
Abstract
BACKGROUND:
Vascular tortuosity is a prevalent morphological change that frequently occurs in arteries across different parts of the body.
OBJECTIVE:
To analyze the relationship between the tortuosities of the extracranial internal carotid artery (EICA) and extracranial vertebral artery (EVA) with mild cognitive impairment.
METHODS:
The tortuosity index (TI), vascular deviation degree, tortuosity degree, and angle number of the EICA and EVA were retrospectively analyzed and calculated in 160 patients who underwent computed tomography angiography (CTA) in this study’s department, and the Montreal cognitive assessment was adopted to evaluate the cognitive function of the patients.
RESULTS:
The differences in age, gender, arterial hypertension (AH), and diabetes mellitus (DM) between the normal group and the mild cognitive impairment group were statistically significant (
CONCLUSION:
There was a significant correlation observed between the TIs of both the EICA and EVA and the presence of mild cognitive impairment. Advanced age, female, HP, DM, and CHD were independent risk factors for EICA and EVA tortuosities.
Introduction
Vascular tortuosity is a common vascular morphological change that occurs in various arteries throughout the body [1]. The cerebral vessels, which primarily consist of the carotid and vertebral arteries, serve as the primary blood supply to the brain. Lesions affecting these arteries, such as cervical atherosclerosis and stenosis, have been found to be associated with the occurrence of chronic cerebral ischemia [2, 3]. Artery tortuosity is a common abnormal vascular morphology in neurology. It mainly refers to when the extracranial internal carotid artery (EICA) and extracranial vertebral artery (EVA) are too long and dilated, with the manifestations of twisted, circled, and looped blood vessels, resulting in an insufficient blood supply to the brain, which occur unilaterally or bilaterally. It has been suggested that chronic cerebral ischemia caused by carotid artery tortuosity may affect cognitive function [4]. However, since the etiology of vascular tortuosity remains unclear, whether it is a risk factor or cause of chronic cognitive impairment is still controversial [5, 6]. The tortuosity index (TI) is considered an important quantitative indicator to reflect the degree of vascular tortuosity and has a good repeatability [7]. We supposed that the TI in EICA and EVA were associated with the cognitive impairment, which also provide a new way to predict the cognitive function of patients. Therefore, the main objective of this study is to investigate the relationship between the EICA and EVA and cognitive impairment. Additionally, this study aims to identify potential risk factors that might contribute to the development of vascular tortuosity in these arteries.
Data and methods
Study objects
The data from a total of 160 patients who were hospitalized in this study’s department from May 2021 to March 2022 were collected, and the enrolled patients had all completed head magnetic resonance imaging (or computed tomography [CT]) together with cerebral and carotid CT angiography (CTA). There were 82 male and 78 female patients. The patients were 40–89 years old, with an average age of 66.54
Methods
General data collection
Statistical analysis of the clinical data was conducted for each patient, including taking their gender and age, their arterial hypertension (AH), diabetes mellitus (DM), and coronary heart disease (CHD) statuses, their total cholesterol (TC), triglyceride (TG), and platelet (PLT) counts, and their smoking and drinking histories.
Carotid CTA examination
A GE 64-slice spiral CT machine (Light Speed, VCT) was used to conduct the cerebral and carotid artery scanning with the scope ranging from the plane of the aortic arch to the cranial top. Iopromide 370 (370 mgI/mL) was used as the contrast and was injected through the median cubital vein (5 mL/s, and the total dosage was 90–100 mL). An ADW4.4 workstation was used for image post-processing, and curved planar reformation, multi-planar reconstruction, volume rendering, and maximum intensity projection were the foci of post-processing technology. The vascular TI, deviation degree (DD), tortuosity degree (TD), and angle number (AN) were measured with reference to the methods by Cao et al. [8].
