrence.
Therapy received and outcomes in the well-differentiated NET cohort (n = 14)
Therapy received and outcomes in the well-differentiated NET cohort (n = 14)
*Ki67 not reported. SSTA somatostatin analogue. PFS progression free survival. RFA radiofrequency ablation. FCarboStrep 5-fluorouracil/carboplatin/streptozocin. FCiSt 5-fluorouracil/cisplatin/streptozocin. DIPNECH diffuse idiopathic pulmonary neuroendocrine cell hyperplasia. PRRT peptide receptor radionuclide therapy. mo months. AKI acute kidney injury.
Three patients had midgut primaries. Two of these patients had relatively small volume metastatic disease and underwent surgical resection of the primary tumor followed by systemic therapy with somatostatin analogues in one case (stable disease after seven years on treatment) and radiofrequency ablation to treat a residual solitary liver metastasis in the other (no evidence of recurrence after seven months follow-up). The third case progressed despite first-line somatostatin analogue therapy and behaved more aggressively (Ki67 2% on first biopsy and 18% on second biopsy). This patient had somatostatin receptor-expressing disease and also suffered severe carcinoid syndrome; he was treated with PRRT with 177Lutetium DOTA-Octreotate alongside somatostatin analogues. Disease progression occurred promptly after the fourth cycle and thus chemotherapy with 5-fluorouracil (5FU), carboplatin and streptozocin was commenced which was well tolerated until the fifth and sixth cycle when a drop in CD4 count occurred. He was commenced on PCP prophylaxis and his antiretroviral therapy elvitegravir/cobicistat/emtricitabine/tenofovir was switched to dolutegravir/emtricitabine/tenofovir. He proceeded to fourth-line therapy with 5FU/irinotecan but experienced life-threatening diarrhea complicated by acute kidney injury (creatinine 426 umol/L; eGFR <15 ml/min) six days following the first cycle, which he survived. Emtricitabine/tenofovir was switched to lamivudine in view of the kidney injury, and chemotherapy was discontinued. The patient died due to progressive metastatic disease 7 months later.
Pancreatic NET
Of the three patients with well-differentiated pancreatic NET, one patient had localized disease and proceeded to a Whipple’s resection (T3 N0 M0, Ki67 8%) with no evidence of disease recurrence after 24 months follow-up. The second patient had a localized 10×11 cm tail of pancreas NET (Ki67 2%) discovered incidentally but was lost to follow-up for 13 years; a follow-up CT chest, abdomen and pelvis surprisingly showed stable appearances. The third patient had metastatic disease (Ki67 3%) and completed three lines of systemic therapy including somatostatin analogues, sunitinib and 5FU/cisplatin/streptozocin chemotherapy before eventually succumbing to progressive metastatic disease 57 months after diagnosis.
Poorly differentiated NEC and MCC
Four out of five patients with poorly differentiated NEC or MCC received first-line therapy with platinum-based chemotherapy regimens with a median PFS of 5.5 months (range 2–11) (Table 3).
Therapy received and outcomes in the poorly differentiated NEC and MCC cohort (n = 5)
Therapy received and outcomes in the poorly differentiated NEC and MCC cohort (n = 5)
LCNEC large cell neuroendocrine carcinoma. FCiSt 5-fluorouracil/cisplatin/streptozocin. FOLFIRI 5-fluorouracil/folinic acid/irinotecan. CAV cyclophosphamide/doxorubicin/vincristine. NR not reported.
Recently, immunotherapy (avelumab, pembrolizumab, nivolumab) has become the new standard of care for patients with metastatic MCC based on several clinical trials [25]. Two patients in our cohort with metastatic MCC and well-controlled HIV received avelumab, however, both did poorly: one patient with high-volume disease treated in the first-line setting died 26 days after cycle 1 due to progressive disease and the other patient treated in the second-line setting after chemotherapy had a PFS of only 3 months (Table 3). One patient with metastatic large cell NEC of the lung received pembrolizumab in the third-line setting but died 5 months after its commencement. There were no immune-related toxic effects. Changes in viral load or CD4 count status were unfortunately not documented.
