
Abstract
BACKGROUND:
Chronic obstructive pulmonary disease (COPD) causes organic damage as well as anxiety, depression, fear, and other psychological disorders, which seriously affect the quality of life and prognosis of patients and cause a huge economic burden to the family and society.
OBJECTIVE:
The aim of this study was to investigate the correlation between an imbalance of serum Th1/Th2 indicators and psychiatric depression in elderly patients with COPD and analyze its implications for clinical management.
METHODS:
From January 2018 to May 2022, 120 elderly patients with COPD treated at our hospital were categorized into two groups based on the self-rating depression scale (SDS): COPD with depression (SDS score
RESULTS:
Compared with the group without depression, the partial pressure of carbon dioxide and COPD assessment test scores were significantly higher, and the oxygenation index, forced expiratory volume in one second (FEV1), and percent predicted FEV1 were significantly lower in the COPD with depression group (
CONCLUSION:
Elderly patients with COPD and depression had reduced pulmonary function and higher serum Th1/Th2 levels, and an imbalance in serum Th1/Th2 indicators was a potential risk factor for depression. Moreover, elderly patients with COPD and depression were at a higher risk of disease progression and had a worse prognosis. Thus, an imbalance in serum Th1/Th2 indicators is a potential prognostic factor for evaluating depression in patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) affects 8.6% of the Chinese population. The prevalence of COPD is 13.7% in individuals aged
Helper T cells secrete cytokines, where Th1 mediates cellular immunity and Th2 mediates humoral immunity [5, 6]. Th1/Th2 is in dynamic balance; pathogen invasion causes a disturbance in the Th1/Th2 ratio, leading to cellular or humoral immunity (Th1/Th2 imbalance) followed by the secretion of inhibitory cytokines [7, 8]. The levels of serum Th1/Th2 cytokines (interleukin [IL]-1
Psychological questionnaires are widely used to evaluate depressive symptoms. However, some respiratory symptoms in elderly patients with COPD often overlap with depressive symptoms on psychological questionnaires. In addition, elderly patients with COPD have varying degrees of hearing and comprehension loss; therefore, completing a psychological questionnaire may be difficult for these patients. Nevertheless, combined with serological indicators for diagnosis, psychological questionnaires are conducive to early diagnosis of COPD complicated by depression and greatly improve clinical efficiency [15].
Systemic inflammation caused by COPD can lead to elevated levels of systemic inflammatory markers, resulting in an imbalance in serum Th1/Th2 indicators [16]. Serum Th1/Th2 indicators are also noticeably elevated in the serum of patients with clinical and subclinical depression [17, 18]. The serum Th1/Th2 ratio may be involved in the pathogenesis of depression through elevated cytokine levels, thereby reducing the synthesis of 5-hydroxytryptamine, which is an important mechanism of depression [19]. This pathway produces neurotoxic metabolites that can lead to depression [19]. In addition, inflammatory cytokines persist for a long time, leading to hyperactivity of the hypothalamus-pituitary-adrenal axis and glucocorticoid resistance [20]. The inflammatory cytokines IL-1
Materials and methods
General information
From January 2018 to May 2022, 120 elderly patients with COPD treated at our hospital were classified into two groups based on the self-rating depression scale (SDS): COPD with depression (SDS
The 46 men and 19 women in the COPD without depression group (
The inclusion criteria were: (1) a clear diagnosis of COPD that met the diagnostic criteria of the Global COPD Initiative (GOLD) guidelines version 2017 [23]; (2) age
The exclusion criteria were: (1) massive pleural effusion, pneumothorax, and the inability to tolerate a 6 min walking distance or lung function test; (2) mental and psychological disorders such as anxiety and depression diagnosed before the diagnosis of COPD; (3) severe hepatorenal insufficiency, severe cardiovascular disease, neuromuscular disease, cerebral infarction, sequelae of cerebral hemorrhage, or solid or hematological tumors; (4) other chronic respiratory diseases such as active tuberculosis, pulmonary embolism, and chronic thrombotic pulmonary hypertension; and (5) Alzheimer’s disease, language communication disorder, and limb movement disorder.
Observation index
COPD assessment test (CAT) score
The CAT score was used to evaluate the impact of COPD on the patient’s health and quality of life and included eight questions [25]. The CAT score ranged from 0–40 points: 0–10 was considered “mildly affected,” and 11–20 points and 21–30 points were defined as “very serious impact.” The CAT score was calculated on the first day after admission.
Prognostic evaluation index
The prognosis of patients was evaluated using modified clinically noticeable deterioration (CID-C), specifically by detecting lung function, health status, and early deterioration to evaluate disease deterioration and prognosis [26]. The criteria for CID-C included at least one of the following: (1) after the use of bronchodilators, forced expiratory volume in one second (FEV1) decreased by more than 100 mL compared with baseline; (2) the CAT score was elevated by more than two points compared with baseline; and (3) moderate or severe exacerbations. The patients were followed-up by telephone at 1, 3, and 6 months after discharge, and the interval before the first occurrence of CID-C and the frequency of CID-C occurrence within 6 months was collected.