Measurement of vascular morphological indicators
The vascular morphological indicators were as follows: (1) Tortuosity index: The calculation formula was vascular TI(%)
Vascular tortuosity index (TI) (%) 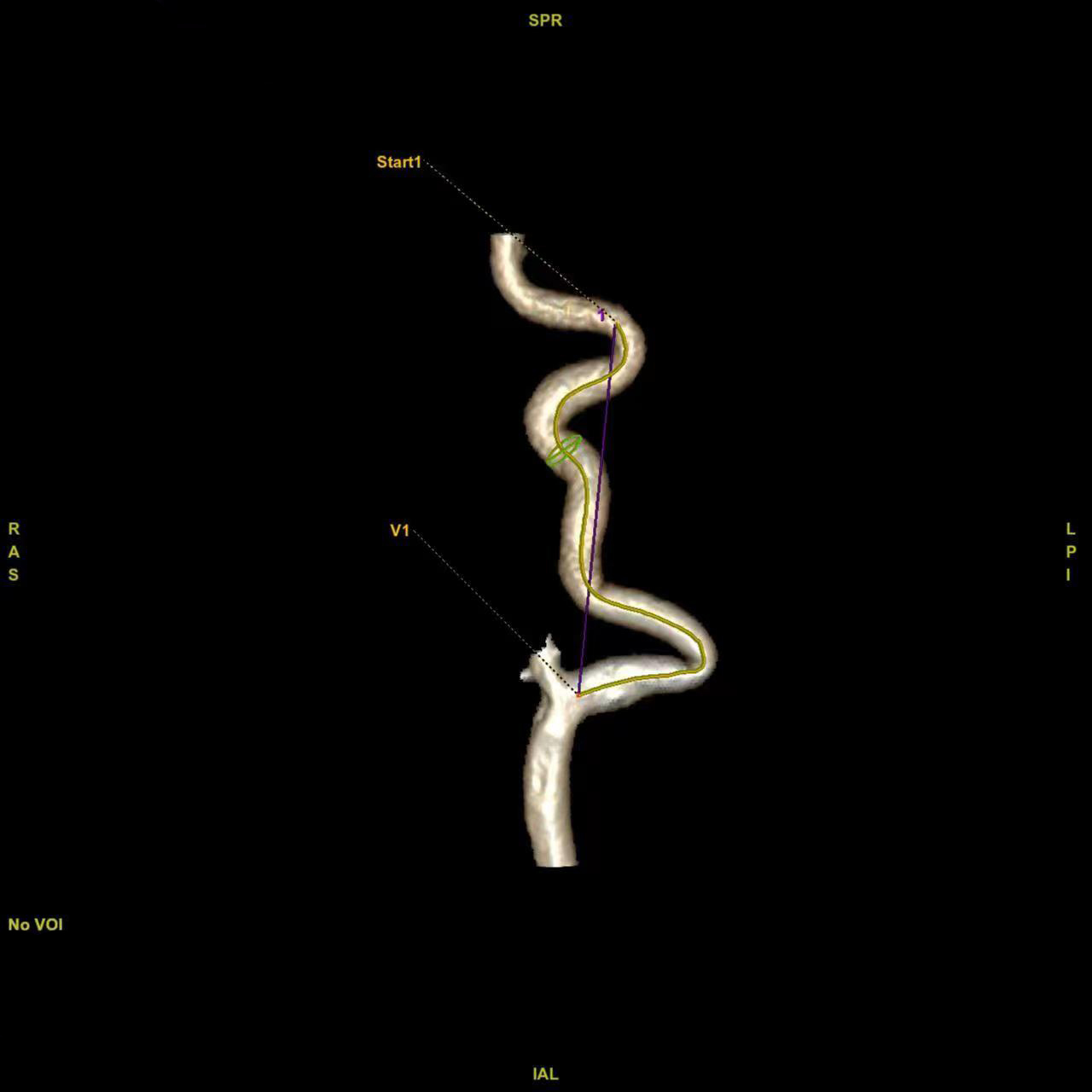
Vascular deviation degree (DD): A straight line was drawn between the two ends of the blood vessel, and DD was the vertical distance from the farthest point of the blood vessel deviating from the ideal straight line to the straight line.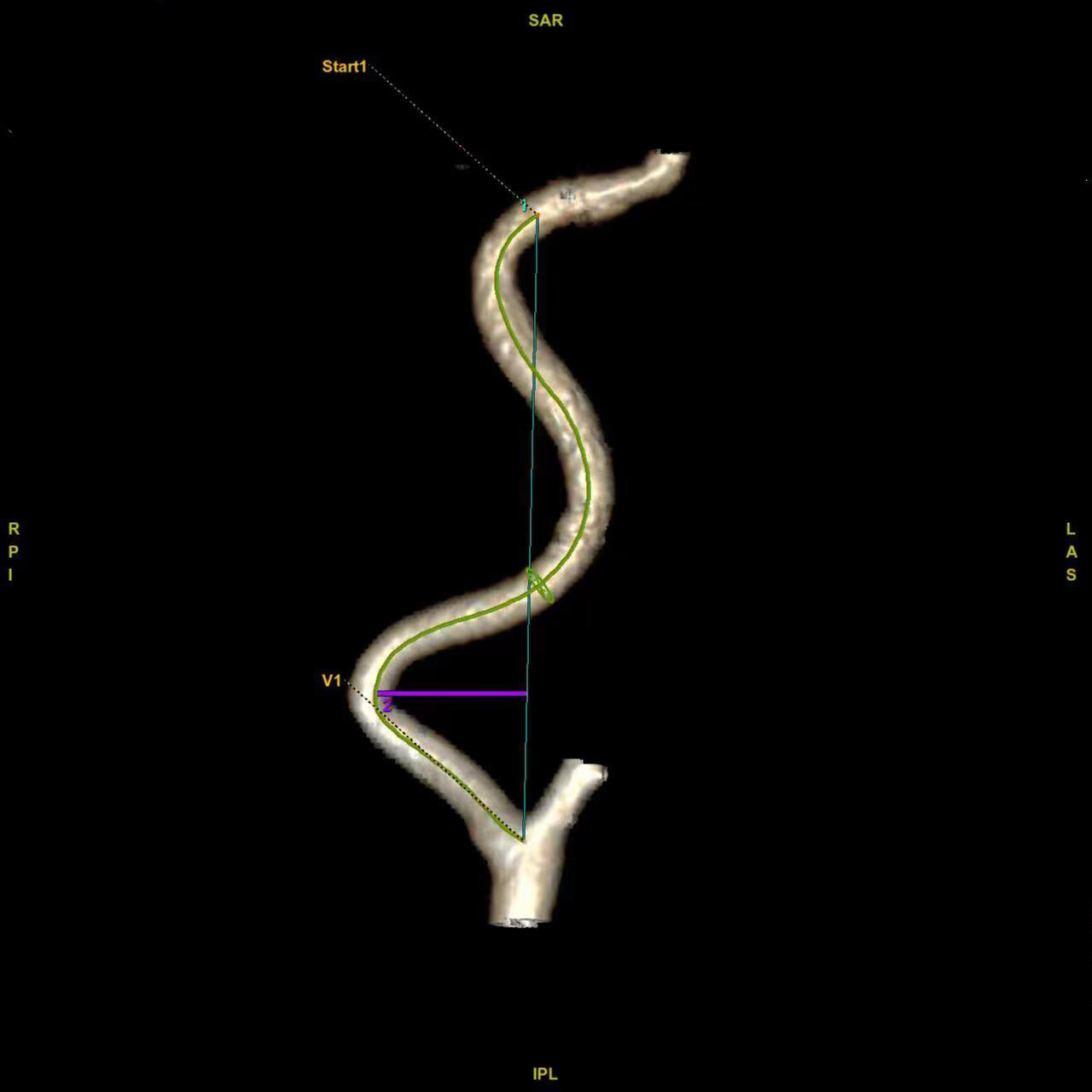
Measurement of vascular tortuosity degree and angle number.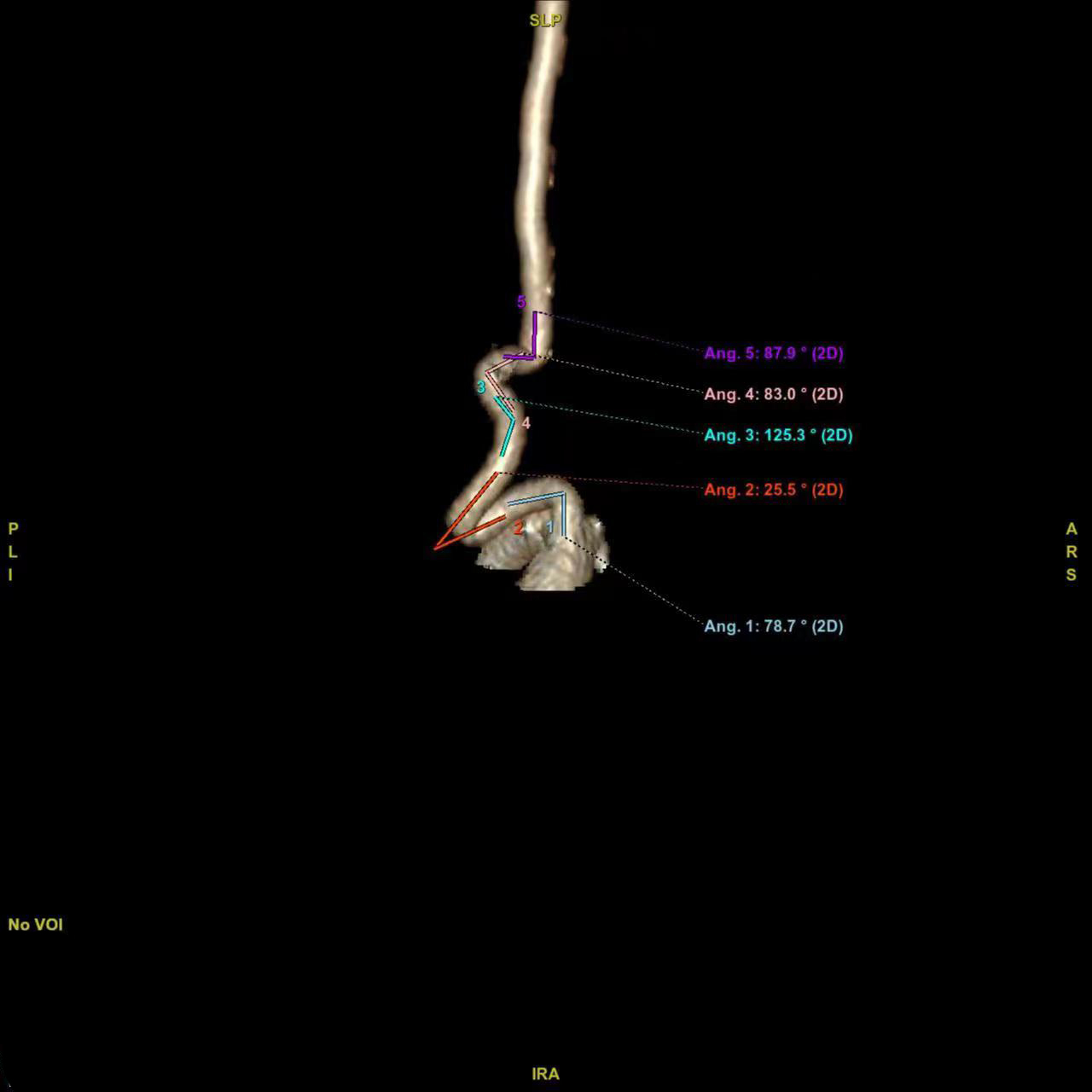
The cognitive function of each patient was assessed using the MoCA, which provides a total score of 30 points. A score below 26 points was deemed abnormal. For those with less than 12 years of education, 1 point was added to correct the educational bias score. The scoring was completed within 10 minutes by strictly trained neurosurgeons or full-time evaluators. In this study, patients with a score of
Statistical methods
Excel 2013 was used for data entry and SPSS 19.0 software was adopted for statistical analysis. The measurement data were expressed as means
Results
Univariate analysis of the cognitive function
The clinical information of the patients is illustrated in Table 1. Among all the enrolled patients, 87 had mild cognitive impairment, and 73 had normal cognitive function. The results showed that the differences in age, gender, HP, and DM between the normal and mild cognitive impairment groups were statistically significant (
Univariate analysis of the risk factors for cognitive impairment (Percentage %)
Univariate analysis of the risk factors for cognitive impairment (Percentage %)
Correlation analysis of tortuosity-related indicators and mild cognitive impairment
