
Abstract
BACKGROUND:
Implant-restored patients with periodontitis have a higher risk of developing peri-implantitis, and helping them develop oral cleaning habits is significant.
OBJECTIVE:
To evaluate the effectiveness of motivational interviewing based on the transtheoretical model on the modification of oral cleaning behaviors of implant-restored patients with periodontitis.
METHODS:
Patients with periodontitis (
RESULTS:
Compared to the control, the experimental group demonstrated significantly better oral hygiene behavior after intervention (
CONCLUSION:
Motivational interviewing based on the transtheoretical model can effectively improve the oral cleaning behavior and periodontal health of implant-restored patients with periodontitis.
Keywords
Introduction
Periodontitis is one of the most important causes of dentition defect or missing dentition encountered in clinical practice. Most patients who clinically require dental implant treatment have a history of periodontitis. Some studies have shown that implant-retained prosthetics during the stable phase of chronic periodontitis is safe and feasible, because patients with periodontitis can also obtain short-term efficacy similar to that of periodontally healthy subjects through effective health maintenance [1]. Currently, there is consensus that periodontitis is not a clinical contraindication for implant-retained prosthetics; however, peri-implantitis is strongly associated with certain pathogenic bacteria [2] and patients with periodontitis have a higher risk of peri-implantitis than periodontally healthy patients after dental implant restoration [3]. Possible causes are as follows: first, periodontitis is a chronic disease and, even if it is successfully controlled with the help of professionals, if the patient does not place considerable emphasis on daily oral care, the risk of relapse remains very high [4]; second, as with other chronic diseases, to maintain long-term curative effect, periodontitis management requires high compliance of patients in their lifelong health management, including maintenance of good oral cleaning habits and regular revisits. Nevertheless, traditional oral hygiene education has little effect on patient compliance. Although it can urge patients to passively follow clinical direction in the short term, it is difficult to fundamentally reverse poor oral cleaning habits and health management in patients with periodontitis [5]. Therefore, improving patient compliance and helping patients to develop stable habits of personal oral cleanliness and health management is an important focus in management of patients with chronic periodontitis who have undergone implant restoration. Overall, there is a significant need to find a new method to better manage the oral health of patients with periodontitis who have undergone implant restoration.
In recent years, some scholars have attempted to introduce the transtheoretical model (TTM) and motivational interviewing (MI) from the field of psychology into health behavior change applications, such as cardiovascular medicine [6], orthopedic sports medicine [7], and pulmonary medicine [8], among others, and the effects were significant [9]. The TTM, also known as the stages of change model, suggests that health behavior change occurs when individuals move through five stages of readiness: precontemplation, contemplation, preparation, action, and maintenance. For the purpose of behavior change, TTM can determine specific behavior intervention strategies, according to the different needs of patients at various behavioral stages, and adopt different transformation strategies for each stage [10]. MI is a method to guide individuals to recognize and correct psychological barriers related to undesirable behavior from five aspects: relevance, risk, rewards, roadblocks, and repetition [11]. TTM and MI can help patients with chronic diseases improve their compliance and behavior, which finally contributes to promoting favorable outcome and improving quality of life [12, 13]. The effects of these two models on unhealthy behavior shifts have been confirmed in numerous ways to date [14]. Further, some scholars have demonstrated that a combination of the TTM and MI can effectively promote improved dietary behaviors among adolescent youth, as well as medication adherence of patients following stroke [15]; however, there have been no reports on the effects of MI based on the TTM on oral cleaning behavior of patients with periodontitis who have undergone implant restoration.
Therefore, in this study, we applied MI based on the TTM to patients with periodontitis who have undergone implant restoration, to explore the effects of this approach on oral health self-management, including oral cleaning behavior change and periodontal status of dental implants. Our research has potential to enrich the theoretical basis underlying clinical application of MI based on the TTM and help patients with periodontitis who have undergone implant restoration to obtain long-term and stable therapeutic effects.
Materials and methods
Study participants
The Department of Dentistry of Nanfang Hospital, Southern Medical University conducted this study between December 2018 and January 2022. The Ethics Committee of Nanfang Hospital, Southern Medical University approved the research.