Serum Th1/Th2 index detection
Within 24 h of admission, 5 mL of venous blood was collected from patients on an empty stomach and centrifuged at 3000 RPM for 10 min. The supernatant was stored in the refrigerator at
Arterial blood gas analysis
For arterial blood analyses, 2 mL of arterial blood was collected immediately on the first day after admission. Arterial blood gas analysis was performed using a blood gas analyzer. The partial pressure of oxygen (PO
Pulmonary function test
Pulmonary function tests were performed during the stable phase of COPD (approximately three months). For the test, patients inhaled 400
Statistical analysis
Excel was used for data management, and data were analyzed and processed using SPSS 24.0 statistical software. Data with normal distribution and uniform variance are expressed as mean
Results
Comparison of clinical indices
In terms of clinical indicators, compared with the group without depression, the PCO
Comparison of clinical information
Comparison of clinical information
As shown in Table 2, IL-1
Comparison of serum Th1/Th2 indicators
Comparison of serum Th1/Th2 indicators
As shown in Table 3, logistic regression analysis indicated that an imbalance in serum Th1/Th2 indicators (IL-1
Logistic regression analysis of risk factors for mental depression in elderly patients with COPD
Logistic regression analysis of risk factors for mental depression in elderly patients with COPD
Serum Th1/Th2 indices (IL-1
Diagnosis value of depression in elderly patients with COPD
Diagnosis value of depression in elderly patients with COPD
The ROC curves for the diagnosis of depression in patients with COPD. (A) IL-1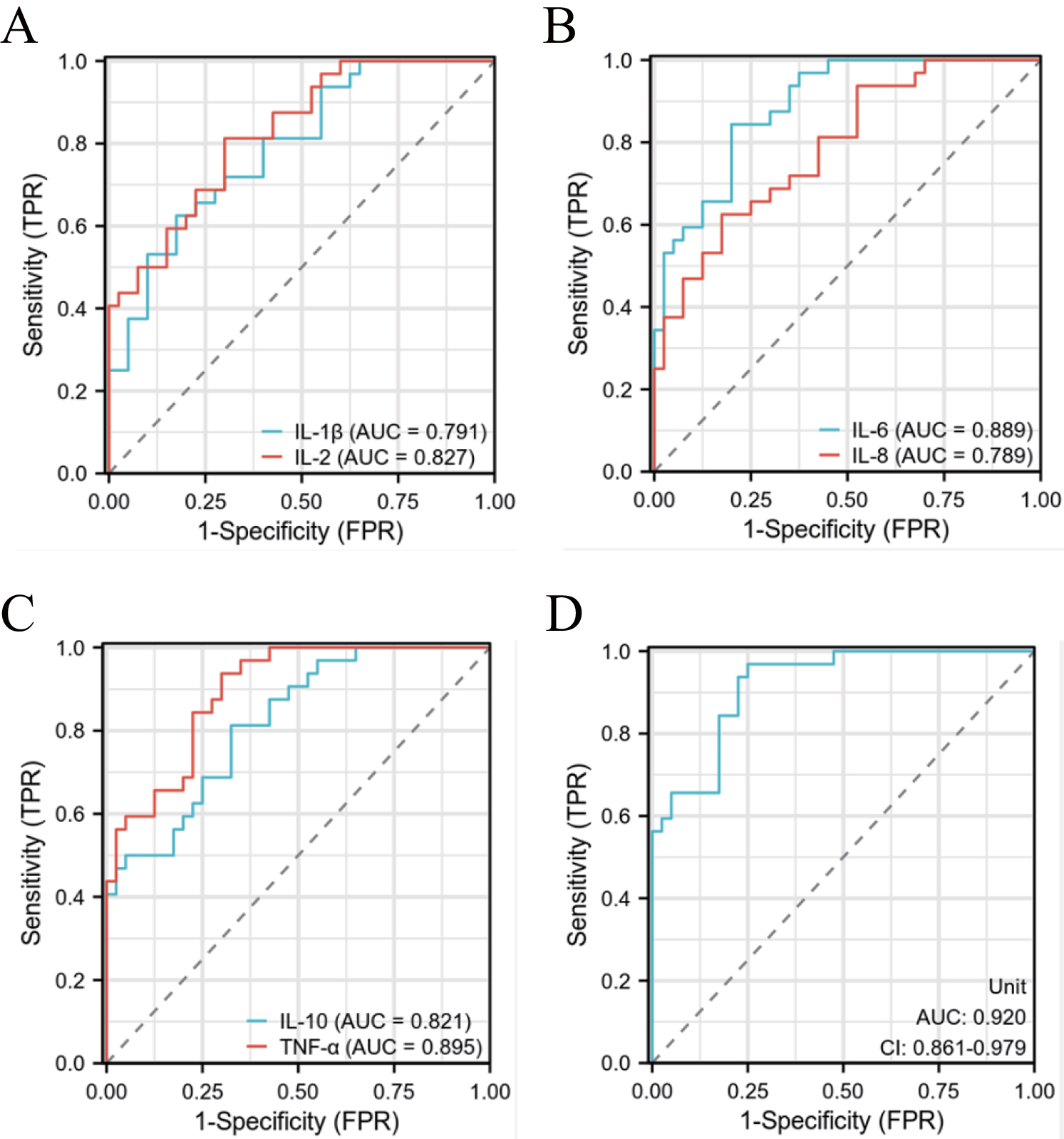
One, three, and six months after discharge, telephone calls were made to follow-up with patients. The interval before the first occurrence of CID-C and the frequency of CID-C within six months after discharge were recorded, and these prognostic indices were compared between the two groups. The interval before the first onset of CID-C in the COPD with depression group was noticeably shorter than that in the group without depression. The incidence of CID-C within 6 months in the COPD with depression group was noticeably higher than in the group without depression (
Comparison of prognostic index
Comparison of prognostic index
Pearson correlation analysis indicated that serum Th1/Th2 indicators (IL-1
Correlation between serum Th1/Th2 and the prognosis of elder COPD with depression
Correlation between serum Th1/Th2 and the prognosis of elder COPD with depression
COPD is characterized by chronic inflammation that occurs in the peripheral airways and pulmonary parenchyma. Various cytokines are released during the progression of inflammation, and the concentration of serum inflammatory cytokines, including IL-6, C-reactive protein (CRP), and TNF-
In cases of infection or stress, changes in cytokine levels reflect the inflammatory state of the body to a certain extent. During infection, the balance between pro-inflammatory and anti-inflammatory factors is disrupted, alternating between the two, which noticeably affects the development, direction, and outcome of the infection. Helper T lymphocytes secrete various cytokines, assist cytotoxic T cells and B lymphocytes, and play an active role in immune responses [36]. At present, they are mainly divided into four subtypes, Th0, Th1, Th2, and Th3, according to the types of cytokines secreted. Among these, Th1 cells are involved in stimulating the cellular immune response, promoting proinflammatory responses, whereas Th2 cells are involved in mediating the humoral immune response promoting anti-inflammatory responses [37]. The imbalances in Th1/Th2 and the secretion of related cytokines has been shown to lead to immune inflammatory damage [38]. The secretion of Th2 cytokines is noticeably elevated in pulmonary diseases, and the dominant response is Th2, indicating that immune function is suppressed and the ability to eliminate pathogens is decreased. Th1 cells are involved in mediating the cellular immune response by inhibiting, lysing, and destroying killer cells through the secretion of TNF-