Correlation analysis between MoCA sub-score and carotid artery tortuosity index
Pearson correlation was adopted to explore the correlations between mild cognitive impairment and the carotid artery TI, vascular DD, vascular TD, and vascular AN. The results are shown in Table 2. The results showed that the carotid TI was negatively correlated with the MoCA score (
Correlation analysis of carotid artery tortuosity and sub-indicators of the cognitive function scores
The correlations between the TIs of the bilateral EICA and EVA and various sub-indicators of the cognitive function scores, including visual-spatial, naming, memory, attention, language, abstract thinking, and orientation, were assessed separately. The results are demonstrated in Table 3. It was revealed that the decline in visual-spatial ability was negatively correlated with the right EICA tortuosity (
Multivariate linear regression analysis of the risk factors of carotid artery tortuosity
Multivariate linear regression was used to analyze the impact of the numerical variables, such as age and TC, TG, and PLT counts, on the TIs of the bilateral EICA and EVA. The data all met the requirements of Durbin-Watson and collinearity. The results are illustrated in Table 4. The results showed that there were statistically significant correlations between age and the TIs of the bilateral EICA and EVA (
Multiple linear regression analysis of tortuosity-related risk factors
Multiple linear regression analysis of tortuosity-related risk factors
Student
A two-tailed
Discussion
Vascular tortuosity of the carotid and vertebral arteries is a prevalent cerebrovascular abnormality frequently observed in clinical practice, particularly among patients. This tortuosity often increases the difficulty of the operation in some cerebral vascular interventional examinations [9], which is a problem that requires attention