The median follow-up for patients still alive was 47 months (range 6–217) after NEN diagnosis. Of the entire cohort (n = 19), eight patients had died. Five of these patients had poorly differentiated NEC or MCC, one patient had a metastatic G2 midgut NET and died 51 months after diagnosis, one patient had a metastatic G2 pancreatic NET and died 57 months after diagnosis, and one patient with a G1 NET of unknown primary died from a synchronous esophageal squamous cell carcinoma 1 month after NET diagnosis. The median overall survival in the NEC/MCC cohort was 8 months (range 5–29). The median overall survival in the well-differentiated NET cohort has not been reached but, based on the 25th centile, 75% of patients are expected to survive for at least 57 months (Fig. 1).
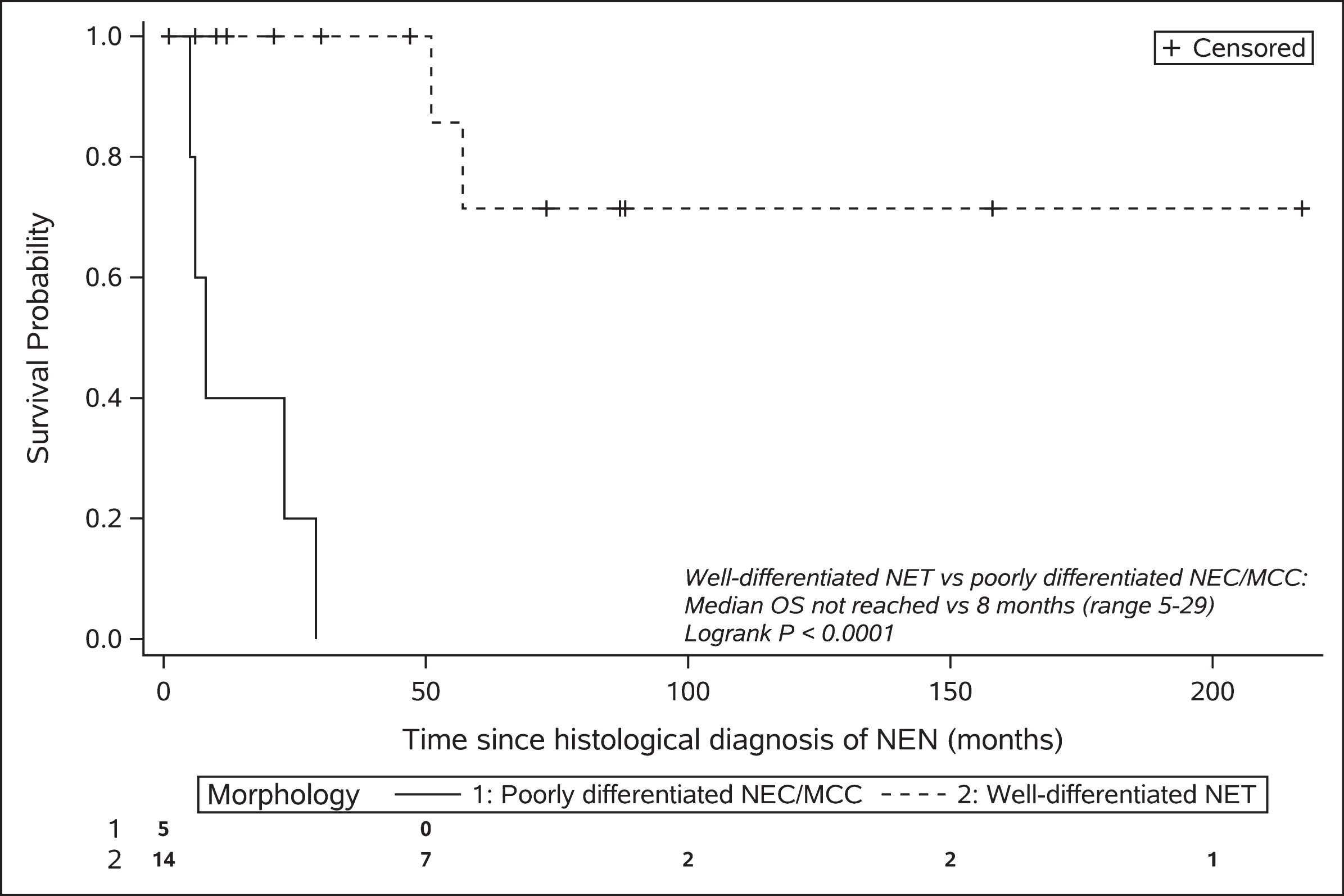
Kaplan-Meier plot of overall survival stratified by morphology.
