
Abstract
BACKGROUND:
Conventional hamstring (HAM) stretching therapeutic effects are not substantiable in neuromusculoskeletal conditions with HAM tightness or shortness. We developed a kinetic chain stabilization exercise to provide a more sustainable effectiveness in adults with HAM tightness. However, its therapeutic effects and underlying motor mechanisms remain unknown.
OBJECTIVE:
To compare the effects of traditional active HAM stretching (AHS) and kinetic chain stretching (KCS) on electromyographic (EMG) amplitude and hip flexion range of motion (ROM) in participants with HAM tightness.
METHODS:
In this randomized controlled trial, 18 participants (mean age: 25.01
RESULTS:
Compared to AHS, KCS led to greater increase in the hip flexion ROM and EMG activation amplitudes in the left and right EO and left IO. Post-test hip flexion ROM data in both the groups were higher than the pre-test data.
CONCLUSION:
KCS produced more sustainable effectiveness in hip flexion movement and EMG motor control patterns in participants with HAM tightness than AHS.
Introduction
Hamstring tightness or contracture is a prevalent neuromusculoskeletal condition affecting essential daily movements such as sitting, standing, and walking in conditions like hemiparetic stroke, spastic diplegia, and Parkinsonism [1, 2, 3]. This issue often leads to functional and structural impairments within the lumbo-pelvic-hip kinetic chain, potentially resulting in back pain and hamstring strains [4, 5, 6]. Functional or structural impairments in the lumbo-pelvic-hip complex may not resolve until adequate hamstring length is restored [7, 8]. Failing to address this concern can lead to heightened hamstring tension and stiffness, thereby contributing to complications within the lumbo-pelvic-hip complex [9, 10, 11]. Prolonged shortening of the hamstrings prompts them to become relatively stiffer compared to lumbar spine tissue, resulting in a posterior pelvic tilt and lumbar spine flexion, causing an anterior shearing force. This, in turn, may lead to posterior derangement of lumbar intervertebral discs and spinal structures, commonly observed in the L4-5 vertebrae [12, 13]. Such posterior derangement of the lumbar intervertebral discs causes discogenic low back pain (LBP) and spondylolisthesis [14, 15].
Contemporary therapeutic techniques including proprioceptive neuromuscular facilitation (PNF) hold-relax and contract-relax techniques, static stretching, and dynamic stretching have been used to address hamstring tightness or shortness. However, these techniques have yielded inconsistent outcomes [16, 17, 18, 19]. Some studies attribute the increased muscle extensibility after single stretching sessions or short-term traditional active hamstring stretching (AHS) programs to modified sensations [20, 21, 22, 23]. Weppler et al. suggested that modifications to the AHS may be necessary to address these factors [24]. Recently, the lumbo-pelvic-hip kinetic chain concept emphasizes the interconnectedness of body segments during movement and stabilization [25]. Kinetic Chain Stretching (KCS) has been introduced as a critical component of intra-abdominal pressure management and dynamic spinal stabilization prior to movement [26]. The underlying mechanism of KCS is that weaknesses or dysfunctions in core and gluteus muscles can lead adjacent muscles like the hamstrings to become overactive or compensatory [27]. Therefore, KCS practice emphasizes core stabilization before hamstring stretching to effectively address these compensatory mechanisms and improve overall movement efficiency [25, 27]. This technique focuses on enhancing hip flexion and knee extension coordination, alongside motor control within core (diaphragm, internal oblique [IO], external oblique [EO]) and hip muscles during walking and running [28, 29, 30].
Despite the potentially important clinical contributions of the KCS to hamstring shortness, the effectiveness of hamstring stretching exercises with or without core stabilization in improving hamstring flexibility remains unknown. Thus, the aim of this study was to compare therapeutic effects of the KCS and AHS on hamstring muscle activity, hip joint angle, and satisfaction levels. Our hypothesis suggests a difference in hamstring flexibility and core chain muscle activation, as assessed through maximal active hip joint flexion angles, between AHS and AHS with KCS among individuals with hamstring tightness.