in clinical practice. The etiology of internal carotid artery tortuosity is not completely clear yet, but it is mainly believed to be caused by congenital reasons, i.e., the factors existing in childhood and the acquired factors [10]. Although congenital embryonic dysplasia may be associated with carotid tortuosity [11], studies have demonstrated that internal carotid artery tortuosity was also affected by gender, age, and vascular risk factors. Koge et al. [12] found that the tortuous group was older and more female than the nontortuous group. In addition, the study by Ge et al. also reported that patients over 60 years old were more prone to developing vascular tortuosity, and ages were positively correlation with vascular tortuosity [13]. These findings were consistent with the results in our study that being female and at an advanced age were independent risk factors for arteries tortuosity. Regarding vascular risk factors, we found that the tortuosities of EICA and EVA significantly increased in patients with HP, DM, and CHD. Multivariate logistic regression analysis showed that HP was an independent predictor of coronary tortuosity [14]. In addition, the correlations between DM, CHD, and other factors and vascular tortuosity had also been confirmed by research reports [15, 16], supporting the conclusion of this study.
The primary focus of this study was to investigate the relationship between vascular tortuosity and cognitive impairment. It found that the tortuosities of both EICA and EVA were correlated with cognitive impairment scores, the decreased visual-spatial ability was correlated with increased tortuosity of the right EICA, and decreased memory was correlated with increased EVA tortuosity. This study was the first to establish the correlation between the score items affecting cognitive impairment and