HIV and concomitant NEN is an uncommon occurrence. The Royal Free Neuroendocrine Tumour Unit is a large international referral center and has treated approximately 3,500 patients with NEN over the last 10 years. Within that time, we identified 19 patients with concomitant HIV, giving an HIV prevalence of close to 0.5% in the NEN population. This might be an underestimate given that our unit, similar to many others, does not routinely screen patients for HIV infection. However, this is somewhat higher than the HIV prevalence in adults in the United Kingdom (0.17%) [26].
This cohort was predominantly male (84%) and HIV comorbidities and second primary cancer diagnoses were common. The characteristics of NEN including diagnosis in the sixth decade of life, and the predominance of well-differentiated (14/19; 74%) as opposed to poorly differentiated tumors, mirror those of the general NEN population [1, 27–30], and this likely reflects the fact that the majority of our cohort with known HIV were receiving treatment with ART (14/15; 93%).
In terms of overall survival, patients with NETs of the lung (n = 5 typical carcinoid) were all alive after a median follow-up of 73 months (range 6–217), and had the best prognosis owing to low grade histopathology and low rates of metastases at diagnosis. This is supported by the general NET literature, which documents a 5-year survival rate for typical pulmonary carcinoid tumors of 87–90% [31, 32], although late recurrences have been reported [3, 33] as demonstrated in two of our patients, and thus long-term follow-up is important.
The patients with well-differentiated midgut and pancreatic NETs also had a relatively good prognosis, with 4/6 (67%) alive after a median follow-up of 54 months (range 30–158; 3-year survival rate 100%; median OS not reached). This is not inferior to survival rates in well-differentiated (G1/G2) midgut and pancreatic NET in the wider NET population, with a 3-year survival rate reported as 80% and 62% respectively [1]. Three patients, with localized disease or small volume metastatic disease, did well after resection of the primary followed by liver-directed therapy or somatostatin analogues. Two patients with extensive metastatic disease had a more difficult course requiring multiple sequential therapies.
The five patients with poorly differentiated NEC or MCC, as anticipated, demonstrated a much poorer prognosis compared with the well-differentiated NET population (Fig. 1). The median PFS following platinum-based chemotherapy (5.5 months, range 2–11) and median overall survival (8 months, range 5–29) was not dissimilar to the wider NEC and MCC populations [34–37].
These findings must be interpreted in light of the limited statistical power available in analyses of rare diseases. Our study is limited by the small number of cases available and the retrospective, single-cohort design. This study also reflects a single-institution experience and while this allows for more homogeneous clinical practice the results may not be generalizable to other cancer centers. The Royal Free Neuroendocrine Tumour Unit is a large international referral center, and while this has permitted focus on a very rare subgroup of patients there may also be a potential bias towards rapid and comprehensive evaluation of neuroendocrine neoplasms. A multicenter, prospective study is required to validate our findings with inclusion of a formal non-HIV comparator group.
Special considerations in the management of patients with NEN and HIV
Drug-drug interactions
Many studies have shown that the combined treatment of cancer and HIV is safe and improves outcomes [38, 39]. However, drug-drug interactions and the need to maximize ART/cancer tre-atment efficacy must be taken into consideration [40]. Evidence-based, drug-drug interaction resources, such as the University of Liverpool HIV Drug Interactions Database (https://www.hiv-druginteractions.org/checker), are useful tools for the clinic.