Method
Participants
We enrolled 18 male participants with hamstring tightness (mean age, 25.01
Procedures
The research produced a sequence of random numbers using a computer generated simple random number table to ensure unbiased and unpredictable allocation. Eighteen participants were recruited and assigned to either group AHS or KCS based on odd or even numbers. The allocation procedure was carried out by a researcher. A standardized experimental protocol was meticulously maintained, encompassing uniform verbal instructions, consistent testing intervals, and sequence uniformity. This uniformity was upheld during both the pre-test phase involving assessments of AROM and electromyography (EMG), as well as the subsequent intervention (AHS or KCS), followed by the post-test phase. The ASLR test was administered while participants were supine. Following proper positioning, participants were instructed to achieve complete muscle relaxation. Prior to data collection, participants underwent a preliminary familiarization session for the ASLR test to ensure standardized and consistent test execution. Upon instruction, participants gradually elevated their leg to a comfort level, under the careful guidance of the experimenter to ensure a measured and controlled motion. Utilizing diverse sensors and an electric goniometer, data were accurately captured. Preceding the intervention, each participant executed an active hip flexion AROM to establish baseline measurements. A visual representation of the study protocol is provided in Fig. 1. Simultaneously, we conducted measurements of electromyography (EMG) and kinematic data as participants performed the ASLR test. Stretching measurements were subsequently carried out by both groups as detailed below. The assessment of AROM was derived from an average of three repetitions. Each group adhered to the subsequent methodology. The intricacies of this procedure are expounded upon in the ensuing sections. This paper proceeds to elaborate on the delineated process in subsequent sections.