During the inflammatory response, TNF-
As an important cell growth factor, IL-2 promotes the activation and proliferation of T cells, promotes the lethality of T cells, and improves immune responses, such as natural killer cell activity and antibody secretion by B cells. Studies have shown that patients with low cellular immune function complicated by COPD can be treated with recombinant IL-2 or genetically cloned IL-2.
Th2 cells participate in the humoral immune response mainly by secreting IL-4, IL-6, IL-10, and other cytokines to produce corresponding antibodies [42, 43]. The upregulation of IL-4 expression in patients with pulmonary disease can reflect the extent of the local inflammatory response and the rate of inflammatory development, and thus may be involved in the occurrence and progression of pulmonary diseases. It is possible that IL-6 is produced first upon infection and inflammation, with its levels increasing rapidly in a short period (approximately 1–2 hours). IL-6 can enhance the function of natural killer cell lysis and promote the regulation of inflammatory responses. It is a sensitive index for the early diagnosis of acute infections and is more sensitive than PCT and CRP [44]. Moreover, an increase in IL-6 levels is associated with the severity of infection and can be used to evaluate the severity and prognosis of infection. In addition to its multifunctional negative regulatory role, IL-10 is one of the primary anti-inflammatory factors in the body. It can participate in the biological regulation of immune, inflammatory, tumor, and other cells and block the molecular pathway of Th1/Th2 to produce TNF-
The comparison of clinical indicators revealed that the PCO
This study has several limitations. This is a retrospective study, with certain associated risks of bias. The sample size was small and subsequent larger multicenter clinical studies are warranted. Moreover, the clinical follow-up time was short, and long-term clinical follow-ups should be conducted. With the ongoing exploration of the relationship between serum Th1/Th2 imbalance and depression in elderly patients with COPD, a research direction of interest is to develop an artificial intelligence tool to assist in the diagnosis of depression in elderly patients with COPD. A telemetry system was developed to diagnose asthma and COPD [53], and other studies have investigated the use of various artificial intelligence systems and machine learning models in the diagnosis of various diseases [52, 54, 55, 56, 57, 58]. We anticipate that an artificial intelligence tool could assist patients with better self-management and enable physicians to rapidly diagnose depression in elderly patients with COPD, monitor patient health status, and potentially provide appropriate professional care or treatment.
Conclusion
Elderly patients with COPD and depression had reduced pulmonary function and higher serum Th1/Th2 levels; moreover, serum Th1/Th2 imbalance was a potential risk factor for depression in elderly patients with COPD. Elderly patients with COPD and depression were at a higher risk of disease progression and had a worse prognosis. Thus, an imbalance in serum Th1/Th2 indicators may have prognostic potential for evaluating depression in patients with COPD.
Footnotes
Conflict of interest
None to report.