And the study involved 70 patients with periodontitis proposed for implant restoration. Every individual signed an informed consent form. And then they were randomly divided into control (
Inclusion and exclusion criteria
Patients with periodontitis who meet the indication of dental implant and would accept related therapy were selected. In addition, they also need to be mentally healthy, capable of understanding and signing consent forms, and willing to receive regular follow-up.
The inclusion criteria for patients with periodontitis were as follows: 1) diagnosed with localized chronic periodontitis, according to the Classification of Periodontal Diseases issued by the American Academy of Periodontology in 1999 [16]; 2) periodontitis was controlled by conventional periodontal treatment before oral implant surgery; and 3) the remaining bone mass at the implant site was sufficient, and there was no need for vertical or horizontal bone augmentation procedures.
The exclusion criteria included: 1) patients with psychiatric or systemic disorders that would affect implant surgery; 2) those who did not consent to the study or cooperate with treatment; 3) subjects with smoking, alcohol abuse, or other unhealthy lifestyle habits; 4) patients who were pregnant or lactating; 5) patients complicated with diabetes, osteoporosis, or other related conditions; 6) patients who could not receive the full course of treatment and complete the entire course of follow-up.
Interventions
Patients in the control group received routine oral hygiene advice during the treatment, including information about perioperative considerations and oral health instructions related to periodontitis and oral implants. Patients in the experimental group received the same routine oral hygiene education as those in the control group plus MI based on the TTM. MI was conducted fortnightly with each interview taking 15–20 min, from the initial visit to 3 months after implant restoration. The specific process and content were as follows: (1) medical and nursing interview groups were established to discuss and develop implementation schemes for MI based on the TTM, and professional training regularly provided for all group members; (2) at first clinic visit, subjects completed open-ended questionnaires to evaluate their willingness to change their oral cleaning behavior, understand their preexisting problems, assess the stage of behavior change patients were in, and the duration and frequency of interview interventions were explained to patients and their families [17, 18]; and (3) the stage of behavior change of the patient was assessed through interviews, and patients were provided with information on how to promote health behavior change and improve their ability to achieve oral cleanliness, based on the different behavior stages they were in (details are provided in Fig. 1).