Active hip flexion range of motion test
We measured the active hip flexion range of motion (ROM) using a smartphone placed on the tibial crest, 5 cm distal to the superior border of the lateral malleolus on the unilateral leg. The ASLR test in this study maintained the ankle in a neutral position (90∘) with no added dorsiflexion or plantar flexion (Fig. 2). To measure the angle change, we used the GetMyROM Pro software (version 1.0.3; Interactive Medical Products, Hampton, NH, USA). The validity intra-class coefficient was reported to be 0.96–0.97; test-retest reliability was reported to be 0.84–0.93 [34]. We used an iPhone 13 Pro (128 GB, model no. MLV93KH/A; Apple Inc., Cupertino, CA, USA) with GetMyROM Pro software, an inclinometry-based application to measure hip ROM.
Study flow chart.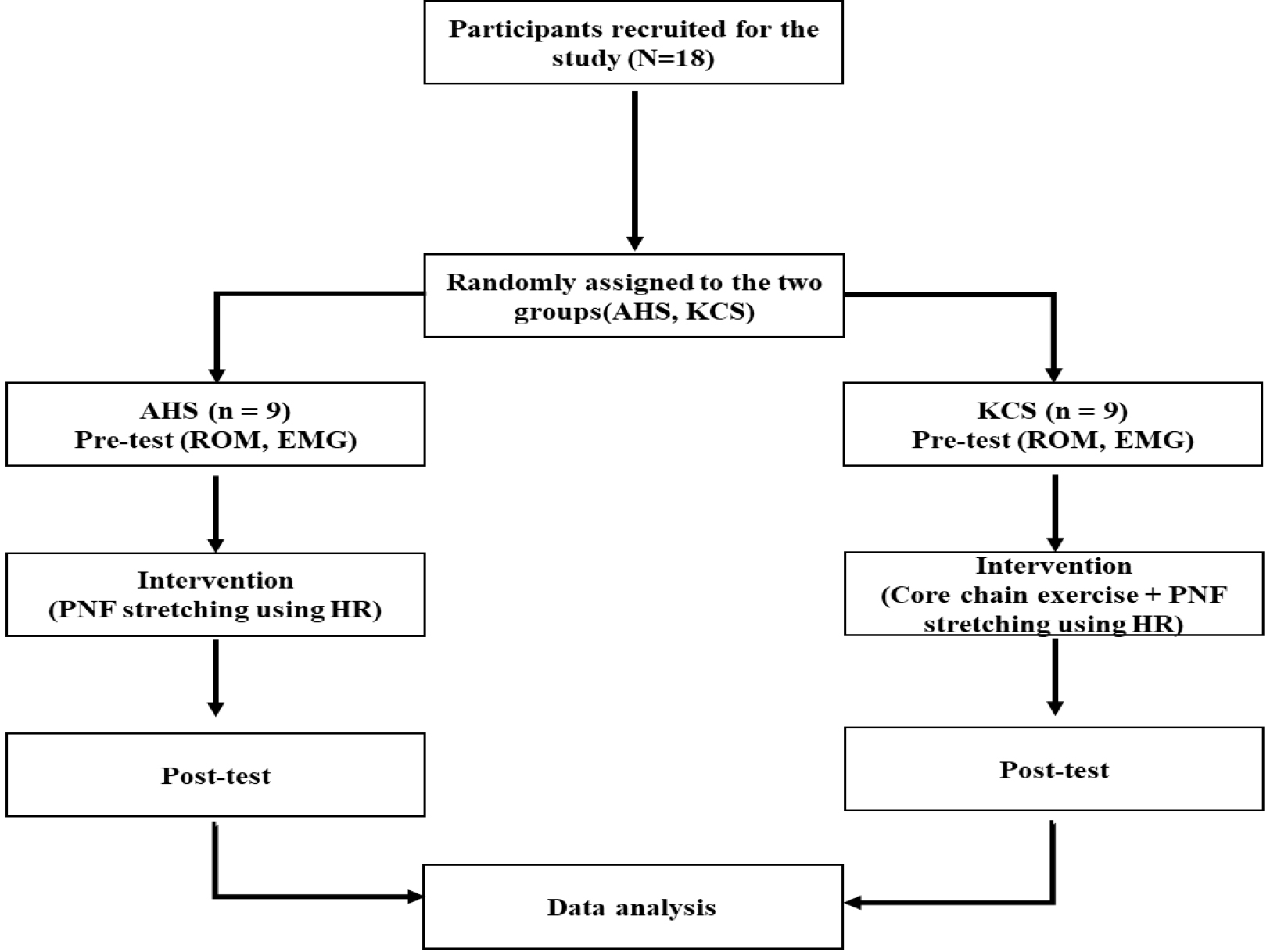
Measurement of the active range of motion of the hip joint.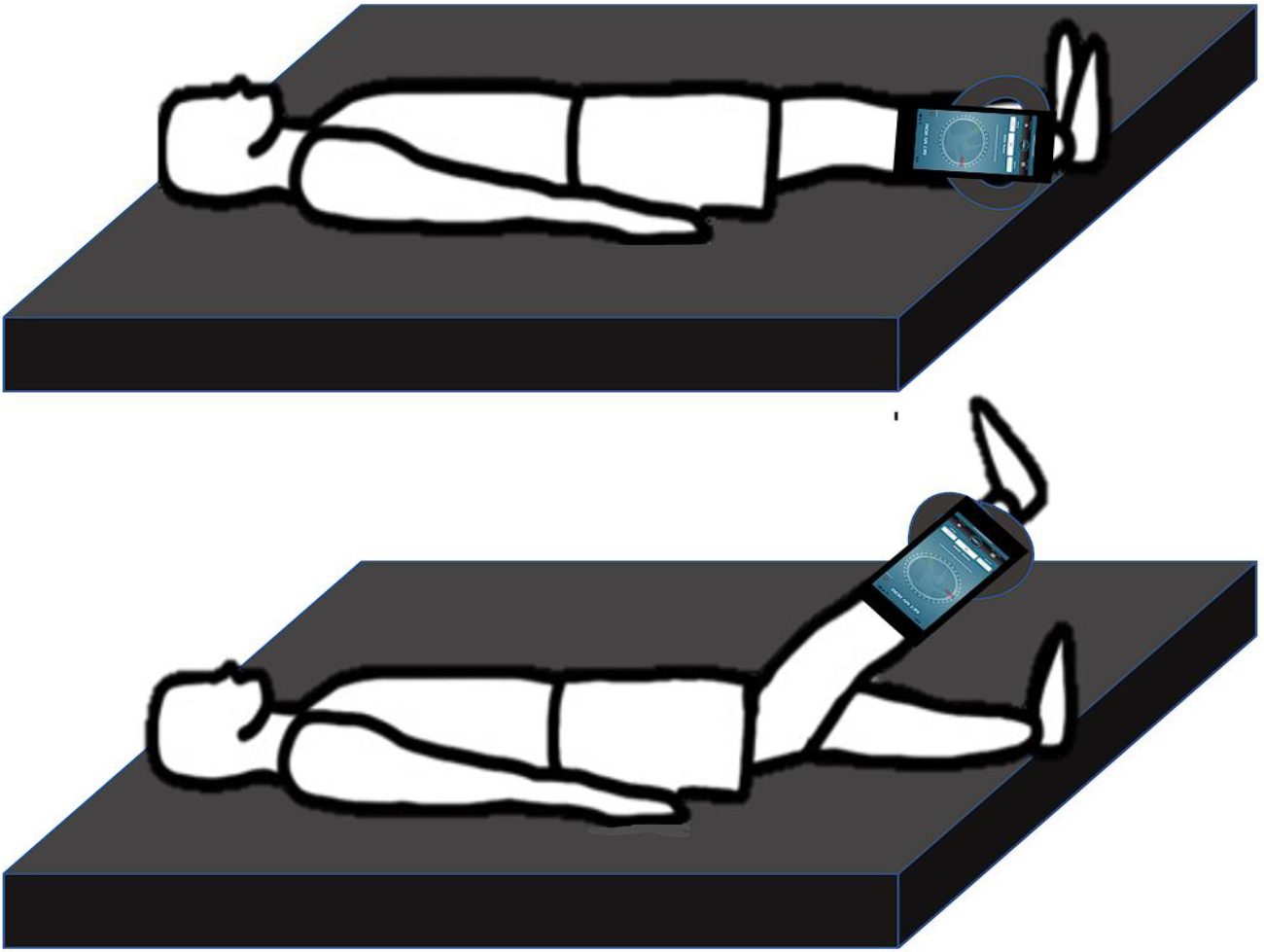
Surface EMG signals were acquired using the Ultium EMG system (Noraxon Inc., Scottsdale, AZ, USA), in conjunction with the MyoResearch software package (ver. 3.18, Noraxon, Inc., Scottsdale, AZ, USA). A sampling rate of 1500 Hz was employed, with band-pass filtering ranging from 50 Hz to 450 Hz, and no application of notch filters. Root mean square calculations were conducted utilizing a 50 ms moving window, with an overall gain set at 500. Exceptional signal quality was ensured with a common mode rejection ratio exceeding 100 dB and an input impedance surpassing 100 Mohm. Participants assumed a designated position on the mat, and double electrodes were meticulously affixed in compliance with Cram’s surface EMG guidelines. Prior to electrode placement, target skin areas were appropriately prepped, involving shaving and disinfection using rubbing alcohol. Electrode pairs were strategically positioned over specific muscles: bilateral rectus abdominis (RA), bilateral external oblique (EO), bilateral internal oblique/transverse abdominis (IO/TrA), bilateral lumbar erector spinae (ES), unilateral rectus femoris (RF), and unilateral biceps femoris (BF). Detailed electrode placement procedures were previously delineated [35]. Maximal voluntary isometric contractions (MVIC) for the aforementioned muscles were conducted, involving three repetitions for each muscle. Data were subsequently analyzed through the MyoResearch software package on a notebook PC. Muscle activity was recorded over a 7-second duration, and the averaged values from all three trials were employed for subsequent analysis.
Interventions
Traditional active hamstring stretching using hold-relax
PNF stretching employs the hold-relax technique to mitigate disruptions in the neural activity of linked muscles, autogenic inhibition, and myotatic reflexes [36]. The hold-relax technique involves lengthening the muscle to its limit, followed by an isometric contraction lasting up to 10 seconds. After this, the limb is passively moved into the new end range. This technique is used to improve muscle flexibility [18]. In Group 1, for hamstring stretching with AHS, the subject lies supine with hips flexed at a 90-degree angle. The therapist extends the knee for a mild hamstring stretch. The subject then isometrically contracts the hamstrings by flexing the knee against the therapist’s resistance at about 50% of maximal strength, ensuring no knee movement for 8 seconds. Upon relaxation, the therapist further stretches the hamstrings to a mild or moderate sensation, maintaining this position for 30 seconds. This stretching routine is repeated three times each session [37] (Fig. 3). Afterward, a two-minute rest period was allowed before measuring the active hip flexion ROM.
Traditional active hamstring stretching using hold-relax.
Kinetic core chain (a) None-Kinetic core chain (b) Kinetic core chain.