EICA and EVA tortuosities, Hence, pharmacological treatment such as semaglutide (a GLP1 agonists) can be used timely for the patients with mild cognitive impairment that predicted according to the tortuosities, thus a relationship between chronic ischemia caused by vascular artery tortuosity and cognitive impairment has been established. Studies reported that blood vessels reduced blood supply to the brain by kinking, and chronic hypoperfusion might lead to the depletion of synapses and neurotransmission, thus affecting cognitive function [17]. Meanwhile, the abnormal blood vessels generated by prolonging the tortuosities of the EICA or EVA might cause damage to different areas of the brain, resulting in different cognitive impairments [10]. For example, the decreased blood pressure due to blood vessel tortuosity and the shear force acting on the external part might aggravate the tortuosity and distal perfusion disorders, increase blood turbulence, and lead to vascular endothelial damage and atherosclerotic plaque rupture [18]. The presence of carotid plaques in patients with atherosclerosis displayed a significant correlation with the decline in cognitive function, and mean plaque scores were correlated with lower scores on all cognitive tests [19]. The reduced blood flow of branch arteries caused by tortuosity might lead to symptoms such as multiple lacunar infarction and leukoaraiosis [14, 20], which were closely correlated with cognitive impairment. A study by Chen et al. [21] suggested that chronic cerebral ischemia-induced white matter damage resulted in impaired memory in patients with carotid artery tortuosity, which also supported the conclusion of this study. Based on the findings of this study, it was established that cerebrovascular tortuosity is indeed an independent risk factor for cognitive impairment.