Many drugs used in ART (e.g. protease inhibitors [PIs], non-nucleoside reverse transcriptase inhibitors [NNRTIs] and chemokine receptor antagonists) have the potential to cause drug interactions due to their ability to induce or inhibit the cytochrome P450 (CYP450) enzyme system. Many chemotherapy agents and molecular targeted therapies are also metabolized through the same pathway, hence there is a high potential for drug interactions with CYP450-metabolised ART. Focusing on NEN therapies, the antimetabolite agents (e.g. 5-fluorouracil), antitumor antibiotics (e.g. streptozocin) and platinums are not metabolized by the CYP450 system and therefore are unlikely to be altered by ART. In contrast, camptothecins (e.g. irinotecan) are eliminated by non-enzymatic routes and are substrates of CYP450 and UGT isozymes, and are consequently more likely to be altered by CYP450-metabolised ART [41]. Bidirectional drug interactions with CYP450-metabolised ART can also be anticipated with alkylating agents (e.g. temozolomide), epipodophyllotoxins (e.g. etoposide), tyrosine-kinase inhibitors (e.g. sunitinib), mTOR inhibitors (e.g. everolimus) and dexamethasone. While there are no randomized trials to guide the optimal ART regimen to be co-administered with these agents, ART that is metabolized independently of the CYP450 system (e.g. NRTIs, raltegravir, enfuvirtide) or that are substrates but do not induce or inhibit CYP450 enzymes (e.g. rilpivirine) are preferred [40, 42]. An evidence-based and regularly updated summary detailing the above described interactions between cancer therapies and all generations of ART can be found on the Liverpool drug interactions website (https://www.hiv-druginteractions.org/prescribing-resources -> treatment selector (by therapeutic indication) -> cancer therapies).
In our cohort, several ART regimens were used concurrently with various anti-cancer therapies, including somatostatin analogues, molecular targeted therapy with sunitinib, chemotherapy with carboplatin/etoposide, 5FU/cisplatin/streptozocin or 5FU/irinotecan and the anti-programmed cell death-1 (PD-1)/-programmed death ligand-1 (PDL-1) inhibitors, avelumab and pembrolizumab (Table 2 and Table 3). No significant drug-drug interactions were identified in our cohort; however, to minimize this risk every anti-cancer therapy and ART regimen was reviewed by a specialist pharmacist. One patient receiving dolutegravir/emtricitabine/tenofovir developed life-threatening diarrhea 6 days following cycle 1 5FU/irinotecan. There is no known interaction between dolutegravir/emtricitabine/tenofovir and irinotecan and an interaction between these drug regimens was considered unlikely. Although not formally tested, dihydropyrimidine dehydrogenase deficiency was also considered unlikely as the patient had previously received 5FU/carboplatin/streptozocin, alongside the same ART regimen, without harm. It was therefore concluded that the diarrhea was most likely secondary to the irinotecan.
Immune checkpoint inhibitors and HIV
Three patients in our NEC/MCC cohort received immunotherapy with PD-1/PDL-1 inhibitors; however, outcomes were relatively poor in this small cohort. In the past, HIV positive patients have been excluded from checkpoint inhibitor clinical trials given concern regarding immune-related toxicity. Nevertheless, observational studies including a phase II single arm prospective study in patients with HIV and solid organ malignancies [43], suggest similar response rates and toxicity profiles compared to the non-HIV population [44–46]. Furthermore, animal models have shown that inhibiting PD-1 signaling can reduce HIV viral loads [47] and may play a role in immune reconstitution by restoring HIV-specific CD8 + T-cell function [48, 49]. A systematic review reporting the tolerance profile of immune checkpoint inhibitors, their effects on HIV viral loads, CD4 + cell count, HIV reservoirs and/or HIV-specific CD8 + T cells, has been recently reported [50]. Thirty-one articles were included, with a total of 176 participants. The side effect profile was similar to the wider population, with 12% experiencing serious adverse events and 49% non-severe adverse events. Plasma viral loads remained stable in 91.9% of patients, increased in 5.8% and decreased in 2.3%. CD4 + counts remained stable in 60.7%, increased in 24.6% and decreased in 14.7%. Most of the trials did not characterize HIV-specific CD8 + T cells as well as viral load, but in a small number of patients, transient plasma viral load increases were noted followed by a boost in HIV-specific CD8 + T cells then associated with a decrease in HIV-DNA.