Kinetic chain hamstring stretching.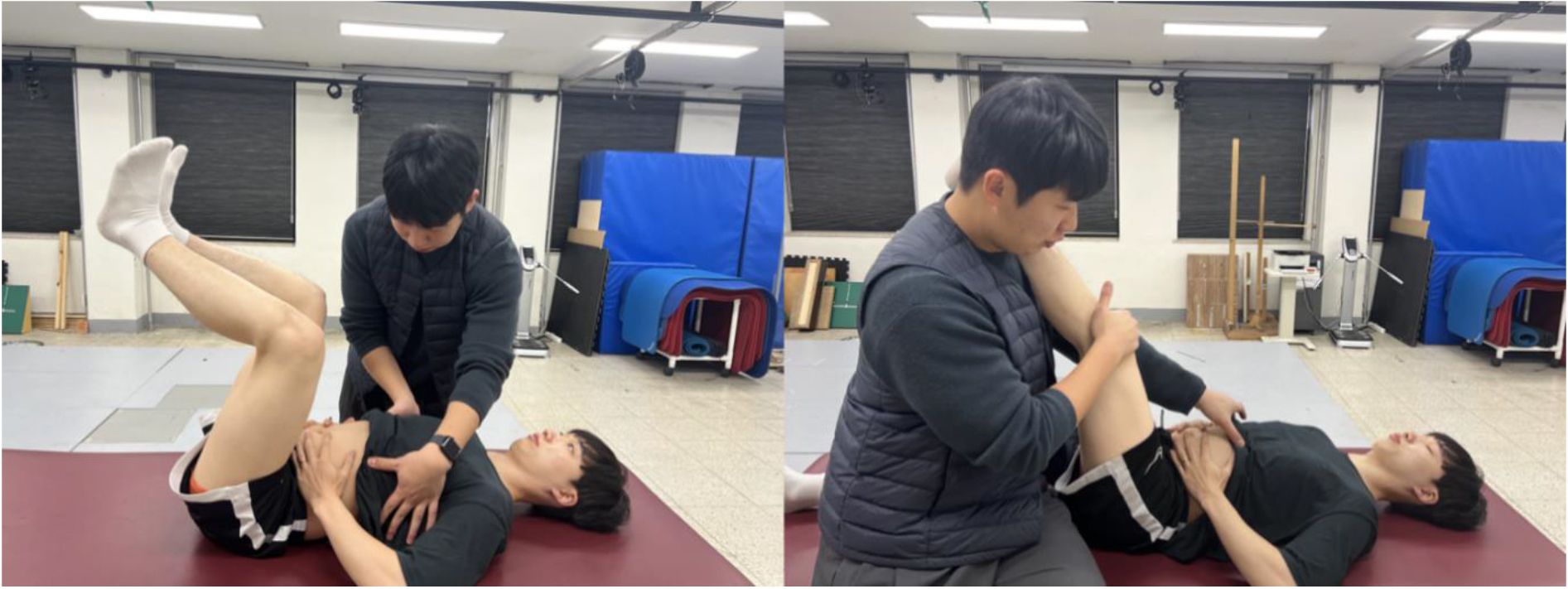
The KCS theory suggests that deep core stabilization muscles such as the diaphragm, transversus abdominis/internal oblique, multifidus, and pelvic floor, create intra-abdominal pressure (IAP) during inspiration. This is stabilized by the reflexive coactivation of external stabilizers like the rectus abdominis, external obliques, and erector spinae [30] (Fig. 4). Core stabilization forces combine with external forces to manage stabilization and movement, particularly in response to external perturbations and dynamic limb movements [29]. In Group 2, participants followed the same protocol as Group 1, incorporating AHS and core chain stability exercises. During the test, participants were instructed to maintain a neutral chest position to allow the diaphragm to descend effectively and generate IAP. This IAP eccentrically activates the transversus abdominis/internal oblique (TrA/IO), pelvic floor, multifidus, external oblique (EO), and other superficial muscles, subsequently concentrically stabilizing the spine in a cylindrical shape during dynamic movements of the extremities [27]. After mastering the technique, participants performed the ASLR three times while maintaining IAP through dynamic neuromuscular stabilization [25, 38]. For hamstring stretching with KCS, the investigator ensured neutral alignment of the thorax and rib cage, correcting any abnormalities like a flared rib cage. Participants were instructed to inhale to expand the ribcage and chest in multiple directions, creating intra-abdominal pressure through the co-activation of the diaphragm, TrA/IO, and pelvic floor muscles. The investigator focused on ensuring a symmetrical, cylindrical chest expansion by observing the anterior expansion of the xiphoid process, lateral expansion of the 10–12 ribs, and posterior expansion of the angulus costae. This process involved widening the intercostal spaces caudally without upward rib motion in the transverse plane [39] (Fig. 5). Afterward, a two-minute rest period was allowed before measuring the active hip flexion ROM.