(a) Flowchart of the study; (b) Specific intervention measures of the motivational interviewing based on transtheoretical model.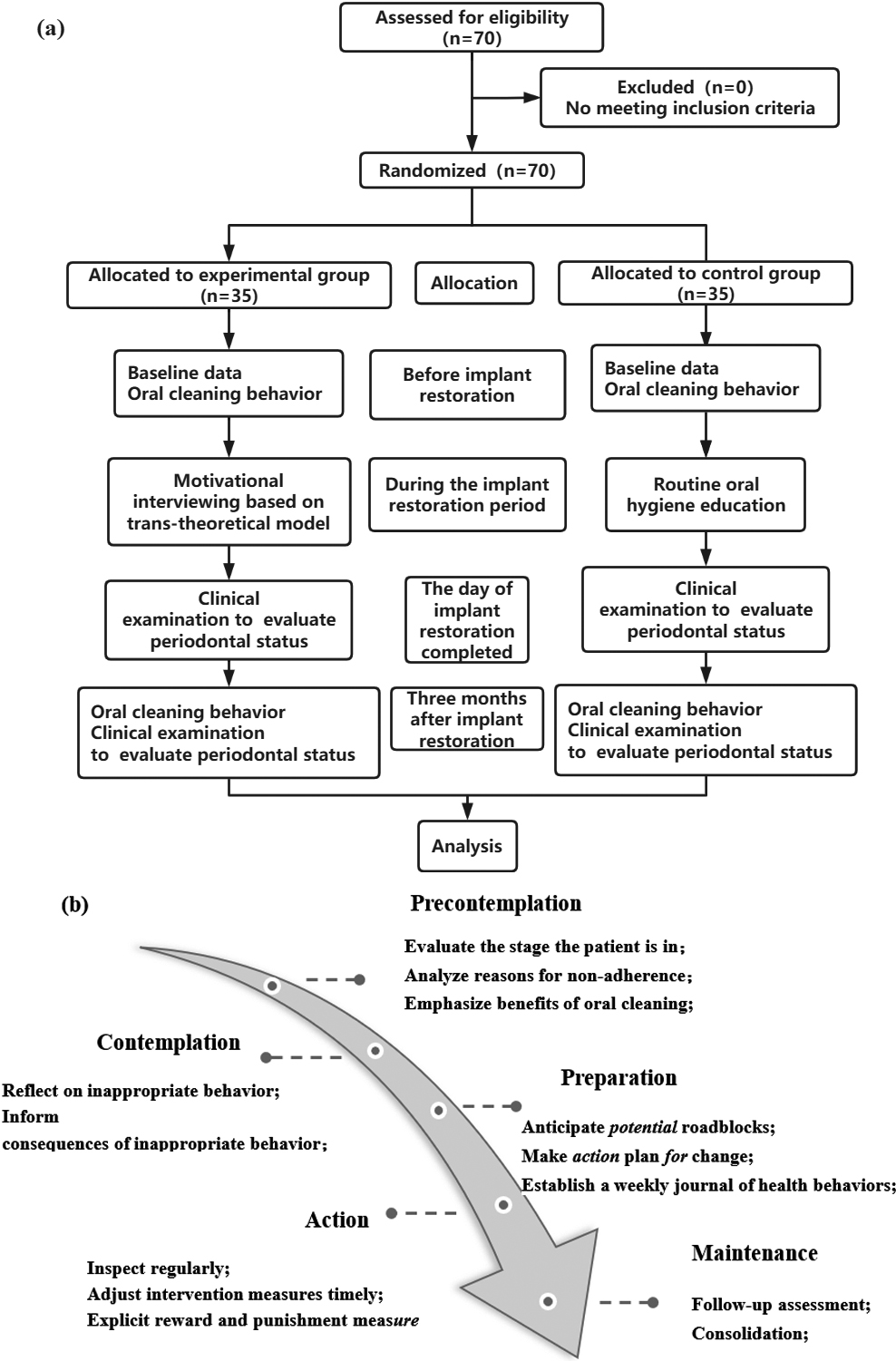
All medical staff involved were uniformly trained before implementation of the study, to ensure consistency of the operation process and mode.
Changes in oral cleaning behavior
An open questionnaire was developed to assess the stage of the oral cleaning behavior of the two groups at first clinic visit and three months after implant restoration. Patients assessed to be in the precontemplation, contemplation, or preparation behavior stages were considered in the first stages of dental cleaning behavior change [17]. Changes in patient oral cleaning behavior were evaluated by comparing differences in numbers of patients in the different behavioral stages before and after the two types of intervention.
Periodontal clinical indices
The periodontal health status of patients was evaluated using the modified plaque index (mPLI), modified bleeding index (mSBI), papilla index score (PIS), and probing depth (PD) on the day of implant restoration and 3 months after implant restoration.
mPLI: Areas around implants were examined using a rigid plastic probe (Click-Probe
mSBI: The probe was use to penetrate the subgingiva 1 mm around the implant and slid parallel to the implant along the buccal-lingual gingival margin, followed by waiting for 30 s. mSBI was then rated as follows: 0, no bleeding; 1, spotted bleeding; 2, linear bleeding in the gingival sulcus; 3, severe bleeding [20].
PIS: Gingival papilla height around the implant was measured and scored as: 0, no papilla; 1, less than half of the papilla; 2, at least half of the papilla; 3, papilla fills up the entire approximal space; 4, hyperplastic papilla [21].
PD: The probe was placed at six sites (mesio-buccal, mid-buccal, disto-buccal, disto-lingual, mid-lingual, and mesio-lingual) around the implant, and along the long axis of the implant, the probe was inserted into the pocket and measured depth from gingival margin to bottom. The average of the six sites was calculated [22].
Statistical analysis
SPSS 20.0 (IBM, New York, American) was used to analyze all data. Data for categorical variables were expressed as n (%), and data for continuous variables were expressed as mean
Results
Baseline data
Comparisons of baseline data from the two groups demonstrated that they did not differ significantly in sex, age, or educational attainment (Table 1).
Comparison of baseline data of patients in the two groups (
SD;
, %)
Comparison of baseline data of patients in the two groups (
Footnotes
Acknowledgments
The study was supported by the Science and Technology Project of Guangzhou Economic and Technological Development Zone (2020GH14) and the Clinical Research Program of Nanfang Hospital, Southern Medical University (2018CR022 and 2021CR016).
Conflict of interest
None to report.