Due to observed correlation between vascular tortuosity and cognitive impairment, it becomes highly crucial to analyze the relationship between potential indicators used to evaluate tortuosity and cognitive impairment. In addition to adopting the recognized TI, the correlations between the vascular DD, TD, and AN and cognitive impairment in the bilateral EICA and EVA were also calculated in this study, respectively. The results showed that although the vascular DD and vascular AN were not highly correlated with the MoCA score of cognitive function (0.2
Most risk factors for cerebrovascular tortuosity, such as age, gender, HP, and DM, are correlated with cognitive impairment, which indirectly confirms the relationship between vascular tortuosity and cognitive impairment. The correlation between age and cognitive decline has become a consensus. As age increases, elastase, an important component of the extracellular matrix, gradually degrades and thins the vascular wall [22], resulting in the tortuosity and abnormal shape of blood vessels caused by low blood flow pressure; therefore, the induced chronic cerebral ischemia might be likely to further impact cognitive function through injury to the cerebral frontal lobe [23]. AH is considered a risk factor for cognitive impairment, vascular dementia, and Alzheimer’s disease. Long-term HP may damage the cerebral microcirculation structure and exacerbate cerebrovascular endothelial dysfunction and neurovascular decoupling, thereby impairing the cerebral blood supply and promoting the inflammation and lesions of the neurons [24]. The study by Umegaki et al. [25] suggested that chronic hyperglycemia might cause osmotic damage and oxidative stress, and the formation of the advanced glycation end products might activate harmful microglia. These would all have direct toxic effects on neurons. A study of neuroimaging assessment on the effects of baseline blood glucose on cognitive function and brain structure in Alzheimer’s disease found that subjects who were normal at baseline had less cognitive function decline and overall brain volume loss over 2 years [26]. Pathologically, impaired insulin signaling may lead to the failure of required neuronal glucose uptake. As a key link between type 2 DM and cognitive impairment, the long-term outcome of insulin resistance may include cellular energy exhaustion, elevated blood lipids, and HP [27]. Whether gender affects cognitive function is still inconclusive. However, most studies suggested that vascular tortuosity was more common in female patients, at least in older female patients [28], which might be correlated with the fact that women are more prone to developing morphological changes due to estrogen-induced vasodilation and reduced elasticity. Additionally, this study provided confirmation that female patients had a higher susceptibility to both vascular tortuosity and cognitive impairment. In summary, it was speculated that these identified risk factors could be closely associated with the occurrence of cognitive impairment resulting from tortuosity.
There were some limitations in this study that should be further investigated. First, although CTA and MRI are probably offering a better resolution, doppler sonography should be encouraged to use for the screening of tortuosity, for their more available, cost-effective and non-invasive. Secondly, it failed to analyze the correlation of risk factors such as gender, age, HP, and DM with cognitive score sub-items to clarify the specific cognitive functions that these risk factors might affect. Meanwhile, the bilateral EICA, EVA, and related tortuosity indicators had not been compared and analyzed to judge the impact of each tortuosity indicator on cognitive function and their internal correlation. Nevertheless, the correlation of the EICA and EVA with mild cognitive impairment are established in this study. With the analysis of the risk factors related to tortuosity and cognitive function, the above mentioned results could provide scientific evidences for the etiology and potential diagnosis and treatment of cognitive impairment in future clinical practice.
Conclusion
The relationship between vascular tortuosity and cognitive impairment has been a subject of debate. While previous studies have reported various influencing factors for vascular tortuosity, there remains a dispute regarding the influence of these factors on tortuosity and their correlation with cognitive function. In this study, through examining the cerebral and artery imaging of hospitalized patients of this study’s department, together with evaluating the correlation between vascular morphology and cognitive function and the risk factors, it was found that the TIs of the EICA and EVA were closely correlated with cognitive impairment in patients. Meanwhile, the right EICA and EVA tortuosities were correlated with declined visual-spatial ability and memory. Age, gender, HP, and DM were risk factors for carotid tortuosity and cognitive impairment. The conclusions of this study will provide a basis for the etiological diagnosis of patients with cognitive impairment and help to optimize future therapeutic regimens.
Ethics statement
This study was approved by the Ethics Committee of the First Affiliated Hospital of Bengbu Medical College (No. 2022-194) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Funding
The study was supported by the Natural Science Research Project of Anhui Educational Committee (KJ2021A0728) and the Scientific Research Project of Bengbu Medical College (2021byzd049).
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Author contributions
Conception and design of the research: LY, WDQ, QQL, SLG; Acquisition of data: XXZ, WLY, KW, SLG; Analysis and interpretation of the data: LY, XXZ, WLY, KW; Statistical analysis: XXZ, WLY, KW, SLG; Obtaining financing: LY, QQL; Writing of the manuscript: LY, XXZ, QQL; Critical revision of the manuscript for intellectual content: WDQ, QQL. All authors read and approved the final draft.
Footnotes
Acknowledgments
We would like to acknowledge the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.