Statistical analysis
We conduct power analyses using the G-power software (ver. 3.1.9.7; Franz Faul, Kiel University, Kiel, Germany) and obtained a sample size of 18 from a pilot study to achieve a power of 0.95 and an effect size of 0.5 with an alpha level of 0.05. Data were presented as mean and standard deviation. We tested the normality of the variables using the Shapiro-Wilk test. All variables were normally distributed. We used the paired
Results
Demographic characteristics
We recruited 18 participants, and each participant was randomly allocated using a random number table to either the AHS or KCS group. The independent
Demographic characteristics of the participants (
18, male)
Demographic characteristics of the participants (
a Values are presented as mean
Active hip flexion range of motion data during straight leg raise test (
Note. Values are expressed as the mean
The independent
Muscle activation data
The independent
Muscle activation data (
18)
Muscle activation data (
Note. Values are expressed as the mean
Overall satisfaction with the duration of the effect (
Note. Strongly satisfied
We observed a statistically significant difference between the KCS and AHS groups in terms of overall satisfaction with the duration of effects (Table 4).
Discussion
The present study demonstrated the effects of hip flexion movement with and without kinetic chain core stabilization exercise on active hip flexion movement and muscle activation patterns in the RA, EO, IO, ES, BF, and RF in non-symptomatic participants with hamstring tightness. Our findings support our hypothesis, revealing a greater augmentation in hip flexion AROM and intricate muscle activation patterns within the KCS group, in comparison to the control group. One of the distinctive contributions of our study lies in the novelty of exploring the therapeutic effects of KCS on AROM and EMG activation in non-symptomatic individuals with hamstring tightness. The dearth of comprehensive comparative data within existing literature limits direct comparisons. Nonetheless, our research offers a new dimension to this discussion, shedding light on the potential merits of KCS.
The post-intervention assessment of hip flexion AROM illustrated a more pronounced enhancement in the KCS group compared to the AHS group. While a multitude of studies have examined the outcomes of static and traditional stretching methods, the exploration of the impact of core exercises and stretching remains relatively sparse [18, 40, 41]. Our findings are in agreement with those of previous studies [42, 43, 44]. Rad et al. documented a considerable increase in hip flexion range of motion (29.3%) following 24 sessions of core stability exercises in non-symptomatic adults, surpassing the changes observed in the non-intervention control [44]. Cho et al. reported a positive effect of 4-week core exercises on hip AROM and pain in 30 patients with chronic LBP [43]. Similarly, core stabilization training using the pilates exercise enhanced lumbar flexion (23.5%) and extension (23.86%) in patients with LBP [44]. The positive shifts observed in AROM may be intrinsically linked to the establishment of proximal core stability, furnishing a robust foundation for dynamic flexion movements within the lumbo-pelvic-hip complex. Kibler et al. observed that baseball throwing performance (e.g., speed, angular velocity, and power) remarkably improves when core stabilization is achieved prior to upper-extremity throwing [29]. Such enhanced kinetic chain movement hinges upon the quality of neuromuscular coordination, with implications for regional, global, and local anatomical and biomechanical parameters essential for lumbopelvic stability, ultimately enriching hip flexion movement [29, 38, 45].
The EMG muscle activity data demonstrated greater improvement in the bilateral EO (90.66%) and left IO (93.40%) during KCS than during AHS. These results were similar to those of previous studies [25, 26, 27, 38]. Park et al. reported a more “normalized core-pelvic-hip EMG muscle pattern” when facilitating underactive deep core stabilization, which provided a stable basis for active hip movement [27]. Choi et al. reported substantial improvements in IO (168.90%) and EO (94.47%) muscle activation during or after a 2-week core stabilization program, resulting in better performance in upper extremity movement function [26]. Kolar et al. observed that automatic, reflexive core stabilization occurred when active shoulder or hip flexion movements were initiated in healthy adults but was impaired in individuals with chronic LBP [38]. Similarly, Yoon and You demonstrated coordinated core muscle activation in the diaphragm and TrA/IO muscles (MVIC 11-18%) following core stabilization exercise in both the healthy and LBP groups, contributing to dynamic limb movement [25]. Such enhanced core muscle stabilization activation in the EMG data plays an important role in improving hip movement [27]. It is plausible that when the ipsilateral hip-supporting zone contacts the surface, it activates the opposite OB chain muscles [29, 38, 46]. These anterior OB chains may be counterbalanced by the posterior chain muscles to upright and stabilize all spinal segments during dynamic hip movement, as in the SLR, producing an external (negative) stabilizing force movement. Internally, the IAP force is concurrently generated by a deep diaphragm-TrA-pelvic floor-multifidus proximal core chain during inspiration, which provides a counterforce to stiffen the KCS chain [29, 38]. The simultaneous synergetic force coupling action between the internal and external KCS chains renders a crucial foundation for distal extremity muscles, such as the hamstrings to be activated in coordination with the EO and IO during active hip flexion [46, 47, 48, 49, 50, 51].