Overlapping toxicity
Anticancer drugs without potential for drug-drug interactions can share side effects with ART that are worsened when administered together, although no overlapping toxicities were seen in our cohort. For example, didanosine, stavudine, maraviroc and zidovudine can cause hepatotoxicity and should be avoided in combination with NEN chemotherapy drugs that rely on hepatic metabolism (e.g. etoposide, irinotecan) [41]. In contrast, the NRTIs, abacavir, emtricitabine, lamivudine and tenofovir, and the NNRTI, efavirenz are less likely to be hepatotoxic [41].
The molecular targeted therapies cause less myelosuppression compared with chemotherapy but may, however, have other potentially overlapping toxicities with ART [13]. Sunitinib, approved for the use in metastatic pancreatic NET, can cause QT prolongation, hypertension and increased cardiovascular events [51]. The boosted PIs, as well as rilpivirine and efavirenz, can also cause QT prolongation and should be avoided in combination with QT-prolonging molecular targeted agents given the risk of arrhythmia and sudden death [15, 41]. The mTOR inhibitor, everolimus, used in patients with gastrointestinal, pancreatic and bronchial NET, is associated with an increased risk of hyperglycemia and hypertriglyceridemia [9, 10]. PI drugs are also associated with hypertriglyceridemia, hypercholesterolemia, insulin resistance and hyperglycemia, and such risk factors may synergize.
Prophylaxis against opportunistic infection
Chemotherapy drugs, especially lymphotoxins such as temozolomide which is often used in patients with progressive pancreatic NET, can cause CD4 count depletion and increase the risk of opportunistic infections including cytomegalovirus and other herpes reactivations, mycobacteria infections and invasive fungal infections [15]. Opportunistic infection prophylaxis may therefore need to be commenced during chemotherapy, and regular monitoring of CD4 counts in HIV patients receiving chemotherapy is vital. This may also be important in patients treated with PRRT. PRRT with 177Lutetium, used to treat patients with well-differentiated, somatostatin receptor-expressing NETs, can also cause significant lymphopenia [11] and patients with high volume bone metastases and prior treatment with chemotherapy may be more prone to PRRT-induced myelosuppression. Two patients in our cohort were treated with PRRT. Neither developed myelosuppression throughout four cycles of PRRT; however, one patient had a drop in CD4 count to 114 cells/mm3 during his subsequent line of therapy with 5FU/carboplatin/streptozocin. He was commenced on PCP prophylaxis with pentamidine which was later stopped after the completion of chemotherapy and CD4 recovery.
Hepatitis B reactivation
Two patients in our cohort had antibodies to hepatitis B core antigen. In the setting of chemotherapy, these patients should be commenced on anti-viral prophylaxis to prevent HBV reactivation [52]; however, it is essential that ART is commenced prior to lamivudine or tenofovir monotherapy which can lead to the development of ART resistance [40].
Conclusions
Within the limits of a small descriptive cohort study, we found no evidence in the era of ART that patients with HIV and NEN are diagnosed at a younger age, nor do they have a poorer prognosis compared with the wider NEN population. Thus, patients with HIV and NEN should be managed similarly, with pursuit of surgical resection in the setting of localized or small volume metastatic disease which offers the only chance of cure. In the unresectable disease or metastatic setting, the full breadth of liver-directed therapies and systemic therapies should also be offered to these patients to support best NEN outcomes, alongside optimization of their ART regimen to minimize the risk of drug interactions and treatment-related complications. Nevertheless, this patient cohort has unique characteristics with a high incidence of comorbidities and significant potential for therapy drug-drug interactions and overlapping toxicities. Their management by a multidisciplinary team including oncologists, HIV physicians, endocrinologists and specialist pharmacists, is paramount.
Author contributions
AH and ML collected the data. AH performed the data analysis. AH and KS drafted the manuscript. All authors critically revised and approved the final manuscript.
Conflict of interest
The authors declare no Conflict of interest.
Funding
This project was funded by the Royal Free Charitable Trust (Quiet Cancer) Grant 311 and the Parasol Foundation Trust.
M.L. is funded by the China post-doctoral Science Foundation