A post-intervention survey was conducted following the 4 weeks of intervention Notably, the majority of participants in the KCS group reported a sustained effectiveness in hip joint movement or hamstring flexibility through the employment of KCS. Conversely, those in the AHS group reported limited lasting effects. The current survey results are similar to those described in previous studies [52, 53, 54]. Knappstein et al. observed that after hamstring PNF stretching, ROM increases reportedly lasting for 7 minutes [52]. Similar to other studies, changes in ROM following PNF have only been observed for a maximum of 10 min following stretching [53, 54]. A single passive stretching session does not permanently deform the muscle-tendon unit because the increase in joint ROM is only momentary [55]. Alternatively, some authors have proposed that acute ROM changes result from distorted stretch perception [56]. This can be explained by the immediate effects of increased hamstring muscle elasticity and nerve tissue extensibility [40]. Moreover, core stability offers a number of advantages, as the proximal and distal segments cooperate to produce and control forces to maximize motor function. The stability and stiffness of the spine are significantly influenced by increased intra-abdominal pressure caused by the diaphragm’s contraction [29, 57]. Most importantly, during “involuntary” subconsciousness, the subcortical motor control network is selectively activated [58]. The regulation of respiration observed during the core stabilization exercise may be explained by this subcortical network [59]. This interplay highlights the importance of core stability within the realm of involuntary or automatic stability paradigms. Furthermore, this stretching paradigm contributes to a nuanced understanding of the intricate control mechanisms driving core stabilization and its role as an effective stretching method for both acute and sustained flexibility.
A few limitations of this study should be considered in the future. First, the absence of IAP measurements, which necessitate a coordinated co-activation of various muscles, remains a noteworthy omission. Further research employing noninvasive pressure sensors may shed light on this aspect. Second, the exclusive inclusion of male participants warrants consideration, highlighting cultural sensitivities. Generalizing these findings to diverse pathological populations necessitates cautious interpretation. Third, the ultrasound was not used to ensure the descending movement of the diaphragm which is associated with spinal stabilization-induced IAP via coordinated auxiliary activation of the diaphragm, transverse abdominis, multifidus, pelvic floor, internal oblique, and external oblique muscles. However, we have used manual palpation to monitor the appropriate activation of these core muscles. Fourth, we included only individuals with hamstring tightness and excluded those with hamstring shortness. Hamstring tightness is operationally defined as reaching the end range of motion, while failure to reach the end range is considered hamstring shortness [60, 61]. In the following study, it is essential to recruit a diverse group of subjects, including those with muscle shortness and hamstring tightness, to effectively evaluate the efficacy of KCS in a range of neuromuscular conditions. Nevertheless, the post-interventional survey confirmed a more effective sustainability of the KCS, with its therapeutic effects lasting longer compared to that of the control group.
Conclusions
This empirical investigation has unveiled significant insights into the realm of hip flexion movement, both with and without kinetic chain core stabilization exercise, within individuals experiencing hamstring tightness. The study’s outcomes furnish clinical substantiation and augment our comprehension of the biomechanical intricacies inherent in kinetic chain core stabilization exercises. These findings offer invaluable contributions to the existing body of knowledge, particularly concerning the formulation of efficacious and enduring mobility exercises tailored to individuals grappling with hamstring tightness. The empirical evidence presented herein not only underscores the potential therapeutic efficacy of kinetic chain core stabilization exercises but also address the need for further research and practical applications in this domain.
Footnotes
Acknowledgments
This study was supported by (1) the Korea Health Industry Development Institute, grant (No. HI18C1687000020); (2) the Brain Korea 21 PLUS Project (Grant No. 2021-51-0151); (3) the Institute of Information & Communications Technology Planning & Evaluation (IITP) funded by the Korean government (MSIT) (Grant No. 20200011290022003); (4) the National Research Foundation of Korea (Grant No. RS-2023-00221762; No. 2022RIS-005); and (5) the Institute for Project-Y Seed Grant of 2023 (Grant No. 2023-22-0277).
Conflict of interest
None to report.